



Acute intermittent porphyria (AIP) is one of the 4 types of acute porphyria presenting with neurological or psychiatric symptoms. In young adults with no specific history, the disease can manifest as encephalopathy associated with neuroimaging abnormalities that may be interpreted in numerous ways. Typical MRI findings resemble those seen in posterior reversible encephalopathy syndrome (PRES), which resolve with medical treatment. We describe the case of a young patient with AIP presenting as epilepsy and MRI alterations compatible with PRES.
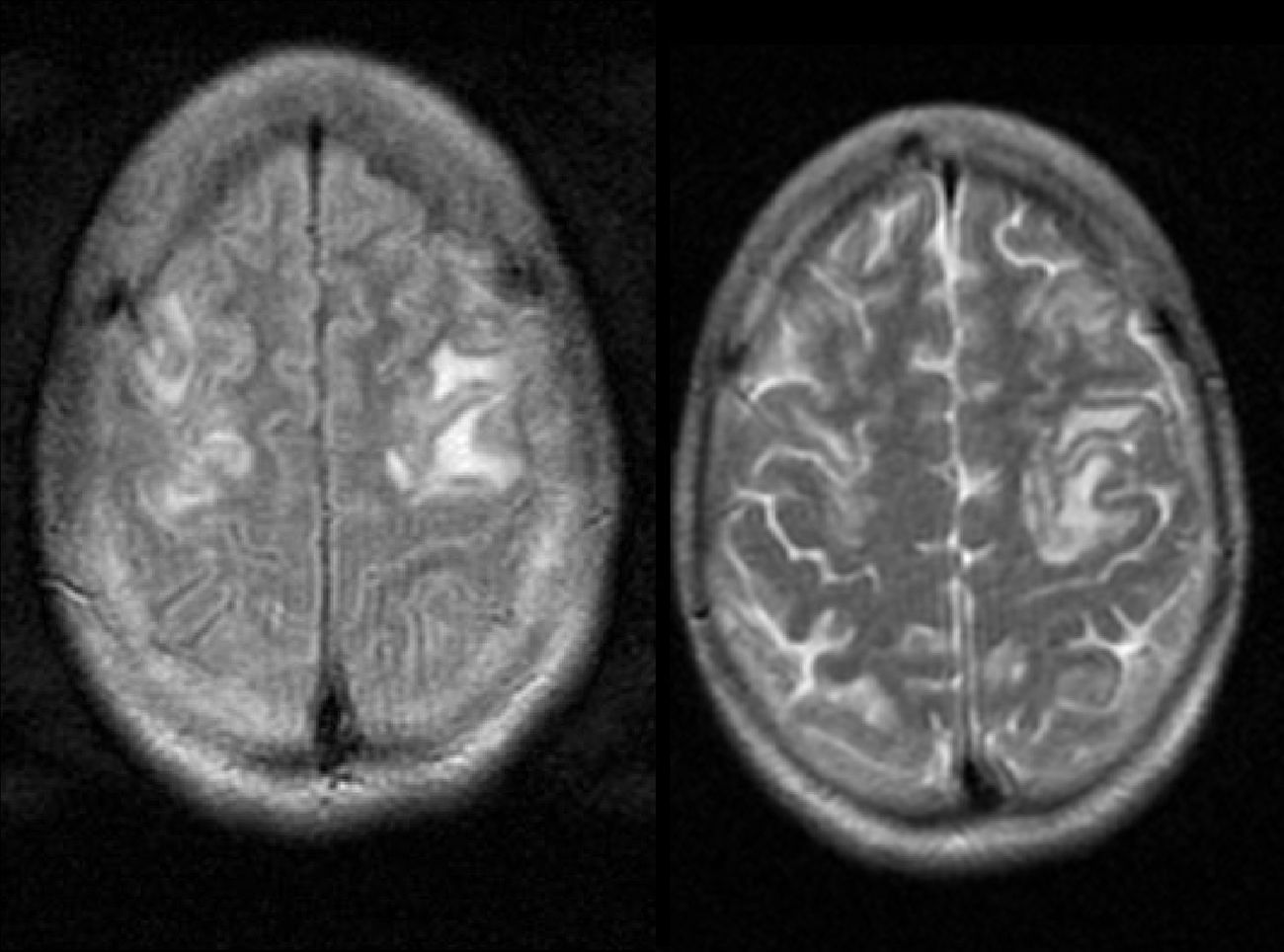
Our patient was a 23-year-old woman with no relevant medical history who experienced a loss of consciousness followed by 2 tonic–clonic seizures that resolved after treatment with midazolam. Upon arriving at the emergency department, she underwent a CT scan and laboratory tests, which yielded normal results except for mild hyponatraemia. She was discharged after a 24-hour observation period and instructed to take levetiracetam. One day later, she returned to our hospital due to another seizure and symptoms of disorientation and agitation; she was treated with haloperidol. She was admitted to the neurology department for a thorough study. Basic biochemical, blood, and serological tests, blood cultures, autoimmune studies, and a lumbar puncture all showed normal results, including normal coagulation and iron metabolism, and normal levels of vitamin B12 and folic acid. However, our patient continued to experience episodes of disorientation, agitation, and fluctuations in level of consciousness, which coincided on one occasion with severe hyponatraemia (114mEq/L). A brain MRI revealed bilateral cortical and subcortical frontal lesions, which were hypointense on T1-weighted sequences, hyperintense on T2-weighted sequences (Fig. 1), and hyperintense on apparent diffusion coefficient sequences.

Given the patient's clinical symptoms, hyponatraemia, and neuroimaging findings, we suspected viral/autoimmune encephalitis and AIP. The diagnosis of AIP was confirmed when a urine test revealed increased levels of total porphyrin (257μg/24hours [normal range: 25-220μg/24hours]), uroporphyrin (200μg/dL [normal values<2μg/dL]), porphobilinogen (PBG) (216mg/24hours [normal values<2.5mg/24hours]), and delta-aminolevulinic acid (delta-ALA) (105.2mg/24hours [normal range, 0-3.4mg/24hours]). We studied the HMBS gene by direct sequencing and detected 2 heterozygous variants: c.83G>T (p.S28I) and c.825+7G>T (IVS12+7G>T).
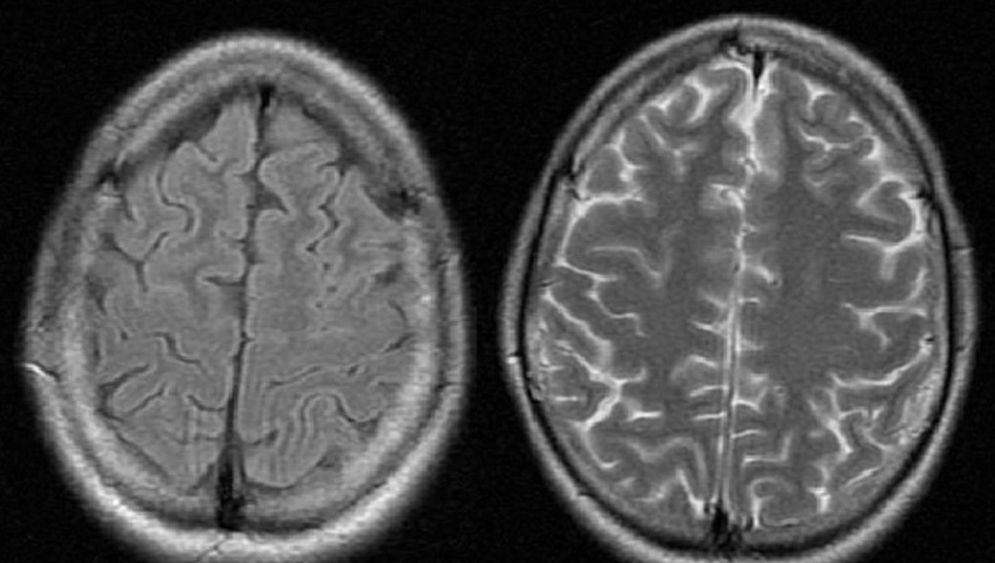
The patient was treated with beta-blockers and a carbohydrate-rich diet; her alterations of consciousness, disorientation, and agitation resolved, leaving no sequelae. In a follow-up consultation 2 months later, she was stable and adhering well to her new diet; MRI showed that lesions had disappeared (Fig. 2).

Porphyrias are a group of rare, heritable diseases which interrupt normal synthesis of the haem group in haemoglobin. AIP is the most common of all acute porphyrias, a group that includes hereditary coproporphyria (HC), porphyria variegata (PV), and delta-aminolevulinic acid dehydratase porphyria (ALAD-P).1 Acute porphyria may manifest with severe episodes that may be triggered by infections, alcohol, drugs, or stress, among other factors. Both men and women can inherit AIP; however, the disease is 5 times more likely to be expressed in women, especially during the third decade of life.1,2 Neurological symptoms are common and may be fatal in 1% of the cases. Autonomic dysfunction manifests as abdominal pain, nausea, vomiting, diarrhoea, hypertension, and tachycardia. Peripheral nervous system involvement may cause paraesthesia, generalised weakness, and respiratory paralysis. Agitation, disorientation, anxiety, and seizures result from central nervous system involvement.3,4 Patients with AIP frequently show electrolyte alterations, the most common being hyponatraemia, which occurs in 40% of the cases. This is thought to be due to gastrointestinal sodium loss, fluid overload, and reduced secretion of antidiuretic hormone.5
Acute porphyria is difficult to diagnose since symptoms are highly variable and non-specific. If it is suspected, a urine test must be conducted during the episode. Several theories have been proposed to explain the mechanism of neurotoxicity in AIP, including accumulation of haem precursors in neurons, which would result in dysfunction of the Na+/K+ pump, altering membrane potentials and leading to neuronal cell death and axonal degeneration.6
In acute porphyria, ALA and PGB levels in urine tests are more than 10 times higher than normal, as seen in our patient.7,8 Levels of these 2 components are high in HC and PV, although these increases are less marked and long-lasting than in AIP. Increased ALA levels can also be found in other metabolic diseases, including lead poisoning and ALAD-P.8 In the latter, total porphyrin levels in urine are not elevated, which helps differentiate ALAD-P from the other 3 types of acute porphyria. Coproporphyrin levels are very high in HC; this diagnosis was ruled out in our patient's case since she displayed normal levels of coproporphyrin. In PV and HC, symptoms are usually neuropsychiatric and cutaneous, whereas in our patient the disease initially manifested as seizures, chronic abdominal pain, paraesthesia, hypertension, and no skin lesions. These clinical findings, together with the results from the urine analysis, are more indicative of AIP.
Genetic testing is considered the gold standard diagnostic tool for acute porphyrias. The mutations in our patient were uncertain since we identified 2 previously undetected variants. The first of these (c.83G>T) significantly alters its protein and may therefore be the cause of the disease, whereas the second (c.825+7G>T) seems to be a polymorphism illustrating the heterogeneity of the mutations that cause AIP.
Neuroimaging studies are also useful for the differential diagnosis of AIP. The most frequent manifestation of the disease is PRES,5 a clinical and radiological entity with characteristic features on CT and MR images of the central nervous system.2,4,7 Typical neuroimaging findings in PRES include cortical vasogenic oedema. However, despite its name, these lesions are rarely located exclusively in the posterior area of parieto-occipital white matter; rather, the frontal lobes, basal ganglia, and cerebellum are more commonly affected.8 In a recently published study of FLAIR and DWI sequences in PRES, most of the patient sample (54%) displayed exclusively frontal involvement,8 in another study, 77% of the patients with frontal involvement also showed parieto-occipital involvement.9 In MRI, lesions are iso- or hypointense on T1 and hyperintense on T2.10,11 Our patient displayed hypointensities on T1 and hyperintensities on T2 in both frontal lobes (Figs. 1 and 2). DWI MRI is also useful since it helps differentiate between oedema secondary to a cytotoxic process (as in stroke) and vasogenic oedema.12,13 Diffusion-weighted MR images reveal increased signal intensity in cytotoxic oedema, whereas in vasogenic oedema (occurring in PRES) MRI shows iso- or hypointense lesions.14,15 In the context of intense or prolonged seizures, the literature describes MRI changes in the form of hyperintensities in cortico-subcortical areas on T2, which points to fluid overload. These lesions show restricted diffusion in diffusion sequences, which is more typical of cytotoxic oedema than of vasogenic oedema.14
The pathophysiology of PRES is not well known. The vascular hypothesis postulates that peripheral vasospasm occurs during an attack of porphyria and causes brain manifestations resembling those of malignant hypertension.15,16 Other possible mechanisms may be the neurotoxic effects of the increase in porphyrins and their precursors, or a deficit of cofactors in the synthesis of the haem group.16
The differential diagnosis of PRES includes acute ischaemic stroke, cerebral venous thrombosis, pontine encephalopathy in the context of mitochondrial encephalomyopathy (MELAS), Creutzfeldt-Jakob disease, and cerebral gliomatosis.17,18 These entities can be ruled out based on the patient's clinical history, examination, and laboratory and neuroimaging findings.
The case presented here proves once again that AIP can have an insidious onset with common and highly variable neurological symptoms. MRI is a useful diagnostic tool for acute porphyrias typically manifesting with PRES, whose symptoms will remit when properly treated.
FundingThe authors have received no private or public funding for this case report.
Conflict of interestThe authors have no conflict of interest to declare.
Please cite this article as: Rivero Sanz E, Camacho Velásquez JL, Santos Lasaosa S, Tejero Juste C. Cambios en la neuroimagen en paciente con síndrome de encefalopatía posterior reversible por porfiria aguda intermitente. Neurología. 2016;31:580–583.
