




We report a case of a 18-year-old male patient with a diagnosis of pseudoaneurysm of the right superficial femoral artery secondary to penetrating injury by gunshot, which was treated in our Hospital with an aneurysm resection and a saphenous vascular graft inverted with a satisfactory evolution.
Introduction
Trauma is the 3rd leading cause of death among the general population. Vascular injuries represent 3% of everyday traumas with a high morbidity. Extremity pseudoaneurysms are developed after penetrating trauma in 60% of arterial injuries. In 40% of those cases, the trauma is caused by a gunshot wound.1
In medical literature, we are able to find a series of small amounts of cases; however, in a study by Yetkin et al., they presented 8 patients with pseudoaneurysms located in the femoral, popliteal and tibioperoneal arteries secondary to gunshot wounds. They concluded that the diagnosis depends on the high rate of suspicion by the healthcare provider, and the longer the diagnosis takes, the more complications they may have, up to loss of the limb.2
Case presentation
We report a case of a patient, male, 18-year-old with a gunshot wound in the right lower extremity that was assessed in a different medical facility and was discharged without an evident vascular injury. Four months after the incident, the patient came to the General Surgery Department at our Hospital for a consultation with pain in the right lower extremity and a limited gait. During physical examination a pulsatile tumor of 9 x 7 x 9 cm in the external face of the right thigh with the presence of a murmur in the femoral region was documented; the rest of the extremity displayed palpable pulse with a good intensity (Fig. 1).
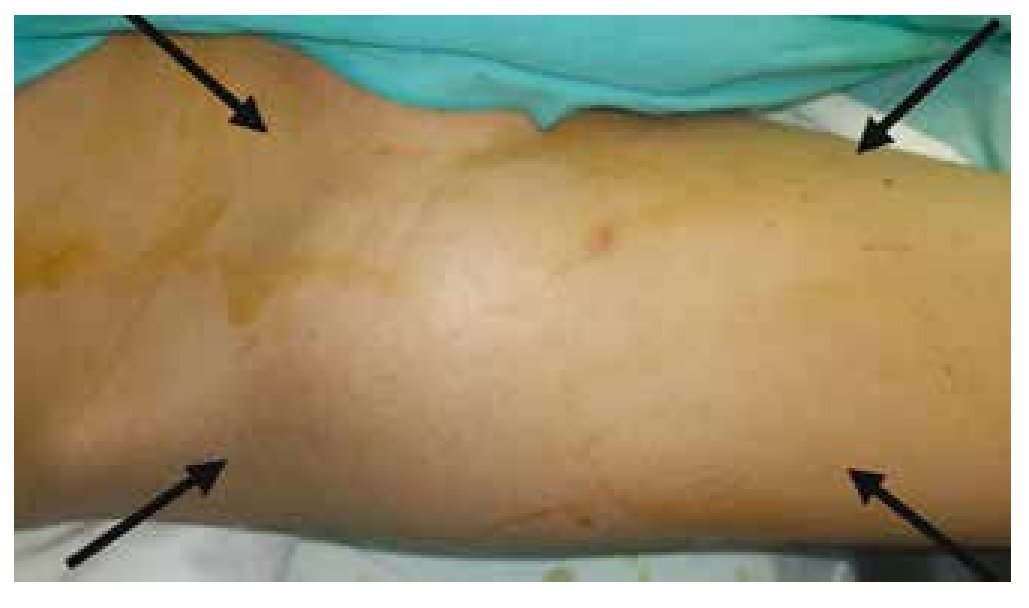
Figure 1 Lump in anterior side outside of right thigh.
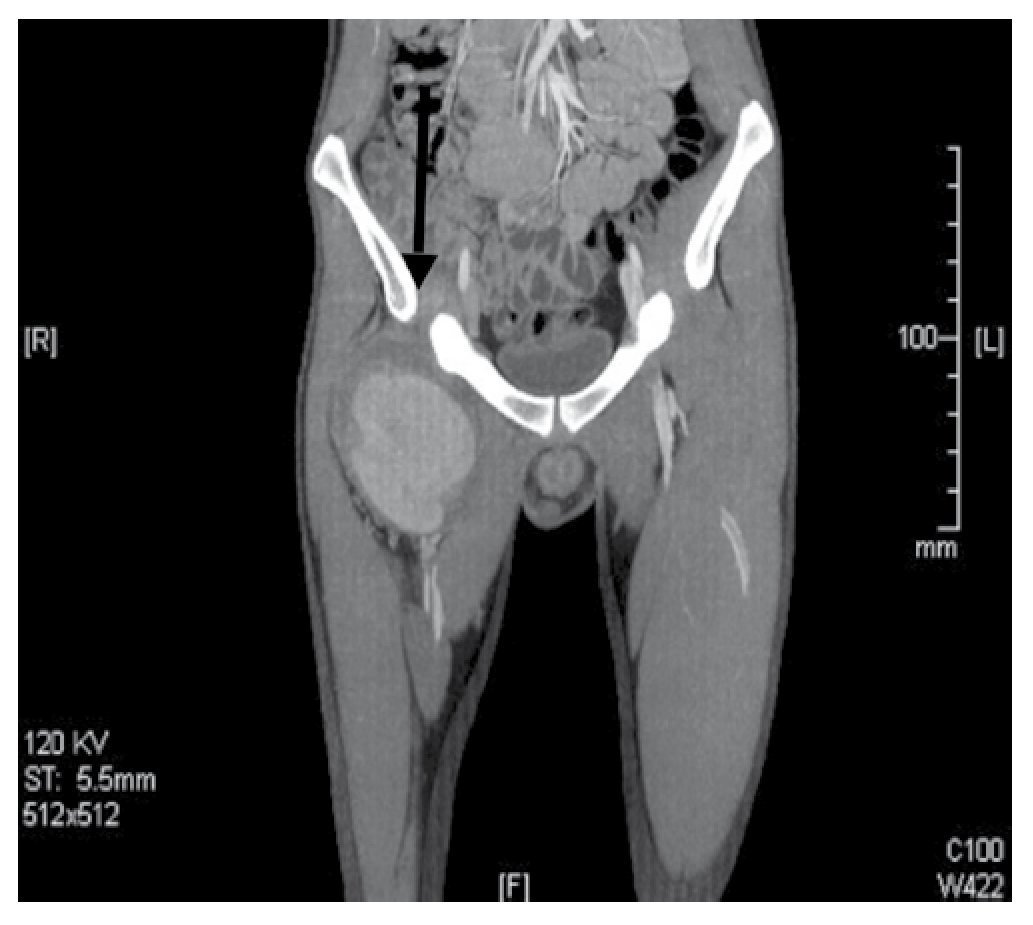
We performed an angiotomography showing an arterial aneurysm 10 x 8 x 7 cm originating from the superficial fe-moral artery with a continuity solution of 0.58 cm, which communicated with the deep femoral artery (Figs. 2 and 3).
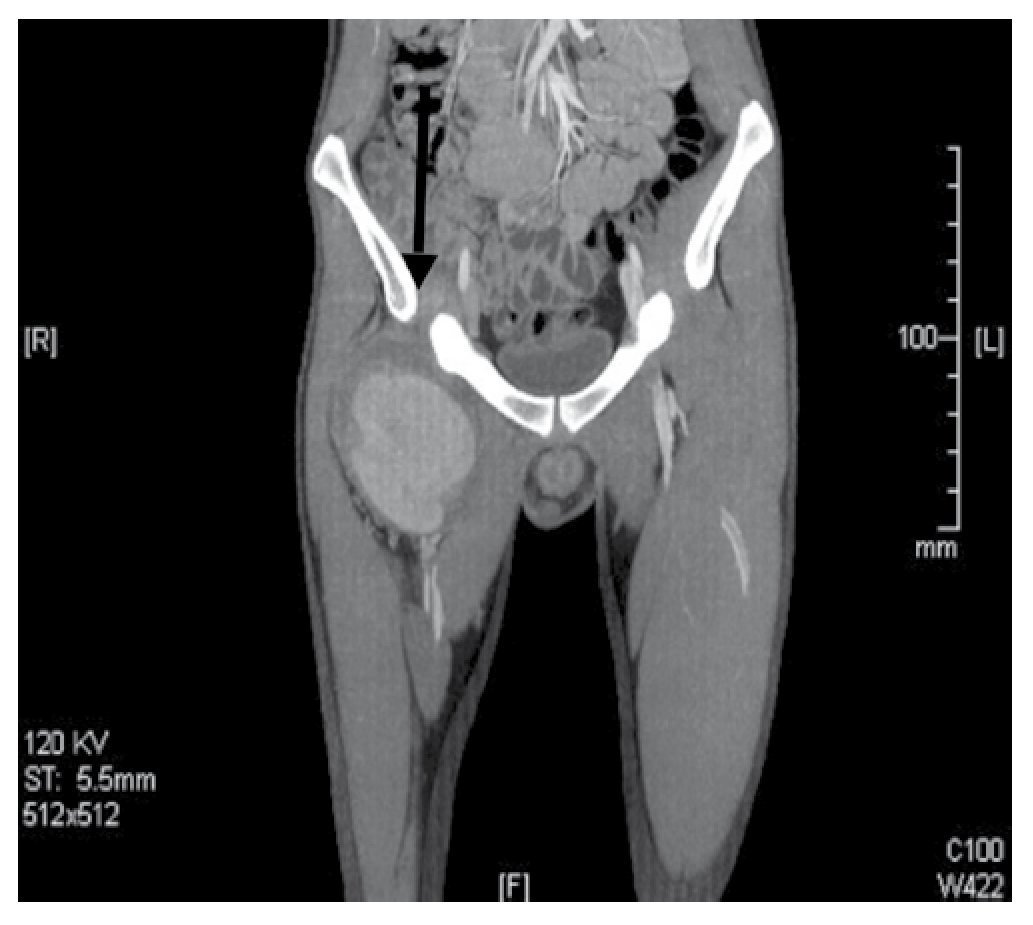
Figure 2 Computed axial tomography in coronal section showing pseudoaneurysm of the superficial femoral artery.
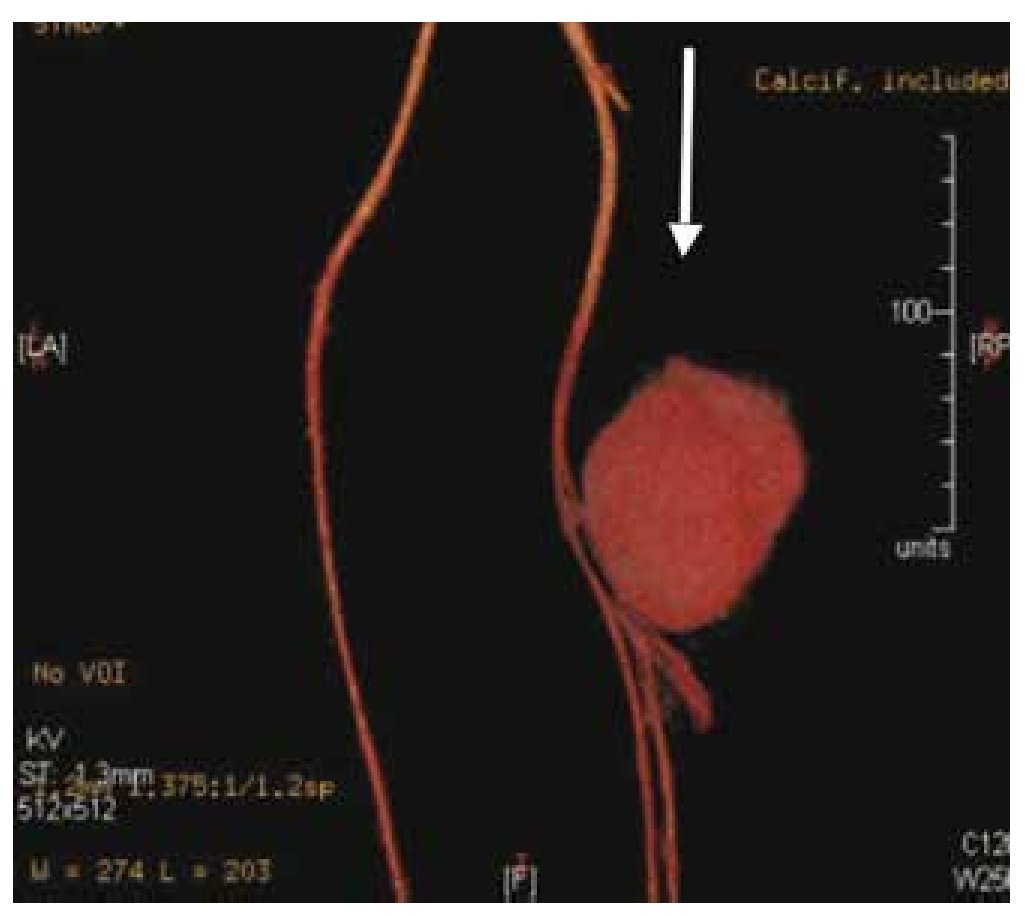
Figure 3 3D recontruction of the pseudoaneurysm of the fe-moral artery.
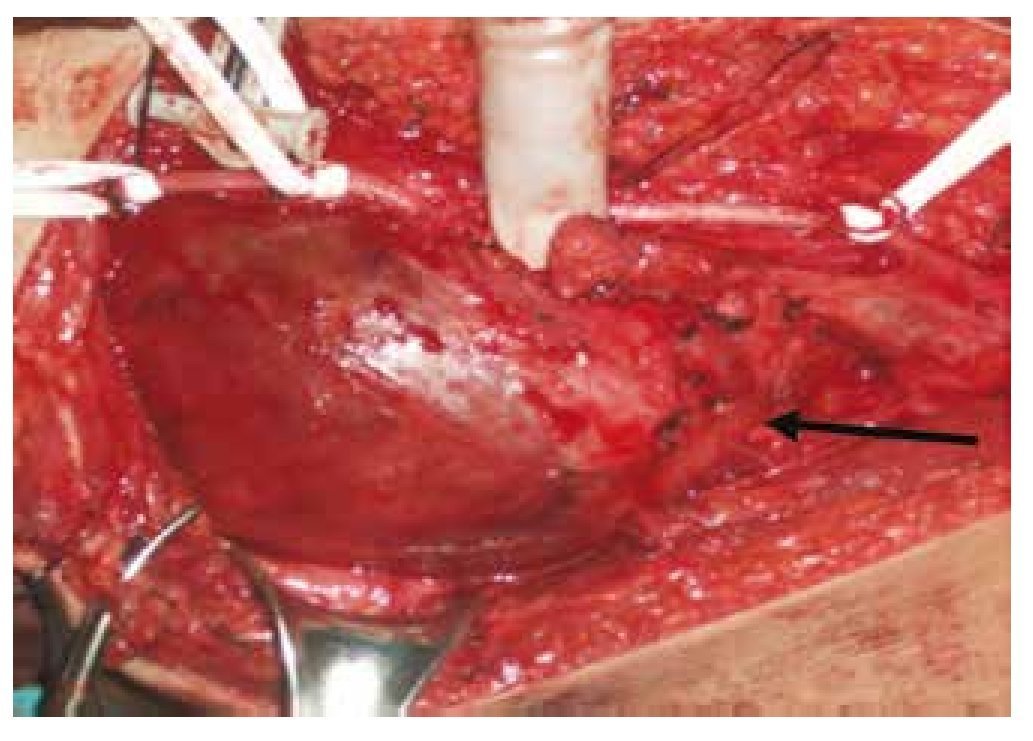
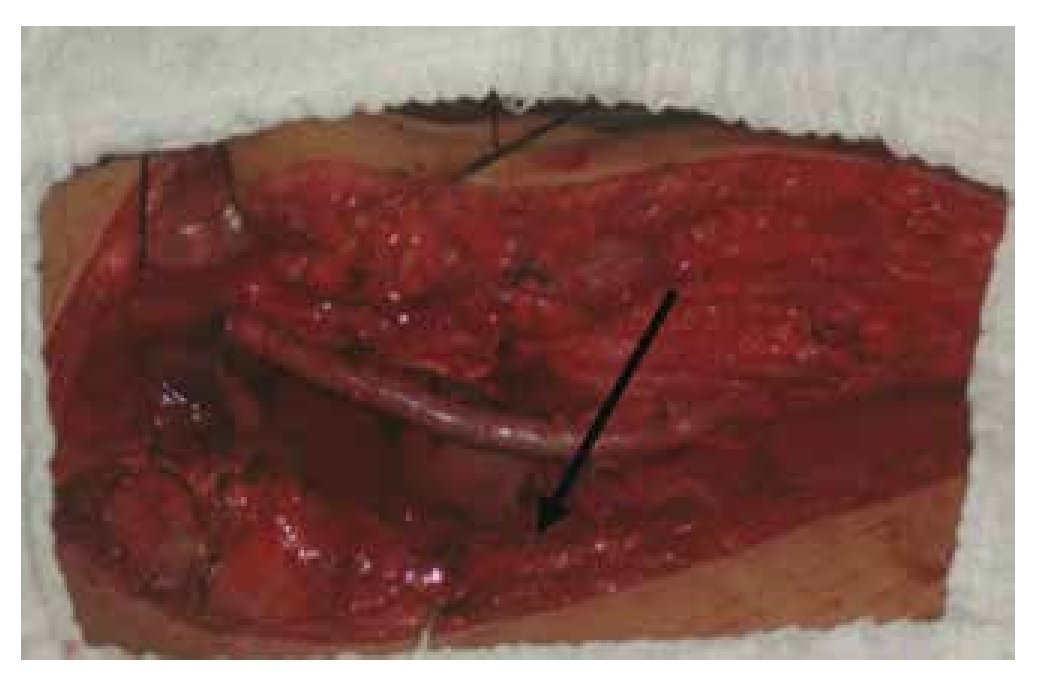
Our surgical strategy consisted of performing proximal and distal vascular control of the superficial femoral artery, complete resection of the superficial femoral artery aneurysm (Fig. 4) and placement of the inverted saphenous graft (Fig. 5). The patient was discharged after a 7-day post-surgical stay, with a good evolution without complications, and after a follow-up period of a year of consultations, the patient was reported as fully asymptomatic.
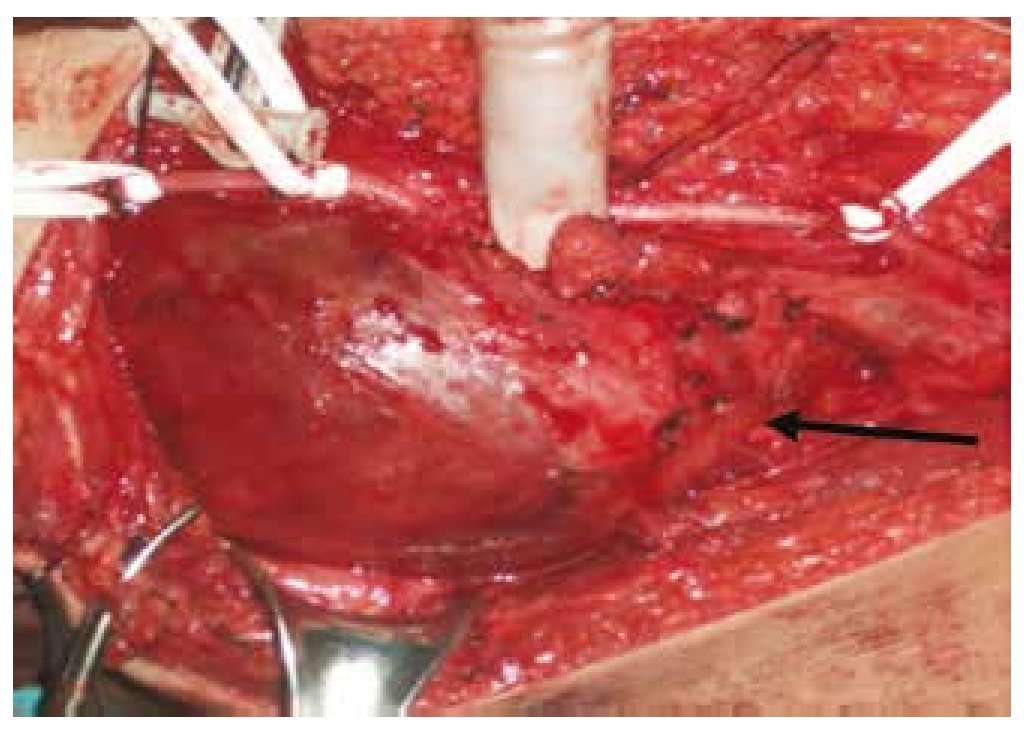
Figure 4 Pseudoaneurysm of the superficial femoral artery.
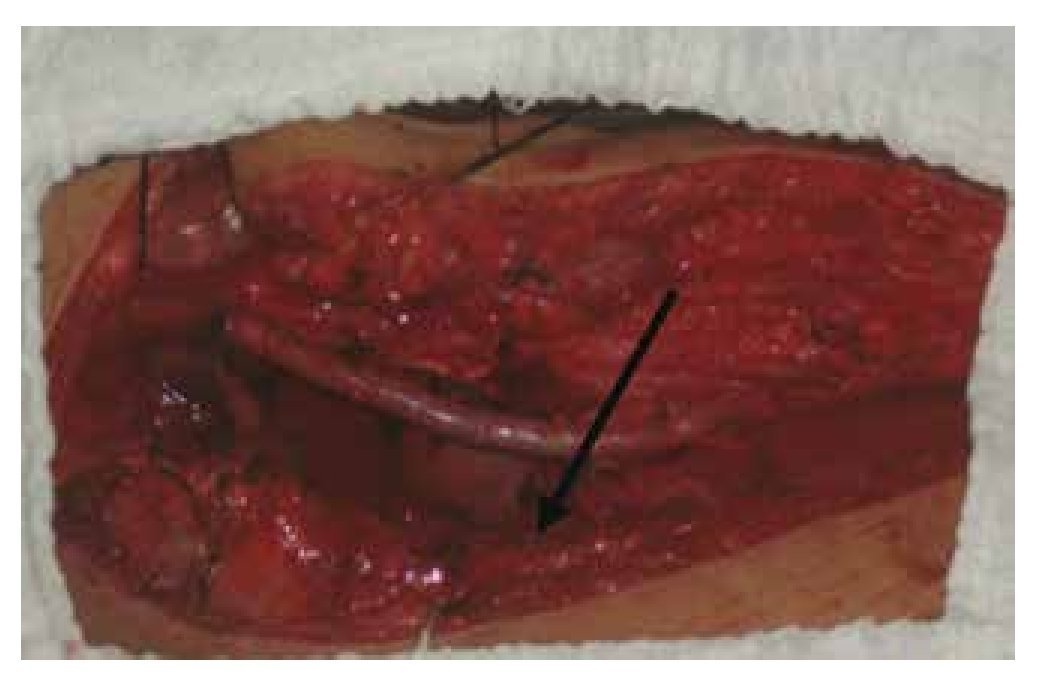
Figure 5 reversed saphenous graft in the femoral artery.
Discussion
Lower extremity pseudoaneurysms concur with global trauma statistics, being more frequent in young male adults. The pathophysiology consists of the result of the energy dissemination of the surrounding tissue, the expansive wave, projectile fragmentation or bone damaging the vascular wall, injuring the endothelial and causing a thrombus.3
Chronic traumatic aneurysm is developed by the partial or complete absorption of the periarterial hematoma at a fibrous sac level which is surrounded by the adjacent tissue. In general, the term “traumatic aneurysm” is utilized to refer to pseudoaneurysms, whether they are acute or chronic. Pseudoaneurysms must be treated as soon as possible, because of their risk of rupture or thrombosis.3 In our patient the diagnosis was made 4 months after the event.
The typical clinical picture starts with a lump with progressive growth and pain and limitation in the extremity’s functionality. During physical examinations there may be tissue pallor and edema, and pulsations and bruits over the lump. Most often there is an absence or decrease of intensity of the distal pulse; however, this is a critical point. In a study by Peck, he concluded that it is possible to feel a distal pulse in 10% of patients with a severe arterial injury,4 just as with our patient.
The most common vascular injuries occur in the femoral arteries (37.3%), as it was in our case, the popliteal arteries (27.8%) and the axillary and brachial arteries (23.5%).1
The diagnosis is made through physical examination and confirmed with an imaging study. The first study used is the color Doppler ultrasound, because it is a non-invasive method with excellent sensitivity and specificity which provides diagnostic, but not therapeutic, information. Even though the “gold standard” is still the arteriography, more importance has been given to non-invasive studies like the angiotomography with 3D reconstruction. It is used because of its diagnostic and therapeutic evaluation; it provides detailed information about the dimensions, morphology and anatomy of the pseudoaneurysm.5 This was the study utilized in our case.
When an aneurysm is larger than 2.5 cm, it is considered “surgical” because of the risk of complications, such as a thromboembolism or a rupture. The surgical treatment includes open surgical repair, compression and injection of thrombin guided by ultrasound, embolization or endovascular repair with stent.3,5
Endovascular repair is not used routinely for the treatment of femoral pseudoaneurysms. In general, it is used when the patient presents contraindications for conventional surgery.6 Open surgical repair must be the first treatment option for late complications of arterial injuries such as fistulas and pseudoaneurysms, using end-to-end anastomosis; however when it is not possible, an inverted saphenous venous graft should be used, because it is more resistant to infection and has a longer duration,7 as was done in our case.
Therefore, we suggest our patients with penetrating wounds located over the vascular trajectory to rule out a vascular injury through an imaging study, even when there is no clinical evidence of such injury. The risk of not diag- nosing a vascular injury is the posterior emergence of an arterial-venous fistula or a pseudoaneurysm which can bring severe complications if not treated in time, because they can cause massive bleeding and possibly loss of the limb.
Conclusion
Currently, vascular injuries are rising with the increase in violence and crime within society. Physical examination is not enough in order to diagnose vascular injuries; therefore, non-invasive and invasive methods must be used in order to exclude possible complications when necessary. Despite all the advances in endovascular interventionism, the first treatment option for this pathology is conventional surgery which consists of a resection of the pseudoaneurysm and reconstruction with an inverted saphenous graft or a prosthetic graft.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
No financial support was provided.
Received: December 2013;
Accepted: January 2014
* Corresponding author:
General Surgery Services,
“Dr. José Eleuterio González” University Hospital.
Francisco I. Madero and Gonzalitos Avenue,
Mitras Centro, Z.P. 64460, Monterrey, N.L., Mexico.
Telephone: (81) 8346 7198. Cell Phone: 5566945497.
E-mail address: mgomezuanl@gmail.com (M. A. Gómez-Álvarez).