



A 24-year-old man with occasional consumption of alcohol and tobacco, without other significant medical history presented to the Emergency department reporting dyspnea on exertion for 2weeks. He had history of headache, dizziness and fatigability with lack of concentration on daily activities for 4 years. Unemployed due to illness.
On examination blood pressure 128/71mmHg, heart rate 87bpm, oxygen saturation of 81% without supplemental oxygen, marked central cyanosis and clubbing present, edema absent, JVP not raised, chest wall deformity with a scoliosis, a normal cardiopulmonary auscultation.
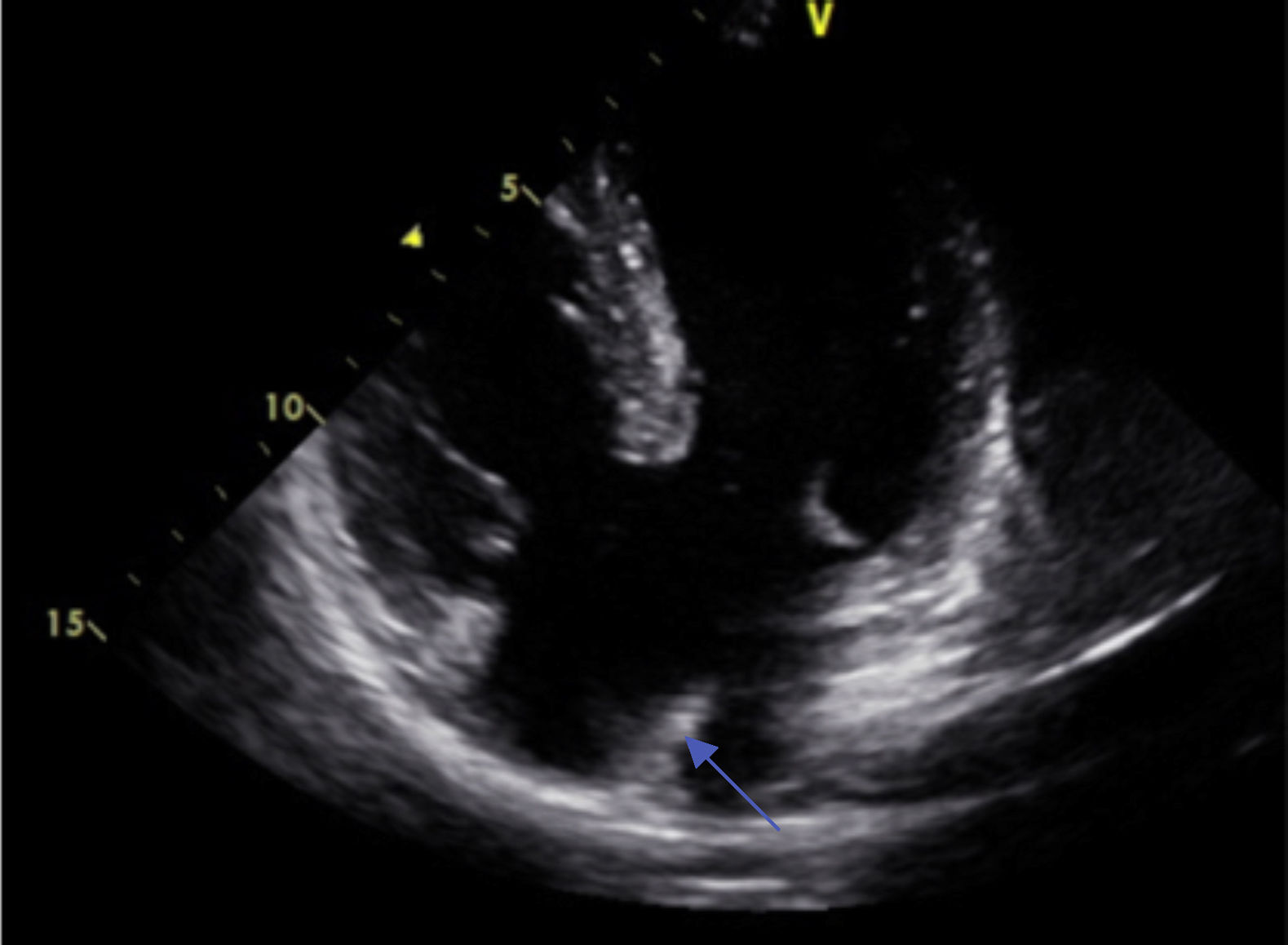
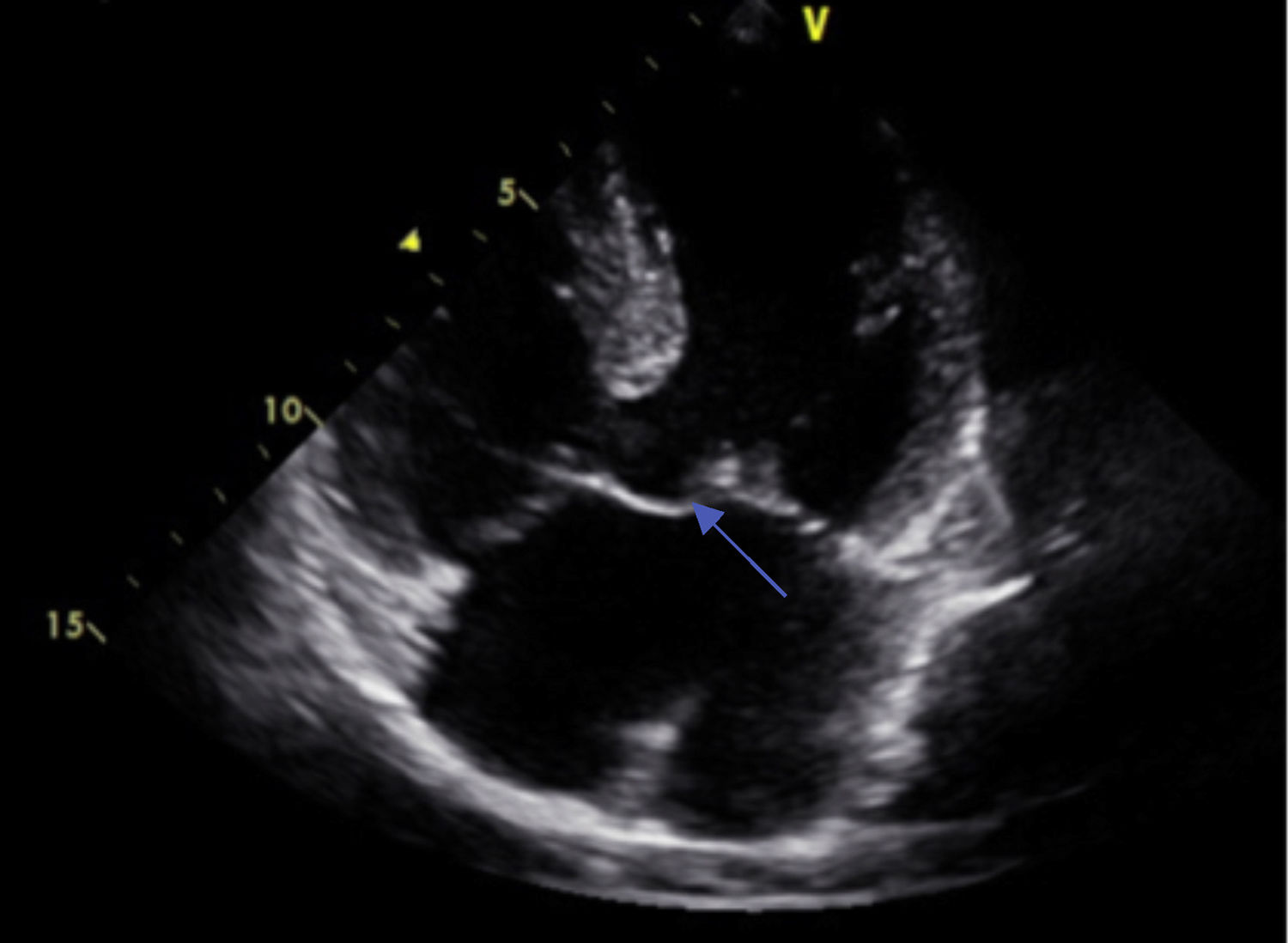
A room air arterial blood gases revealed significant hypoxemic respiratory failure (pO2 45%). On investigation, hemoglobin was 18.9g/dL and haematocrit 53.8%. ECG showed features of ventricular hypertrophy. Chest radiograph showed cardiomegaly. Echocardiography showed congenital cardiac disease with: a complete atrioventricular septal defect (with free communication between 4chambers) (Fig. 1) with a single atrioventricular valve (Fig. 2), reduced vertex inter-ventricular communication, wide communication inter-atrial (30mm); severe pulmonary hypertension (PSAP 80mmHg), preserved ejection fraction, cavities within the limits of normality1-4.
.")
.")
Cerebral computed tomography (CT) was normal and chest CT revealed a marked increase in the caliber of the pulmonary artery (43mm) and presence of a bilateral mosaic pattern, excluding pulmonary thromboembolism. The patient was diagnosed with Eisenmenger Syndrome secondary to untreated congenital cardiac defect.
