


Social representations are the meanings and beliefs built into the processes of social communication about a significant object in the collective life of a group, and these influence the behavior of the group members. Men who have sex with men (MSM) are a risk group for HIV/AIDS. Therefore, knowing their social representation of HIV/AIDS will help to plan strategies for prevention and adherence to treatment.
ObjectiveTo know the social representation of HIV-AIDS among young men who have sex with men (MSM).
MethodAn exploratory qualitative study with a trans-sectional non-experimental design was performed. A non-probability sampling was used. The convenience sample consisted of 25 MSM, who ranged in age from 18 to 29 years and resided in the metropolitan area in a city in northeastern México at the time of application of a free association test and a questionnaire with eight open-ended questions. Data were collected through social networks and a non-governmental organization and were analyzed using a thematic content analysis.
ResultsThe category most associated with HIV-AIDS was “disease,” followed by the categories “acquisition forms” and “death.” These three categories represented 59% of the associations.
ConclusionsYoung MSM who participated in the study had a social representation of HIV/AIDS as a deadly disease, caused by a virus (HIV) that is spread during sex. This representation was strongly burdened with images, beliefs or fears of getting infected or being socially condemned.
The HIV/AIDS pandemic has been plagued with stigma and discrimination from its beginnings in the 1980s. In the public eye, it was quickly linked to gay men and drug users, thus putting a great deal of pressure on these groups.1,2
Even though there was a decrease in the infection rate amongst MSM in the 1990s, recently there has been an increase in new cases within this group in most western countries, since they often practice unsafe sex (without a condom), despite the campaigns which promote the use of the condom.3 According to data from the Pan-American Health Organization, the chances of being infected by HIV in MSM is 33% higher in comparison to general population.4 In Mexico, the epidemic is concentrated in certain groups of the population, such as men who have sex with men, male sex workers and people who use intravenous drugs.5 By age, the most affected are young adults.6 Using a predictive model developed by the Joint United Nations Program on HIV and AIDS (UNAIDS), estimations suggest that the prevalence of HIV infection in the Mexican adult population from 15 to 49 years of age in 2013 was 0.23% (CI 95%: 0.18%, 0.32%).5
The social representation theory was first proposed by Serge Moscovici in the 1960s, picking up on work by Durkheim which highlighted the difference between individual and collective representations. In these studies, the main idea was that collective representations derive from a collective conscience, transcending the individual. The same happens with myths, religion, beliefs and other collective products.6,7 Moscovici does not mention the collective mind, but a vertical social communication process (government, media, school, church) and a horizontal one (amongst citizens).7
The understanding of social representations may be important to achieve the modification of social practice and promote preventative behaviors which individuals can adopt, due to both are affected by the way in which HIV/AIDS is perceived.8,9 From the representational perspective, the pathology is considered a discursive confluence which establishes the frontiers between what's “normal” and what's “pathological”, between what's allowed and what is sanctioned. From this perspective, the disease appears loaded with meanings that link the perception, action, and intervention with respect to the disease.10
Social representations of HIV/AIDS refer to the knowledge and beliefs of a social origin, which are shared and utilized by the members of society, and serve as patterns of the social expressions that this disease raises as a phenomenon.11 The structural perspective of social representation establishes that these are made of a central nucleus that groups and organizes the elements on which there is more consensus, and a peripheral system which is in charge of adapting the representation to a particular context that is presented to the individuals.12,13
Through the health-disease dyad, we can access the image society has of it, since we are able to observe how many of the involved processes are conceived, and how social representations are constituted.14 It is worth noting that in an open society, there is often a plurality of representations of the same object, even when one of them is predominant, and individuals may show discrepancies with the dominant representation due to the affiliations and sense of identity they may have with the members and subgroups of said society.15 Moreover, the representation may be seen as a structured product (cross-section) or as a dynamic process (longitudinal section). From this distinction, the observance of social representation applied to the social construction of risk encourages us to take into consideration the double nature of cognition, as a product and a process.16
The approach of this investigation is based on considering HIV/AIDS, not only as a medical disease, but also as a social phenomenon characterized by different meanings, beliefs, and feelings and influenced by the cultural surroundings.11 The objective of this study was to discover the social representation of HIV/AIDS in one of the main groups at risk of acquiring this condition, such as the group of MSM young adults.
Methods and materialsAn exploratory qualitative study with a trans-sectional non-experimental design was performed. The inclusion criteria were: being a man who has sex with men, being between the ages of 18 and 30, and to live in Monterrey or its metropolitan area. Exclusion criteria included: being illiterate, having a mental disability or cognitive deterioration which impeded answering the written questionnaire and free association test. Elimination criteria was an incomplete questionnaire or the non-completion of the free association test. Non-probabilistic sampling was utilized. The convenience sample consisted of 25 participants and was put together through social networks (Facebook and Grindr) and through a non-governmental organization Metropolitan Community A.C. (COMAC by its Spanish acronym), between January and July 2015. The participants answered a questionnaire in either written or electronic form. The questionnaires were sent via email (for those participants on Facebook and Grindr) or handed out (for those participants from the COMAC).
Informed consent was requested (without a signature), guaranteeing complete confidentiality of the information, anonymity, and the availability to resolve any question. For this purpose, an institutional affiliation, as well as the email address of those responsible for this study was provided. We did not request personal data, nor information on their HIV serological status. The research was approved in its ethical aspects by the Master's and Thesis Ethics Committee at the Psychology School at the UANL, and we adhered to the recommendations given by the American Association of Psychology.17
A questionnaire was applied, starting with the informed consent request, and three questions about socio-demographics (gender, age, and level of schooling); it continued with a free association test (with space for ten possible words) with three instructions: which words come to your mind when you hear the word AIDS? Put them in order of importance for you, and indicate the opposite word and define each word, and finished with eight open-ended questions: How did you find out about the existence of AIDS? Are HIV and AIDS the same thing? (If the answer to this question is no, how did you find out?) Moreover, what is the difference between HIV and AIDS? What does ‘being HIV positive’ mean for you? How do people get HIV? What is your biggest fear in case you were HIV positive? Does the existence of HIV/AIDS affect your sex life? What are you doing to avoid getting HIV? How do you imagine people with HIV live?
The questionnaire was designed specifically for this study by the authors of the article with the objective of exploring the representation of HIV/AIDS. Hence, the use of the free-association test (exploration of semantic fields or group of meaning linked to the stimuli word AIDS) and the format of some open-ended questions about the knowledge and beliefs about HIV/AIDS. The formulation of questions implicitly assumed that HIV/AIDS is an acquired and non-congenital disease, but without implying its infectious nature via sexual transmission or via bloodstream, chronic, deadly and treatable (with chronic treatment which controls the virus, yet does not eliminate it) transmitted by the homogenized medical speech by the UNAIDS international institution.18 Content validity and reliability of the questionnaire was not established, given the fact that it was an exploratory qualitative study.19 Its temporal reliability was not proved either, nor was its internal consistency. No other validation tests were conducted (concurrent, predictive, or retrodictive). Therefore, the replicability degree of our results is unknown.
The data were analyzed using a thematic content analysis, frequency and percentage tables, central nucleus and the three peripheries using the ideal structural method by Abric.15,16,20 We used Microsoft Excel 2007 to process these calculations.
ResultsAmongst the 25 MSM who conformed to our sample, the age range was between 18 and 29 years of age, with a mean age of 22.12 and a standard deviation of 2.89. The range of years of schooling varied between 10 and 16 years, with a mean age of schooling of 12.75 and a standard deviation of 2.13.
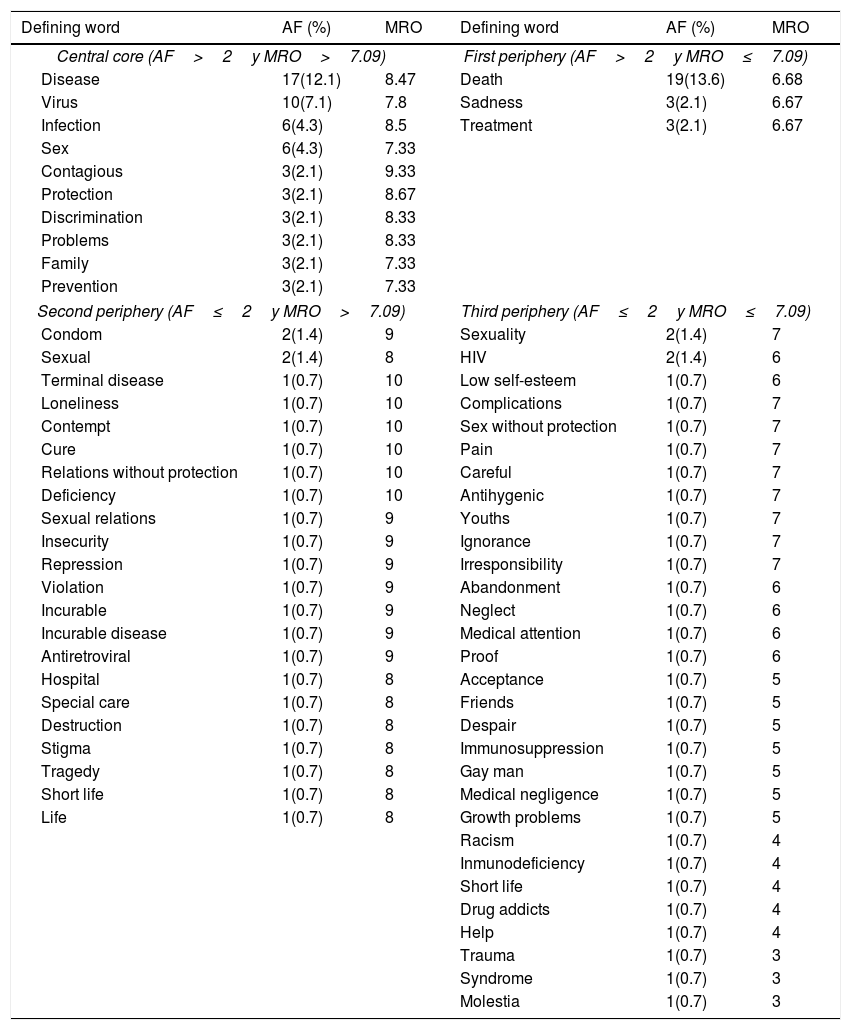
For every defining word (associated words to the stimuli word AIDS), its association frequency (AF) and mean representativeness order (MRO) were calculated. Regarding the order of representativeness, each defining word was given an ordinal value of 10 (the maximum number of associated words to the stimulus word) when said defining word was ordered in first place of representativeness by the participant, 9 when placed in second place, 8 in third, 7 in fourth, 6 in fifth, 5 in sixth, 4 in seventh, 3 in eight, 2 in ninth and 1 when placed in tenth place. When adding these values and dividing them by the number of summed values, we obtained the MRO of each defining word. Thus, the MRO ranged from 10 (the highest representativeness) to 1 (the lowest representativeness). The central nucleus and the three peripheries of the presentation of AIDS were determined from the arithmetic means of AF and MRO. The arithmetic mean AF of the 66 defining words in all 140 associations was 2.012, and MRO was 7.090. The central nucleus of representativeness was determined by the defining words with a high AF (>2) and a high MRO (>7.08). The first periphery was formed by the defining words of high AF (>2) and a low MRO (≤2). The second periphery was formed by the defining words of low AF (≤7.09) and high MRO (>7.09). Lastly, the third periphery was formed by the defining words of low AF and low MRO. (Table 1)
Representation of AIDS through 66 defining words.
| Defining word | AF (%) | MRO | Defining word | AF (%) | MRO |
|---|---|---|---|---|---|
| Central core (AF>2y MRO>7.09) | First periphery (AF>2y MRO≤7.09) | ||||
| Disease | 17(12.1) | 8.47 | Death | 19(13.6) | 6.68 |
| Virus | 10(7.1) | 7.8 | Sadness | 3(2.1) | 6.67 |
| Infection | 6(4.3) | 8.5 | Treatment | 3(2.1) | 6.67 |
| Sex | 6(4.3) | 7.33 | |||
| Contagious | 3(2.1) | 9.33 | |||
| Protection | 3(2.1) | 8.67 | |||
| Discrimination | 3(2.1) | 8.33 | |||
| Problems | 3(2.1) | 8.33 | |||
| Family | 3(2.1) | 7.33 | |||
| Prevention | 3(2.1) | 7.33 | |||
| Second periphery (AF≤2y MRO>7.09) | Third periphery (AF≤2y MRO≤7.09) | ||||
| Condom | 2(1.4) | 9 | Sexuality | 2(1.4) | 7 |
| Sexual | 2(1.4) | 8 | HIV | 2(1.4) | 6 |
| Terminal disease | 1(0.7) | 10 | Low self-esteem | 1(0.7) | 6 |
| Loneliness | 1(0.7) | 10 | Complications | 1(0.7) | 7 |
| Contempt | 1(0.7) | 10 | Sex without protection | 1(0.7) | 7 |
| Cure | 1(0.7) | 10 | Pain | 1(0.7) | 7 |
| Relations without protection | 1(0.7) | 10 | Careful | 1(0.7) | 7 |
| Deficiency | 1(0.7) | 10 | Antihygenic | 1(0.7) | 7 |
| Sexual relations | 1(0.7) | 9 | Youths | 1(0.7) | 7 |
| Insecurity | 1(0.7) | 9 | Ignorance | 1(0.7) | 7 |
| Repression | 1(0.7) | 9 | Irresponsibility | 1(0.7) | 7 |
| Violation | 1(0.7) | 9 | Abandonment | 1(0.7) | 6 |
| Incurable | 1(0.7) | 9 | Neglect | 1(0.7) | 6 |
| Incurable disease | 1(0.7) | 9 | Medical attention | 1(0.7) | 6 |
| Antiretroviral | 1(0.7) | 9 | Proof | 1(0.7) | 6 |
| Hospital | 1(0.7) | 8 | Acceptance | 1(0.7) | 5 |
| Special care | 1(0.7) | 8 | Friends | 1(0.7) | 5 |
| Destruction | 1(0.7) | 8 | Despair | 1(0.7) | 5 |
| Stigma | 1(0.7) | 8 | Immunosuppression | 1(0.7) | 5 |
| Tragedy | 1(0.7) | 8 | Gay man | 1(0.7) | 5 |
| Short life | 1(0.7) | 8 | Medical negligence | 1(0.7) | 5 |
| Life | 1(0.7) | 8 | Growth problems | 1(0.7) | 5 |
| Racism | 1(0.7) | 4 | |||
| Inmunodeficiency | 1(0.7) | 4 | |||
| Short life | 1(0.7) | 4 | |||
| Drug addicts | 1(0.7) | 4 | |||
| Help | 1(0.7) | 4 | |||
| Trauma | 1(0.7) | 3 | |||
| Syndrome | 1(0.7) | 3 | |||
| Molestia | 1(0.7) | 3 | |||
Source: Elaborated by the authors.
Notes: AF=association frequency; MRO=mean representativeness order; %=percentage in relation to the total of 140 associations.
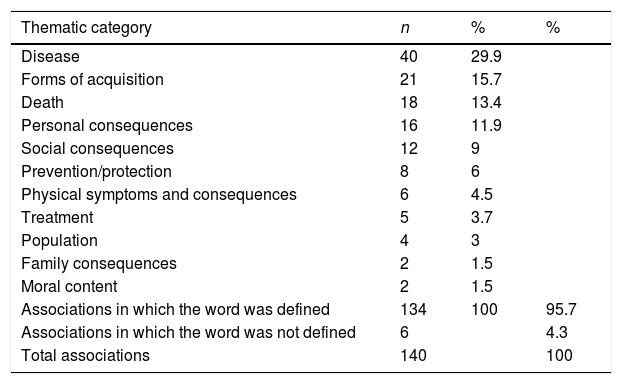
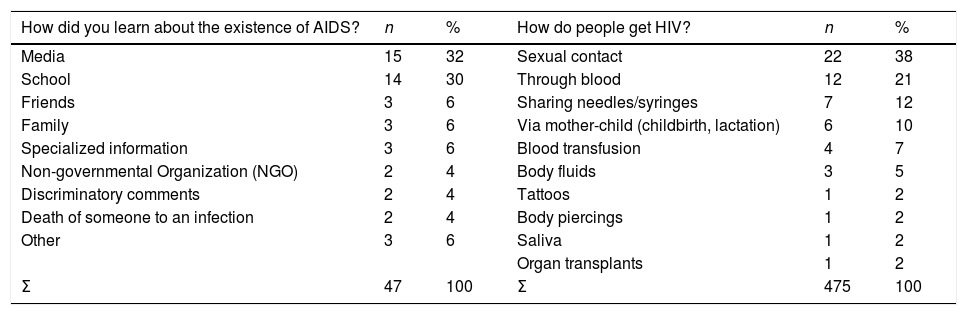
From the definitions given to the 66 defining words in 134 associations (in 6 associations the participant did not define the word), 11 thematic categories were elaborated on: disease (this category included words like “disease”, “virus”, “infection”, “hospital”), form of acquisition (“sexual transmission”, “contagion”, “infection”, “sex”, “unprotected sex”, “sexually transmitted infection”, “sex without protection”, “sexuality”, “sexual relations”, “medical negligence”), death (“death”), personal consequences (“distress”, “loss of hope”, “frustration”, “isolation”, “tragedy”, “loneliness”, “personal problems”, “low self-esteem”, “trauma”, “repression”, “special care”, “to need medical attention”), social consequences (“discrimination”, “friends”, “stigma”, “support”, “racism”, “destruction”, “disregard”, “ignorance”, “neglect”, “irresponsibility”), family consequences (“family problems”), prevention or protection (“red ribbon”, “care”, “condom”, “prevention”, “test”, “protection”, “condom and prevention”), physical consequences or symptoms (“skin sores”, “deficiencies”, “complications”, “discomfort”), population (“gay men”, “drug addicts”, “young people”), treatment (“antiretroviral drugs”, “cure”) and moral content (forms of acquisition with judgment or moral condemnation). In Table 2, we can see that disease represents 29.9% of the content present in all 134 associations. This content was followed by forms of acquisition, death, personal and social consequences. These four thematic categories represented 70.9% of the content. Moreover, nine new categories were created for the answers to the question about the original source by which the participant found out about the existence of AIDS. The category media represented 32% of the 47 sources mentioned, while school represented 30%. (Table 3).
Frequency of the categories created for the definitions given to the 66 defining words from the word stimulus AIDS.
| Thematic category | n | % | % |
|---|---|---|---|
| Disease | 40 | 29.9 | |
| Forms of acquisition | 21 | 15.7 | |
| Death | 18 | 13.4 | |
| Personal consequences | 16 | 11.9 | |
| Social consequences | 12 | 9 | |
| Prevention/protection | 8 | 6 | |
| Physical symptoms and consequences | 6 | 4.5 | |
| Treatment | 5 | 3.7 | |
| Population | 4 | 3 | |
| Family consequences | 2 | 1.5 | |
| Moral content | 2 | 1.5 | |
| Associations in which the word was defined | 134 | 100 | 95.7 |
| Associations in which the word was not defined | 6 | 4.3 | |
| Total associations | 140 | 100 |
Source: Elaborated by the authors.
Notes: n=absolute frequency; %=percentage.
Frequency of the categories created for the answers to the questions: how did you learn about the existence of AIDS? How do people get HIV?
| How did you learn about the existence of AIDS? | n | % | How do people get HIV? | n | % |
|---|---|---|---|---|---|
| Media | 15 | 32 | Sexual contact | 22 | 38 |
| School | 14 | 30 | Through blood | 12 | 21 |
| Friends | 3 | 6 | Sharing needles/syringes | 7 | 12 |
| Family | 3 | 6 | Via mother-child (childbirth, lactation) | 6 | 10 |
| Specialized information | 3 | 6 | Blood transfusion | 4 | 7 |
| Non-governmental Organization (NGO) | 2 | 4 | Body fluids | 3 | 5 |
| Discriminatory comments | 2 | 4 | Tattoos | 1 | 2 |
| Death of someone to an infection | 2 | 4 | Body piercings | 1 | 2 |
| Other | 3 | 6 | Saliva | 1 | 2 |
| Organ transplants | 1 | 2 | |||
| Σ | 47 | 100 | Σ | 475 | 100 |
Source: Elaborated by the authors.
Notes: n=absolute frequency; %=percentage; Σ=sum per column.
Regarding the question about whether or not HIV was the same as AIDS, 56% answered no, while 40% answered yes and 2% reserved their answer. Those participants who answered no were asked how they had found out, then, the following five thematic categories were created for their answers. At school represented 36% of the sources of this information, through a governmental organization represented 21%, searching on the internet represented 14%, reading represented 14%, informed talks represented 7%, and 7% did not answer the question.
The participants were also asked if they knew what the difference between HIV and AIDS was. In general, the participants indicated that HIV is a virus that, when infecting the body, may cause AIDS to develop, which they consider the disease. To cite some representative answers, one participant answered “HIV is the presence of the human immunodeficiency virus in an organism. AIDS is the acquired immunodeficiency syndrome. Moreover, as such, it involves a series of ailments, signs, and symptoms, considered the final stage of the infection”. Another commented: “HIV is a virus people can live with, without having it develop, while AIDS is a disease which you do need to treat to avoid worsening consequences.” Another answer was “HIV is the existence of the human immunodeficiency virus in the organism, and AIDS describes the symptoms that appear when HIV levels begin altering the organism at a functional level.”
Then they were asked, “What would be HIV positive mean to you?” The content of the answers was about issues regarding health and lifestyle changes, death, and rejection from family and friends. For example, a participant said “It would mean having the HIV virus, undergoing treatment and a different lifestyle. It would mean becoming someone who, in the future, will develop the AIDS”. Another person answered, “To start, a great anguish as a result of what people may say or think, how I would tell my parents and friends, and whether or not this would affect my career. On the bright side, having detected it, there is a therapy which will give me a decent quality of life and extend my life expectancy.” Another response was: “a complete change of life. If you control it, you can live with it, but you will always have to be careful to prevent it from developing”.
For the answers to the question “How do people become infected with HIV?”, ten thematic categories were created. The categories of sexual contact, the bloodstream, and needle/syringe sharing represented 71% of the 475 means of infection mentioned (Table 3).
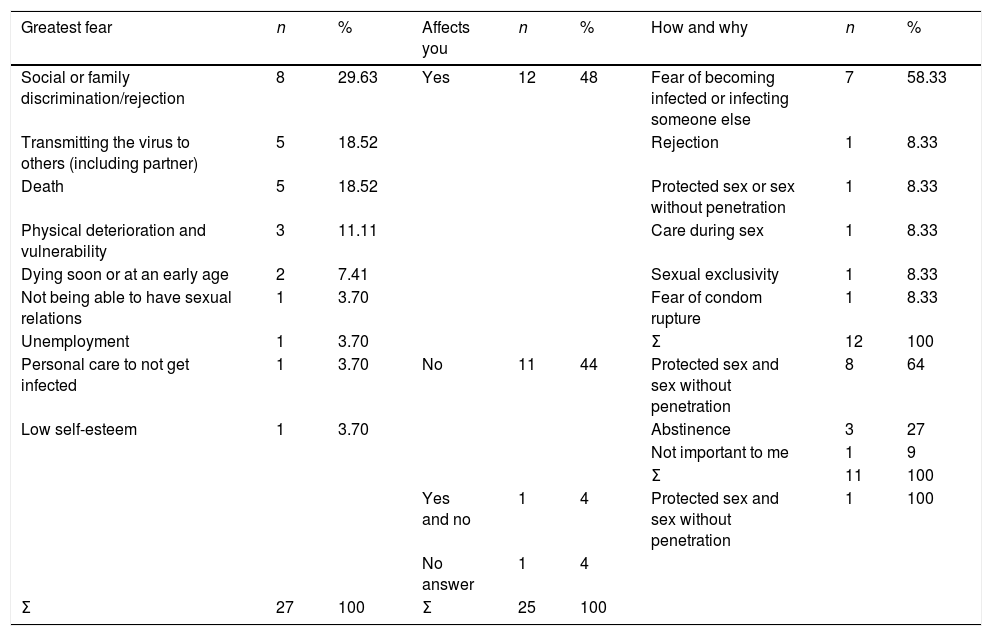
For the question “What is your greatest fear in case you were HIV positive?” six thematic categories were created. The categories of discrimination and social rejection (including family), fear of infecting others (including a partner), fear of dying and physical deterioration and vulnerability represented 78% of the 27 fears mentioned (Table 4).
Frequency of the categories created for the answers to the questions: what is your greatest fear in the case that you were HIV positive? How does the existence of HIV/AIDS affect you?
| Greatest fear | n | % | Affects you | n | % | How and why | n | % |
|---|---|---|---|---|---|---|---|---|
| Social or family discrimination/rejection | 8 | 29.63 | Yes | 12 | 48 | Fear of becoming infected or infecting someone else | 7 | 58.33 |
| Transmitting the virus to others (including partner) | 5 | 18.52 | Rejection | 1 | 8.33 | |||
| Death | 5 | 18.52 | Protected sex or sex without penetration | 1 | 8.33 | |||
| Physical deterioration and vulnerability | 3 | 11.11 | Care during sex | 1 | 8.33 | |||
| Dying soon or at an early age | 2 | 7.41 | Sexual exclusivity | 1 | 8.33 | |||
| Not being able to have sexual relations | 1 | 3.70 | Fear of condom rupture | 1 | 8.33 | |||
| Unemployment | 1 | 3.70 | Σ | 12 | 100 | |||
| Personal care to not get infected | 1 | 3.70 | No | 11 | 44 | Protected sex and sex without penetration | 8 | 64 |
| Low self-esteem | 1 | 3.70 | Abstinence | 3 | 27 | |||
| Not important to me | 1 | 9 | ||||||
| Σ | 11 | 100 | ||||||
| Yes and no | 1 | 4 | Protected sex and sex without penetration | 1 | 100 | |||
| No answer | 1 | 4 | ||||||
| Σ | 27 | 100 | Σ | 25 | 100 |
Source: Elaborated by the authors.
Notes: n=absolute frequency; %=percentage; Σ=sum per column.
When we asked them if the existence of HIV/AIDS affected their sex life, 48% answered yes, while 44 responded no, 4% responded yes and no and 4% avoided the question. The 12 participants who answered yes were asked how they were affected, and 6 categories were created for their answers; 58% stated that they were afraid of infecting someone or being infected. Moreover, thematic categories for the arguments given by the other 13 participants were elaborated on. From those who answered no, 64% stated they practiced safe sex (use of condoms) or without penetration, 27% said they refrained from having sexual relations, and 9% commented that this was not important for them. The person who avoided the question asked to be informed, and the participant who answered yes and no stated that they practiced safe sex without penetration (Table 4).
For those answers to the question “What are you doing to avoid being infected with HIV?” Four thematic categories were created, 68% stated that they used a condom, 12% avoided penetration, 12% refrained from sex, and 8% gave different answers. Amongst these last ones, one of the participants responded “Not to engage in sexual relations with people who may carry this disease…” which stands out from the majority of responses.
The last question of the questionnaire was “How do you think people with HIV live?” Sadness, rejection, and discrimination represented 88% of the contents of this answer. Within the distinctive answers to this question were the following answers: “really sad and despairing,” “afraid of dying and sad,” “well, really bad, they have to be careful all the time, other people look at them with disdain.”
DiscussionFrom the data from the free association test, we are able to observe that the central nucleus of AIDS's social representation amongst young MSM who participated in this study. They consisted of the ten words (disease, virus, infection, sex, contagion, protection, discrimination, problems, family, and prevention), since they are the words with the highest frequency and with high representativeness. From this representational nucleus, we can observe that AIDS is seen as an infectious disease which leads to discrimination, a wide range of problems and feelings of shame within the family. More precisely, when imagining a person living with HIV, the load of negative feelings is evident. Sadness, rejection, and discrimination are all embedded into the meaning of this infectious disease. These images agree with other studies, which have pointed out that disease, death, discrimination, and sex appear in central contents in AIDS's social representations.9,10,16,21 In this study, associations with sex are within the first periphery (less frequent words, but to which a great deal of importance is conceded). However, the family stands out in the central nucleus. The outstanding part about family in this representation and living with HIV have been highlighted by other studies conducted in Mexico, and it is attributable to the centrality family possesses in the Mexican socioemotional world.22,23
Amongst young MSM, being gay and homosexuality is a part of the third periphery of the AIDS representation, that is, meanings with less association to which less importance is given. Furthermore, there is no mention about this when speaking about how to avoid becoming infected by HIV, and how the existence of HIV affects their sex life. When mentioning what their greatest fear was in the case of being HIV positive, discrimination and rejection for being the carrier of a transmittable disease were at the top of the list, not being attributed to public exposure of their sexual preferences. Nevertheless, the sexual stigma content is, in fact, implicit in the shame before the family. Also, studies conducted on women living with HIV report their fear of rejection and discrimination, since they are considered to be unfaithful or promiscuous.23,24 Both fears are related with the social control of sexuality in Mexico, where gay preferences are stigmatized in men, along with promiscuity and unfaithfulness in women.23
It is worth noting that death is a frequently associated meaning, even though it is not given enough importance, being a part of the second periphery in this study, as well as in other studies,10,16 which could be attributed to the cognitive avoidance of terrifying things.8 On the other hand, treatment is regarded as necessary and with side effects, although some commented that it increased the quality of life.
The behaviors mentioned to avoid becoming infected with HIV and how the existence of HIV clearly affects their sex life clearly reflect the impact of the prevention campaigns which are aimed specifically at MSM.4 Thus, from the data in the open-ended questions, one can deduce that this representation proceeds from formal sources, i.e., school and prevention campaigns on different media outlets, as well as from informal sources, i.e., family, friends and implicit social attitudes. Although some researchers mention that it has been observed that specialized information is not the favored source of construction of AIDS's representations of university students,21 in the present study with MSM, formal sources do have a great weight, even in the form of avoiding infection and how it affects their sexuality.
As a limitation of the study, the use of non-probabilistic sampling and a relatively small number of participants should be noted, so the results do not admit an inference regarding probability to the population; they can only be used as comparison data or sources of the hypothesis. Both limitations were a consequence of the reluctance of young MSM from Monterrey to participate in HIV/AIDS survey studies. The HIV status of the participants is unknown, as they were not asked about it to avoid ethical complications in the study and facilitate participation. Hence, the population from which this incidental sample was extracted is that of young MSM regardless of their serological status, which constitutes a population adequate for the exploratory objective of the study (social representation of HIV/AIDS), especially when it is indicated as one of the populations with the highest risk of infection. Inter-rater reliability of the thematic categories created to analyze the data should still be estimated; to ensure that this metric property is high, these categories were designed following the principles of simplicity, completeness, exclusivity and reduced number.19 Finally, there is the limitation that the validity of the content of the questionnaire created expressly for this study has not been established with an expert's judgment. In the conventional procedure of this type of exploratory qualitative studies on inter-individual subjectivity, the validity of the content of the instrument has not been established, due to the lack of a precise definition of the construct and the accent of the study in the spontaneous emergence of meanings and beliefs. On the contrary, this property does have special relevance in quantitative research aimed at estimating population parameters.19 Consequently, since the reliability and validity of the questionnaire applied have not been established, the degree of replicability of the results is unknown, even if they were obtained with a large sample drawn by probabilistic sampling.
It is concluded that, among the 25 young MSM participating in the study, the social representation of HIV/AIDS is that of a deadly disease, caused by a virus (HIV) that is spread during sex (sexual relations), and that is heavily loaded wiih negative images and beliefs or related to the fear of contagion and social rejection. This representation comes from formal sources, such as at school and through lectures given by NGOs, as well as from experience with people living with HIV and information and beliefs that are transmitted in everyday conversations. Half of them are affected in their sexual relations, which motivates most to practice protected sex and generates a positive attitude toward retroviral treatment, which is seen as a means to prolong and give quality of life.
Taking up the present exploratory study as a first qualitative phase, it is suggested to use this information to elaborate on an instrument with a semantic differential for the meanings of AIDS and closed questions on HIV/AIDS. It is recommended to submit the new instrument to an expert's judgment to establish its content's validity and to determine its reliability properties (internal consistency and temporal stability) and construct validity. With this new instrument, and using a larger sample, one could further deepen the representation of HIV/AIDS in the population under study.
FundingThe study was financed by the authors. The first author had won a scholarship for Master studies granted by the National Board Science and Technology during the completion of this study. The data presented hereunder are derived from his Master's dissertation in Master in Science with a major in health.
Conflict of interestsAuthors declare that there are no conflicts of interest.
To the Metropolitan Community A.C. (COMAC by its Spanish acronym), a non-governmental organization created for the prevention and support to people with HIV and STDs, for their support in the recruitment part of the participants of this study.