




Frontline healthcare workers (F-HCWs) are at the forefront of medical care providers against the novel coronavirus 2019 (COVID-19) pandemic which has life-threatening potentials. Inadequate knowledge and incorrect attitudes among HCWs can directly influence practices and lead to delayed diagnosis, poor infection control practices, and spread of disease.
ObjectivesThe aim of this study was to assess the knowledge, attitude and practice (KAP) regarding the COVID-19 pandemic among the frontline healthcare workers (F-HCWs) working at a tertiary care hospital situated in eastern Uttar Pradesh and to identify the factors significantly associated with KAP.
MethodsA cross-sectional study was conducted among 260 health care providers across eastern Uttar Pradesh including Basti city during December 2020. Data was collected using a self-primed pretested questionnaire from the FHCWs working at a tertiary care hospital of eastern Uttar Pradesh. In this survey, a convenience sampling method was adopted. 12 items on knowledge, 10 items on attitude, and 5 items on practices related to COVID-19. The other variables consisted of 4 items on socio-demographic attributes, p-value and 95% confidence intervals (CIs) were performed to assess the attitude and practices in relation to knowledge.
ResultsOf the total 260 study population, 228 were interviewed online, 32 were self-administered. Knowledge and attitude of the nursing staff were highest but practice score was best for residents. Among different age groups knowledge, attitude and practices scores were highest for 35–45, 45–60 and 25–35 age groups respectively. Respondents having 5–10 years of experience had the best knowledge and the attitude score was highest for HCWs having 10–20 years’ experience but the practice score was higher for HCWs having more than 20 years’ work experience. Overall knowledge score of respondents having strong correlation with attitude (p<0.05) and to the practice (p<0.05).
ConclusionIn this survey many F-HCWs reported adequate overall knowledge with a positive attitude and adopted appropriate practices. The F-HCWs with a higher level of education and more years of experience in health care facilities had better KAP towards COVID-19.
Los trabajadores de la salud de primera línea (F-HCW) están a la vanguardia de los proveedores de atención médica contra la pandemia del nuevo coronavirus 2019 (COVID-19), que tiene un potencial mortal. El conocimiento inadecuado y las actitudes incorrectas entre los trabajadores sanitarios pueden influir directamente en las prácticas y llevar a un diagnóstico tardío, prácticas deficientes de control de infecciones y propagación de enfermedades.
ObjetivosEl objetivo de este estudio fue evaluar el conocimiento, la actitud y la práctica (CAP), con respecto a la pandemia de COVID-19 entre los trabajadores de atención médica de primera línea (TS-TS) que trabajan en un hospital de atención terciaria situado en el este de Uttar Pradesh e identificar la factores asociados significativamente con CAP.
MétodosSe realizó un estudio transversal entre 260 proveedores de atención médica en el este de Uttar Pradesh, incluida la ciudad de Basti, durante diciembre de 2020. Los datos se recopilaron utilizando un cuestionario autocebante previamente probado de los trabajadores sanitarios de salud que trabajan en un hospital de atención terciaria del este de Uttar Pradesh. En esta encuesta, se adoptó un método de muestreo por conveniencia. Doce ítems sobre conocimientos, 10 ítems sobre actitud y cinco ítems sobre prácticas relacionadas con COVID-19. Las otras variables consistieron en cuatro ítems sobre atributos sociodemográficos, valor de p e intervalos de confianza (IC) del 95%, que se realizaron para evaluar la actitud y las prácticas en relación con el conocimiento.
ResultadosDel total de 260 habitantes del estudio, 228 fueron entrevistados en línea, 32 fueron autoadministrados. El conocimiento y la actitud del personal de enfermería fueron los más altos, pero la puntuación de la práctica fue la mejor para los residentes. Entre los diferentes grupos de edad, los puntajes de conocimientos, actitudes y prácticas fueron los más altos para los grupos de edad de 35 a 45, 45 a 60 y 25 a 35 años, respectivamente. Los encuestados que tenían entre cinco y 10 años de experiencia tenían el mejor conocimiento y el puntaje de actitud era más alto para los TS que tenían entre 10 y 20 años de experiencia, pero el puntaje de práctica era más alto para los TS que tenían más de 20 años de experiencia laboral. Puntaje de conocimiento general de los encuestados que tiene una fuerte correlación con la actitud (p < 0,05) y con la práctica (p < 0,05).
ConclusiónEn esta encuesta, muchos trabajadores sanitarios F informaron un conocimiento general adecuado con una actitud positiva y adoptaron prácticas apropiadas. Los PS-M con un mayor nivel de educación y más años de experiencia en establecimientos de salud tuvieron mejor CAP hacia COVID-19.
Coronavirus disease 2019, known as COVID-19 is an extremely expanding pandemic caused by a severe acute respiratory syndrome coronavirus (SARS-CoV-2), an enveloped single-stranded RNA virus, previously known as 2019-nCov.1–3 SARS-COV-2 is transmitted from person to person by close contact (within about 6 feet) via the respiratory secretions (droplets) in coughs or sneezes or by touching virus-contaminated surfaces or objects. Due to the rapid spread of this highly transmissible virus, the disease rapidly spread all over the world affecting more than 176 million peoples and more than 3.8 million deaths. As of 15 June 2021 more than 2.3 billion vaccines have been administered.4 COVID-19 is characterized by flu-like symptoms and may also pose fatal respiratory problems. Old age and the pre-existence of chronic illnesses have been identified as potential risk factors for severe disease and mortality.5 The virus incubation period is 2–14 days with the majority of patients (80%) having mild symptoms that do not require medical intervention.6 Until now there is no specific antiviral curative treatment that has been recommended for COVID-19. Many vaccines have been developed and being administered on large scale to healthcare workers and general public. Vaccines authorized for emergency use by USFDA are Pfizer-BioNTech COVID-19 vaccine, Moderna COVID-19 vaccine, and Janssen COVID-19 vaccine. Other vaccines that are under WHO Emergency Use Listing (EUL) are SII/Covishield, AstraZeneca/AZD1222 vaccines, and Sinopharm COVID-19 vaccine. COVAXIN (India) is also being administered but is not under EUL.7
The HCWs are at the frontline of COVID-19 pandemic defense and are exposed not only to infection with COVID-19 due to their frequent exposure to infected individuals, but they also suffer psychological distress, long working hours, fatigue, occupational stigma and many times may encounter physical violence.8,9 Knowledge of any infectious agent, its mode and route of transmission plays crucial role in planning and executing infection control. The inadequate knowledge and incorrect attitudes among HCWs can directly influence their practices and lead to delayed diagnosis, poor infection control practices, and spread of the disease.10,11
Understanding HCWs’ knowledge, attitudes, and possible perception of risk of infection help to predict and correlate the outcomes of COVID-19. The purpose of the study was to evaluate the knowledge, attitude, and perception (KAP) of the risk of infection with COVID-19 among HCWs in eastern Uttar Pradesh India.
Materials and methodsSettings and study populationA total of 260 participants gave consent to participate in this online web-based survey. This study was conducted to assess the status of health care workers’ KAP related to COVID-19 during the COVID-19 pandemic. We conducted a cross-sectional study based on the health care population at our institution.
Sample size and sampling techniqueConsidering the special situation, it was not possible to conduct a full community-based study with a representative sample. Thus the study focused only on HCWs and a sampling technique of convenience was adopted to obtain the desired information for the study.
Data collectionData was collected using a structured questionnaire. The questionnaire was put together or drawn up in English and Hindi language. It was pre-tested among a cross-section of participants to ensure the clarity of questions and to eliminate any ambiguity.
Design of the questionsThe questionnaire included socio-demographic characteristics like age group, marital status, profession, and years of experience in healthcare services. The name and gender were excluded to maintain anonymity. The other variables were knowledge, attitudes and practices related to COVID-19 and its prevention and control. The questions mainly focused on HCWs’ knowledge of hospital infection control practices. Some questions were designed to assess the knowledge of the mode and route of transmission of SARS-CoV-2. Questions related to misconceptions about food habit and COVID-19 were adopted from WHO's document,12 questions related to child isolation from mother were included based on general query of population and few questions were formulated to assess the stigma towards COVID-19 patients. At the beginning of the year 2020, there were misconceptions of the existence of SARS-CoV-2, therefore one question of knowledge was included to know whether the HCWs believe this real threat. The attitude questionnaire was designed to assess behaviour towards COVID-19 positive patient, hand washing and social distancing in preventing the disease. The practice parameters covered the quotient of worry if one happens to contact the COVID-19 positive patient, frequency of handwashing, use of disinfectants and maintaining social distancing. The knowledge was assessed by 12 factual statements, practice by 10 and 5 questions were related to practice.
Based on 80–100% correct answer for each question, it was considered as appropriate knowledge, and below 80.0% was considered as inappropriate knowledge. Similarly, attitudes and practices were also categorized.
Statistical analysisThe categorical variables were described as numbers (%) and 95% confidence intervals (CIs). The continuous variables were presented using means. All statistical analyses were performed using SPSS.26 version; p<0.05 (two-tailed) was considered statistically significant.
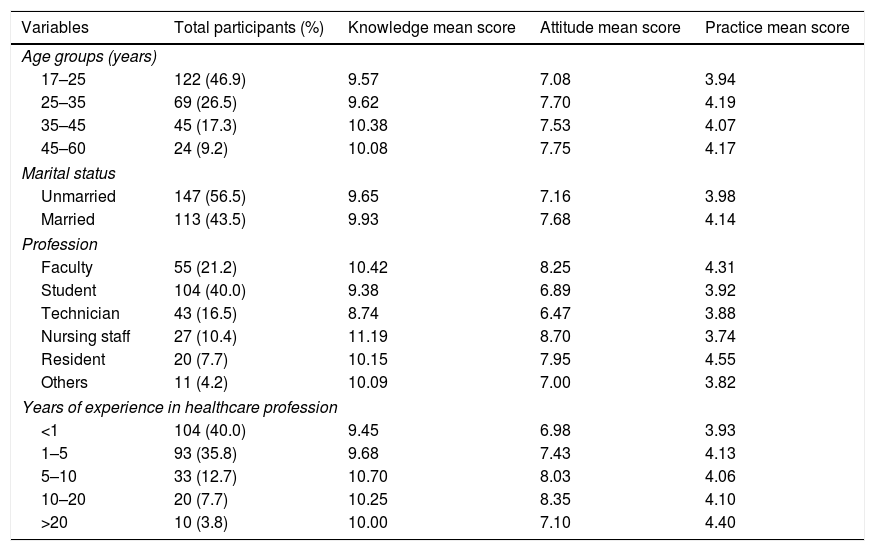
ResultsCharacteristics of the study populationA total of 260 participants were interviewed in this cross-sectional study. Of the study population, 46.9% belonged to the young age (17–25 years) group, followed by the 25–35 age group (26.5%), 35–45 age group (17.3%) and participants of age more than 45 years were 9.2%. Among all participants, 56.5% were married. The majority of participants were medical students (40%) followed by medical faculty (21.2%), technicians (16.5%), nursing staff (10.4%), residents (7.7%) and others (4.2%) (Table 1).
Demographic characteristics of health care workers.
| Variables | Total participants (%) | Knowledge mean score | Attitude mean score | Practice mean score |
|---|---|---|---|---|
| Age groups (years) | ||||
| 17–25 | 122 (46.9) | 9.57 | 7.08 | 3.94 |
| 25–35 | 69 (26.5) | 9.62 | 7.70 | 4.19 |
| 35–45 | 45 (17.3) | 10.38 | 7.53 | 4.07 |
| 45–60 | 24 (9.2) | 10.08 | 7.75 | 4.17 |
| Marital status | ||||
| Unmarried | 147 (56.5) | 9.65 | 7.16 | 3.98 |
| Married | 113 (43.5) | 9.93 | 7.68 | 4.14 |
| Profession | ||||
| Faculty | 55 (21.2) | 10.42 | 8.25 | 4.31 |
| Student | 104 (40.0) | 9.38 | 6.89 | 3.92 |
| Technician | 43 (16.5) | 8.74 | 6.47 | 3.88 |
| Nursing staff | 27 (10.4) | 11.19 | 8.70 | 3.74 |
| Resident | 20 (7.7) | 10.15 | 7.95 | 4.55 |
| Others | 11 (4.2) | 10.09 | 7.00 | 3.82 |
| Years of experience in healthcare profession | ||||
| <1 | 104 (40.0) | 9.45 | 6.98 | 3.93 |
| 1–5 | 93 (35.8) | 9.68 | 7.43 | 4.13 |
| 5–10 | 33 (12.7) | 10.70 | 8.03 | 4.06 |
| 10–20 | 20 (7.7) | 10.25 | 8.35 | 4.10 |
| >20 | 10 (3.8) | 10.00 | 7.10 | 4.40 |
In the analysis of the different variables, age group 35–45 have the highest knowledge mean score was 10.38, by profession nursing staff have highest knowledge mean score was 11.19 followed by faculty which was 10.42 and by the year of experience in the healthcare profession, HCWs with 5–10 years of experience have the highest knowledge mean score of 10.70 (Table 1).
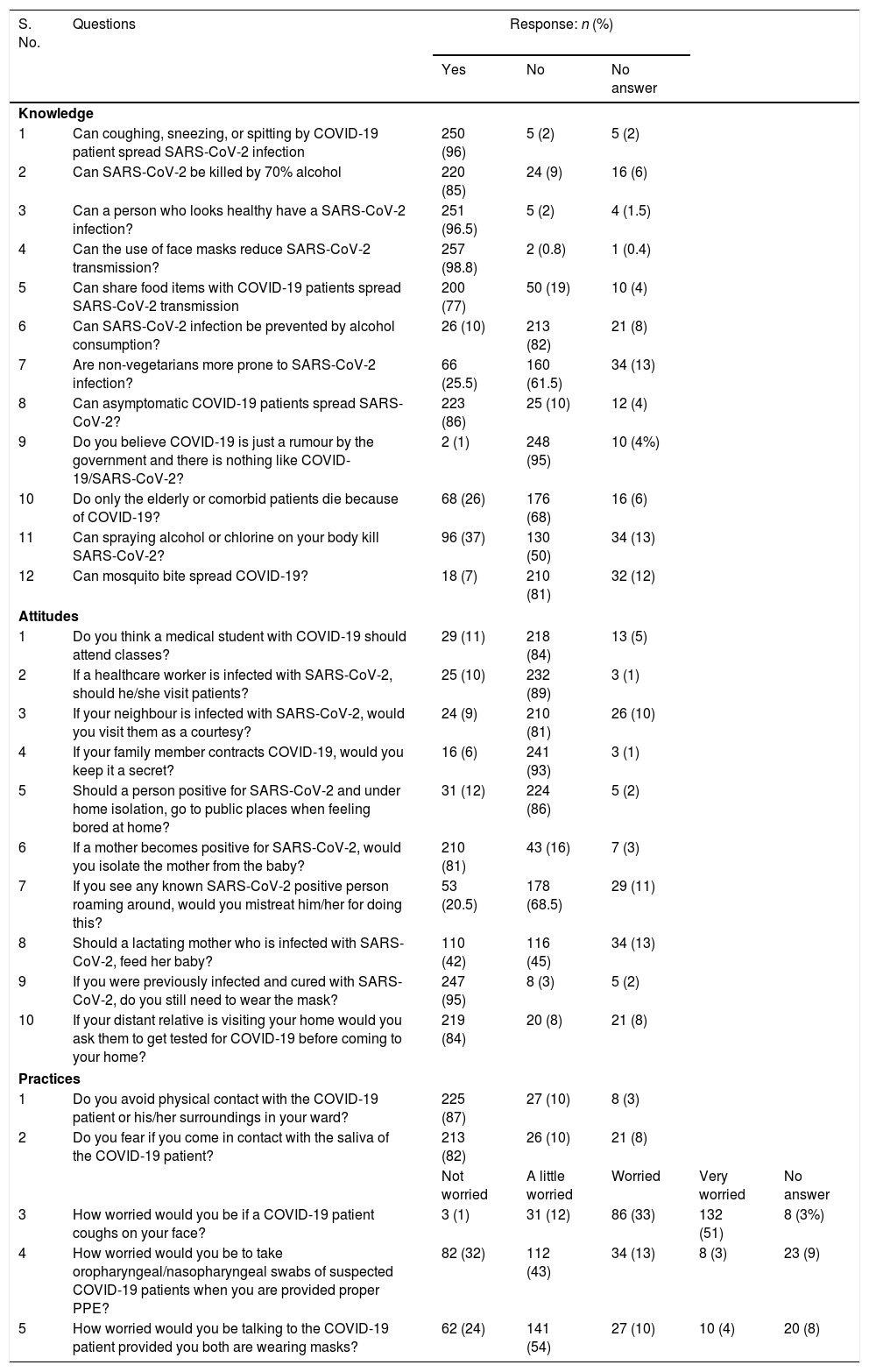
Most knowledge questions had a high accuracy rate (>85%). For example, 250 (96%) respondents agreed that coughing, sneezing, or spitting by COVID-19 patient spread SARS-CoV-2 infection, and most respondents agreed that using alcohol-based hand sanitizers are effective against SARS-CoV-2 (220; 84%) and using face mask (257; 99%) can prevent COVID-19 infection. However, among all 260 respondents, only 10 (4%) disagreed that coughing, sneezing, or spitting by COVID-19 patient spread SARS-CoV-2 infection, only 9 (4%) disagreed that a person who looks healthy can have a SARS-CoV-2 infection and only 37 (14%) disagreed that asymptomatic COVID-19 patients spread SARS-CoV-2 (Table 2).
Analysis of knowledge, attitude and practice among HCWs towards COVID-19.
| S. No. | Questions | Response: n (%) | ||||
|---|---|---|---|---|---|---|
| Yes | No | No answer | ||||
| Knowledge | ||||||
| 1 | Can coughing, sneezing, or spitting by COVID-19 patient spread SARS-CoV-2 infection | 250 (96) | 5 (2) | 5 (2) | ||
| 2 | Can SARS-CoV-2 be killed by 70% alcohol | 220 (85) | 24 (9) | 16 (6) | ||
| 3 | Can a person who looks healthy have a SARS-CoV-2 infection? | 251 (96.5) | 5 (2) | 4 (1.5) | ||
| 4 | Can the use of face masks reduce SARS-CoV-2 transmission? | 257 (98.8) | 2 (0.8) | 1 (0.4) | ||
| 5 | Can share food items with COVID-19 patients spread SARS-CoV-2 transmission | 200 (77) | 50 (19) | 10 (4) | ||
| 6 | Can SARS-CoV-2 infection be prevented by alcohol consumption? | 26 (10) | 213 (82) | 21 (8) | ||
| 7 | Are non-vegetarians more prone to SARS-CoV-2 infection? | 66 (25.5) | 160 (61.5) | 34 (13) | ||
| 8 | Can asymptomatic COVID-19 patients spread SARS-CoV-2? | 223 (86) | 25 (10) | 12 (4) | ||
| 9 | Do you believe COVID-19 is just a rumour by the government and there is nothing like COVID-19/SARS-CoV-2? | 2 (1) | 248 (95) | 10 (4%) | ||
| 10 | Do only the elderly or comorbid patients die because of COVID-19? | 68 (26) | 176 (68) | 16 (6) | ||
| 11 | Can spraying alcohol or chlorine on your body kill SARS-CoV-2? | 96 (37) | 130 (50) | 34 (13) | ||
| 12 | Can mosquito bite spread COVID-19? | 18 (7) | 210 (81) | 32 (12) | ||
| Attitudes | ||||||
| 1 | Do you think a medical student with COVID-19 should attend classes? | 29 (11) | 218 (84) | 13 (5) | ||
| 2 | If a healthcare worker is infected with SARS-CoV-2, should he/she visit patients? | 25 (10) | 232 (89) | 3 (1) | ||
| 3 | If your neighbour is infected with SARS-CoV-2, would you visit them as a courtesy? | 24 (9) | 210 (81) | 26 (10) | ||
| 4 | If your family member contracts COVID-19, would you keep it a secret? | 16 (6) | 241 (93) | 3 (1) | ||
| 5 | Should a person positive for SARS-CoV-2 and under home isolation, go to public places when feeling bored at home? | 31 (12) | 224 (86) | 5 (2) | ||
| 6 | If a mother becomes positive for SARS-CoV-2, would you isolate the mother from the baby? | 210 (81) | 43 (16) | 7 (3) | ||
| 7 | If you see any known SARS-CoV-2 positive person roaming around, would you mistreat him/her for doing this? | 53 (20.5) | 178 (68.5) | 29 (11) | ||
| 8 | Should a lactating mother who is infected with SARS-CoV-2, feed her baby? | 110 (42) | 116 (45) | 34 (13) | ||
| 9 | If you were previously infected and cured with SARS-CoV-2, do you still need to wear the mask? | 247 (95) | 8 (3) | 5 (2) | ||
| 10 | If your distant relative is visiting your home would you ask them to get tested for COVID-19 before coming to your home? | 219 (84) | 20 (8) | 21 (8) | ||
| Practices | ||||||
| 1 | Do you avoid physical contact with the COVID-19 patient or his/her surroundings in your ward? | 225 (87) | 27 (10) | 8 (3) | ||
| 2 | Do you fear if you come in contact with the saliva of the COVID-19 patient? | 213 (82) | 26 (10) | 21 (8) | ||
| Not worried | A little worried | Worried | Very worried | No answer | ||
| 3 | How worried would you be if a COVID-19 patient coughs on your face? | 3 (1) | 31 (12) | 86 (33) | 132 (51) | 8 (3%) |
| 4 | How worried would you be to take oropharyngeal/nasopharyngeal swabs of suspected COVID-19 patients when you are provided proper PPE? | 82 (32) | 112 (43) | 34 (13) | 8 (3) | 23 (9) |
| 5 | How worried would you be talking to the COVID-19 patient provided you both are wearing masks? | 62 (24) | 141 (54) | 27 (10) | 10 (4) | 20 (8) |
In the different variables, age group 45–60 have more positive attitude mean score was 7.75, by profession nursing staff have more positive attitude mean score of 8.70 followed by faculty which was 8.25 and by the year of experience in the healthcare profession, 10–20 years of experience have a more positive attitude, and the mean score was 8.35 (Table 1).
Among all 260 respondents, 232 (89%) agreed that if a healthcare worker is infected with SARS-CoV-2, he/she should not visit patients, and 247 (95%) agreed that if you were previously infected and cured of SARS-CoV-2, they still need to wear the mask, however, only 13 (5%) disagreed that if one was previously infected and cured with SARS-CoV-2, still need to wear the mask (Table 2).
PracticesThe different variables analysis age group 25–35 have a practice mean score of 4.19, however, professional residents have a more appropriate practice mean score of 4.55 and by the year of experience in the healthcare profession, >20 years of experience have a better practice mean score which was 4.40 (Table 1). In terms of COVID-19 related practices, 87% of health care workers avoided physical contacts when providing care/services to suspected or positive COVID-19 patients, 82% HCWs feared if come in contact with saliva of COVID-19 patients, 84% HCWs were worried or very worried if a COVID-19 patients coughs on their face, 75% HCWs either not worried or a little worried for patient's sampling if they are provided proper PPE, and 78% HCWs were little or not worried while talking to a COVID-19 patient while wearing mask (Table 2).
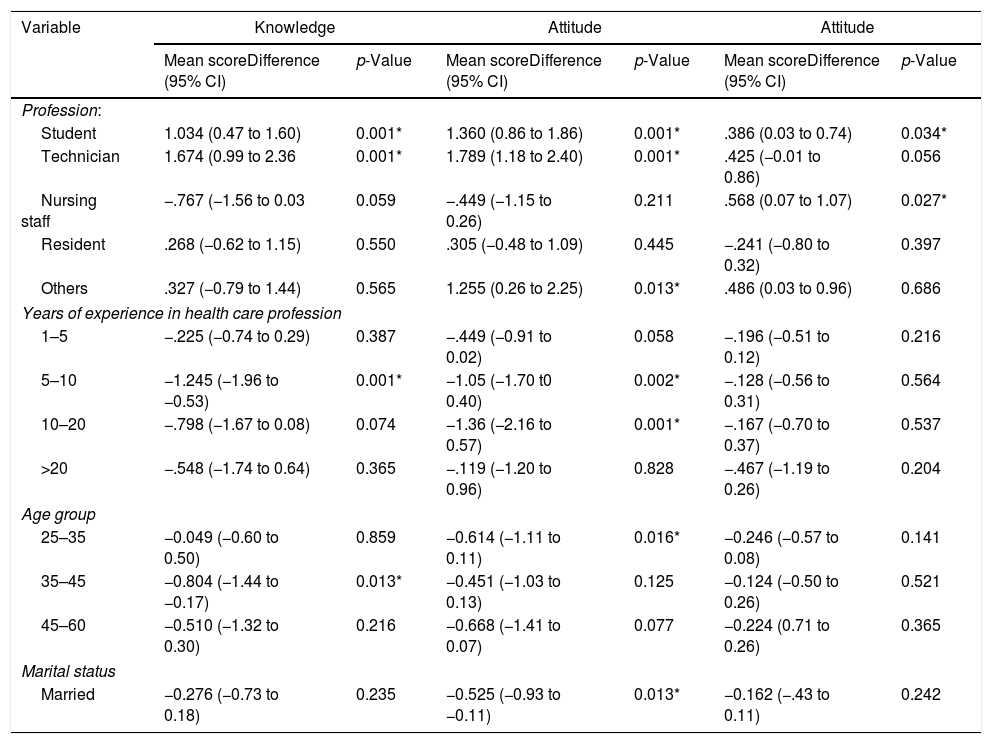
Factors associated with knowledge, attitudes, and practices regardingCOVID-19A multivariate linear regression analysis was carried out to determine association between sociodemographic characteristics and mean knowledge, attitude and practice scores, after controlling for other variables. In comparison to faculty, the youngest respondents mainly students (17–25 years) had least knowledge score (mean=1.034, 95% CI=0.47–1.60, p<0.001), attitude (mean=1.360, 95% CI=0.862–1.86, p<0.001), practice (mean=0.386, 95% CI=0.03–0.74, p 0.034). In addition, nurses had significantly higher practice score compared to technicians (mean=0.568, 95% CI=0.07–1.07, p 0.027). While respondents with faculty levels had statistically significant knowledge of COVID-19 practices related to COVID-19 residents respondents score was noted higher in comparison to others included in this study (Table 3).
Associations between socio-demographic characteristics and mean knowledge, attitude and practice scores.
| Variable | Knowledge | Attitude | Attitude | |||
|---|---|---|---|---|---|---|
| Mean scoreDifference (95% CI) | p-Value | Mean scoreDifference (95% CI) | p-Value | Mean scoreDifference (95% CI) | p-Value | |
| Profession: | ||||||
| Student | 1.034 (0.47 to 1.60) | 0.001* | 1.360 (0.86 to 1.86) | 0.001* | .386 (0.03 to 0.74) | 0.034* |
| Technician | 1.674 (0.99 to 2.36 | 0.001* | 1.789 (1.18 to 2.40) | 0.001* | .425 (−0.01 to 0.86) | 0.056 |
| Nursing staff | −.767 (−1.56 to 0.03 | 0.059 | −.449 (−1.15 to 0.26) | 0.211 | .568 (0.07 to 1.07) | 0.027* |
| Resident | .268 (−0.62 to 1.15) | 0.550 | .305 (−0.48 to 1.09) | 0.445 | −.241 (−0.80 to 0.32) | 0.397 |
| Others | .327 (−0.79 to 1.44) | 0.565 | 1.255 (0.26 to 2.25) | 0.013* | .486 (0.03 to 0.96) | 0.686 |
| Years of experience in health care profession | ||||||
| 1–5 | −.225 (−0.74 to 0.29) | 0.387 | −.449 (−0.91 to 0.02) | 0.058 | −.196 (−0.51 to 0.12) | 0.216 |
| 5–10 | −1.245 (−1.96 to −0.53) | 0.001* | −1.05 (−1.70 t0 0.40) | 0.002* | −.128 (−0.56 to 0.31) | 0.564 |
| 10–20 | −.798 (−1.67 to 0.08) | 0.074 | −1.36 (−2.16 to 0.57) | 0.001* | −.167 (−0.70 to 0.37) | 0.537 |
| >20 | −.548 (−1.74 to 0.64) | 0.365 | −.119 (−1.20 to 0.96) | 0.828 | −.467 (−1.19 to 0.26) | 0.204 |
| Age group | ||||||
| 25–35 | −0.049 (−0.60 to 0.50) | 0.859 | −0.614 (−1.11 to 0.11) | 0.016* | −0.246 (−0.57 to 0.08) | 0.141 |
| 35–45 | −0.804 (−1.44 to −0.17) | 0.013* | −0.451 (−1.03 to 0.13) | 0.125 | −0.124 (−0.50 to 0.26) | 0.521 |
| 45–60 | −0.510 (−1.32 to 0.30) | 0.216 | −0.668 (−1.41 to 0.07) | 0.077 | −0.224 (0.71 to 0.26) | 0.365 |
| Marital status | ||||||
| Married | −0.276 (−0.73 to 0.18) | 0.235 | −0.525 (−0.93 to −0.11) | 0.013* | −0.162 (−.43 to 0.11) | 0.242 |
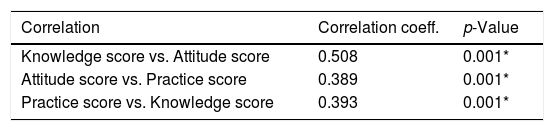
Positive linear correlations were noted between knowledge and attitude (r=0.508), attitude and practice (r=0.389), and knowledge and practice (r=0.393), with all three correlations being statistically significant (Table 4).
DiscussionIt is basically a web-based survey involving 260 F-HCWs working at different hospitals or clinical settings. F-HCWs reported adequate knowledge with a positive attitude and most of them adopted the appropriate practices. Individuals associated with adequate knowledge were doctors, nurses and a few paramedical staff. This study involving over 260 respondents was conducted to assess healthcare workers’ (HCWs) KAP related to COVID-19 during the pandemic and found that levels of knowledge (mean: 9.77 out of 12 points), attitudes (mean: 7.38 out of 10 points), and practices (mean: 4.05 out of 5 points) of COVID-19 were relatively high. However, gaps in knowledge, misconceptions and discriminatory attitudes regarding COVID-19 patients were common, for example, 25 (10%) respondents disagreed that asymptomatic COVID-19 patients spread SARS-CoV-2 and only 50 (19%) respondents disagreed that sharing food items with COVID-19 patients spread SARS-CoV-2 transmission. Misconceptions were mostly prevalent inward attendants, workers and security personnel. Moreover, faculty level respondents had higher levels of knowledge and attitude related to COVID-19 (both p-value for trend <0.05) but practice score was higher of resident doctors (mean score: 4.55).
In contrast to previous studies of KAP related to other infectious diseases (Ebola, H7N9, etc.),13–15 our study showed that COVID-19 awareness was high among health care workers. Moreover, widespread coverage in print and electronic media and other social platforms serves as a constant source of information. The most important reason is related to the measures taken by India, including postponing the start of schools and factories and adopting transport restrictions in various areas, and timely imposition of public curfew and total lockdown. Blocking trains, planes, and other traffic and propagating knowledge of COVID-19 through various media and official guidelines served in containment. In addition, strong publicity across the country and communities at all levels and the experiences of battling SARS, the vast majority of Indian people especially HCWs willingness to pay attention to the epidemic through various channels, obtain correct knowledge, hold positive attitudes, and take necessary precautions. Alzoubi et al. mentioned that the commonest source of knowledge of their participants was social media.16 Although most people try to obtain correct information about COVID-19 through various media, most workers lack professional knowledge and still believe some rumours.
It is essential to wear PPE throughout taking care of the patients, especially when performing aerosol-generating procedures such as; intubation, cardio-pulmonary resuscitation, and nebulization. At the initial stage of the disease outbreak, F-HCWs were infected as most of them were not properly using facemask, gown, and gloves. A negligible amount of N95 respirators were available for the F-HCWs. Upon the arrival of the adequate PPE kits, training of donning and doffing, strict implementations of guidelines the infection to the F-HCWs went down to almost zero. Infection transmission to the F-HCWs at the initial stage was attributable to carelessness, inadequate knowledge, insufficient PPEs, and even improper practices. So, the WHO has also given a particular focus on the correct use of PPEs, including masks, goggles, gloves, and gowns. Additionally, those F-HCWs who used PPEs had comparatively fewer infection rates.
As the health sector comes in the first place as regards the risk that entails its employees, reducing this risk is the first step in providing quality healthcare. The HCWs risk perception could strongly affect not only their mental health but also their exposition to this risk.17,18 It is worth mentioning that, despite their high knowledge score, the vast majority of our respondents were afraid and felt more susceptible to acquire COVID-19 infection even after wearing PPE (16%). This comes in line with Zhou et al. and Maleki et al.19,20 who found that 85% and 92% of HCWs, respectively, were afraid of getting infected with the disease and transmitting it to the family. Determining the risk perceived by the HCWs is considered the basic tool to change the attitude and make the workplace more healthy and safe.17,18
In this study, lack of the PPE was the most commonly mentioned cause for feeling more susceptible followed by dealing with the public who are not committed to preventive measures together with ill ventilation and overcrowding in the workplace. Likewise few other authors reported limited supplies of infection control materials and overcrowding in the emergency rooms were perceived as barriers in infection control practice that could set them at high risk of getting infected.20–22 Even though the healthcare population had a positive general attitude towards the disease preventive measures, more than half (98.8%) of respondents believed that the face mask can protect against infection, and 95% were ready to wear it even if they were previously infected.
It is a fact that F-HCWs are highly susceptible to the infection, while their constant exposure also makes them vectors for disease transmission. Even though the FHCWs have significant roles for infection prevention and disease transmission, it is necessary to follow strict rules of the PPE donning and doffing, hand-hygiene, and isolation of the patients as per the Centre for Disease Control (CDC) and WHO guidelines. The government and stakeholders have the responsibility of providing public awareness, regular updates of the infection prevention protocol, and provide adequate IPC training during this pandemic, and adequate logistic supply. The transmission of the disease among HCWs is compounded by overcrowding, absence of isolation facilities, contaminated environment and is likely enhanced by insufficient knowledge and awareness of infection control practices among HCWs.23
Our study reveals there is a gap in the knowledge towards COVID-19 and infection control practices even after several months of working in the COVID-19 pandemic. Hospital managers can fill this gap from time to time by updating the knowledge and by training of HCWs for infection control practices. In addition, they must focus on motivational factors, including the availability of the resources and provision of incentives and security to family to the F-HCWs. Clinicians can monitor their staff and their attitude towards patients so that nosocomial infections can be prevented. All these measures will be helpful in strengthening the healthcare system and its delivery.
In this study the number of participants is limited. As the participation in the study was voluntary, much of HCW's knowledge could not be recorded. This study included participants of our institution and associated hospital, but it could provide a better analysis of the KAP of HCWs if more government and private hospitals and medical institutions across the country were included. Participants of our study belonged to government organization only which works as a non-profiting service provider but the HCWs working in the private sector may have different view and attitude. Furthermore, like other survey-based studies, results in our study may not be unaffected by response bias.
ConclusionIt can be concluded that F-HCWs reported adequate overall knowledge with a positive attitude and adopted the appropriate practice. The F-HCWs with a higher level of education and more years of experience in health care facilities had better KAP towards COVID-19. Many HCWs specially technicians and students were found lacking appropriate knowledge towards COVID-19.
FundingNone declared.
Conflict of interestNone declared.

