



Many studies highlight that an impaired ability to communicate is one of the key clinical features of Alzheimer disease (AD).
ObjectiveTo study temporal organisation of speech in an oral reading task in patients with AD and in matched healthy controls using a semi-automatic method, and evaluate that method's ability to discriminate between the 2 groups.
Subjects and methodsA test with an oral reading task was administered to 70 subjects, comprising 35 AD patients and 35 controls. Before speech samples were recorded, participants completed a battery of neuropsychological tests. There were no differences between groups with regard to age, sex, or educational level.
ResultsAll of the study variables showed impairment in the AD group. According to the results, AD patients’ oral reading was marked by reduced speech and articulation rates, low effectiveness of phonation time, and increases in the number and proportion of pauses. Signal processing algorithms applied to reading fluency recordings were shown to be capable of differentiating between AD patients and controls with an accuracy of 80% (specificity 74.2%, sensitivity 77.1%) based on speech rate.
ConclusionAnalysis of oral reading fluency may be useful as a tool for the objective study and quantification of speech deficits in AD.
Numerosos estudios han puesto de manifiesto que la alteración en la capacidad comunicativa es uno de los síntomas característicos de la enfermedad de Alzheimer (EA).
ObjetivoEstudiar la organización temporal del habla en una tarea de lectura en un grupo de pacientes con EA y otro de controles sanos, utilizando un procedimiento semiautomático, así como valorar su capacidad para discriminar entre ambos grupos.
Sujetos y métodoSe aplicó una prueba de lectura a 70 sujetos: 35 con EA y otros tantos controles. Antes del registro del habla, los sujetos fueron sometidos a una batería de pruebas neuropsicológicas. Los grupos no diferían en edad, sexo o nivel de estudios.
ResultadosTodas las variables analizadas se mostraron alteradas en el grupo con EA. Los resultados señalan que la lectura de los pacientes con EA se caracteriza por una reducida velocidad de elocución y articulación, una baja efectividad del tiempo de fonación, así como en un incremento del número y la proporción de las pausas. Los algoritmos de procesamiento de la señal aplicados a las grabaciones de fluidez lectora demostraron su capacidad para discriminar entre ambos grupos con una precisión del 80% (especificidad 74,2%; sensibilidad 77,1%) mediante la velocidad de elocución.
ConclusiónEl análisis de la fluidez de lectura oral puede representar una herramienta potencial para el análisis objetivo y la cuantificación de los déficits del lenguaje en la EA.
Distinguishing early stages of Alzheimer disease (AD) from the cognitive impairment associated with normal ageing is a challenge. Rapid ageing among the population has drawn attention to the need to develop instruments for diagnosing AD by first identifying early (premorbid) markers allowing us to determine the nature, type, and severity of the disease.
Numerous studies have shown that changes in language are some of the most apparent symptoms in AD.1 They affect between 8% and 10% of the population in early stages of the disease and become more severe in later stages.2 It is well-documented that patients with AD show signs of language deficit long before their diagnosis is confirmed,3,4 and this tendency is especially useful for detecting mild cognitive decline.5 The meta-analysis performed by Bäckman et al.6 concludes that language decline shows a significant effect size for cognitive decline in preclinical patients with AD, years before the clinical diagnosis has been established. Both semantic verbal fluency (SVF) and phonological verbal fluency (PVF) tests are widely used in diagnosing AD, and they are considered reliable indicators of language deterioration7 in early detection of both AD and mild cognitive impairment (MCI).8
Reading tests have been used in diagnosing AD because of the difficulty of simultaneous processing of decryption, phonological, and semantic tasks.9 The National Adult Reading Test,10 which is the most widely used test, evaluates reading an English-language text out loud. It is a quick test featuring uncommon and irregularly spelled words, and it may be used for detecting MCI11 as well as to gauge AD progression.12
Multiple studies have shown that reading ability is largely spared in AD since the task is partially automated.13 While there are no detectable changes in reading ability in the early stages of the disease,14 researchers have observed a significant decline in reading fluency in advanced stages,15 although patients remain able to read short sentences.16,17
The purpose of this study is to analyse the temporal parameters of reading fluency by using an automatic, objective evaluation procedure. We will also evaluate this test's ability to discriminate between asymptomatic subjects and those with AD.
MethodStatistical designThe study was framed with a cross-sectional, analytical, observational, and retrospective design.
PatientsThe sample was composed of 70 subjects with no prior history of alcohol abuse or drug consumption and no symptoms of depression (Geriatric Depression Scale score <10).
The group with AD (n=35, 77.1% male and 22.9% female) consisted of patients at the national centre of reference for the care of patients with AD and other forms of dementia (CREA) in Salamanca, Spain. All patients had been diagnosed according to criteria established by the National Institute of Neurological and Communicative Disorders and the Alzheimer's Disease and Related Disorders Association. Their GDS score was 4 (mild AD).18 Patients in this phase exhibit a slight language deficit in the processes of object naming and word comprehension. This is associated with anomic aphasia or impaired ability to search semantic memory. All patients had been enrolled in the CREA cognitive stimulation programme. Conditions for inclusion were retaining adequate communication skills (auditory perception and articulation) and the ability to read and follow instructions. The control group (n=35, 80.6% men and 19.4% women) was composed of University of Salamanca students enrolled in the Spanish university programme for adults older than 55. All spoke Spanish fluently and they had no prior history of brain damage, neurological disorders, psychosis, or substance abuse. None of the controls had cognitive impairment or concerns about memory loss. Two subjects in the initial sample were excluded due to having scores ≤23 points on the Mini-Mental State Examination (MMSE).19
MaterialsAll participants completed a neuropsychological evaluation consisting of the following tests:
- -
MMSE,19 the most widespread test for evaluating mental state, offers the most commonly used severity index for dementia. MMSE explores 5 cognitive areas: orientation, registration, attention and calculation, and recall and language. The maximum total score is 30 points.
- -
CVT, The test created by Cuetos-Vega et al.20 has a high discriminant ability for cognitive impairment (sensitivity 0.96%, specificity 0.86%). This test includes 10 tasks, half of which are language-related: (1) SVF; (2) PVF; (3) naming by definition; (4) object naming; (5) verbal fluency for proper names; (6) naming with proper names; (7) immediate recall of a word list; (8) deferred recall of a word list; and (10) delayed recall of data about a person. The maximum total score is 100 points.
- -
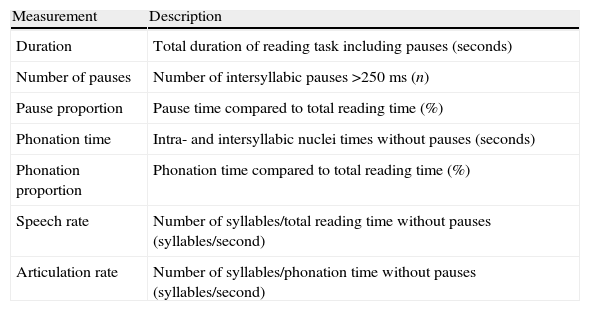
Speech was recorded during the reading task using a professional Fostex® FR-2LE recorder with a resolution of 24 bits and a 48kHz sampling rate, and an AKG D3700S cardioid microphone. All samples were edited using Praat® voice analysis software, version 5.1.42.21 We obtained 7 reading fluency indexes (see Appendix A) by using scripts evaluating the following: (1) total duration of the reading task; (2) number of pauses (silences >250ms); (3) pause proportion; (4) phonation time; (5) phonation–time ratio; (6) speech rate; and (7) articulation rate.
All patients signed an informed consent form according to the protocols approved by the ethics committees at participating institutions. The procedure was carried out in 2 sessions. In the first session, we registered patients’ biographical information and administered the MMSE and CVT. Recordings were made in the second session, held 3 to 5 days later. The subjects’ task was to read the first paragraph of El ingenioso hidalgo don Quijote de la Mancha by Miguel de Cervantes. The text was displayed on a screen in 48-point size for easier reading. The examiner made a recording of subjects’ attempts in a quiet but not soundproof room. The microphone was placed 8cm from the speaker's mouth and at an angle of approximately 45° in order to minimise breath noise.
ResultsWe did not initially find significant differences between subjects in each group in the areas of age, years of education, or sex distribution (χ12=0.14; P=.96).
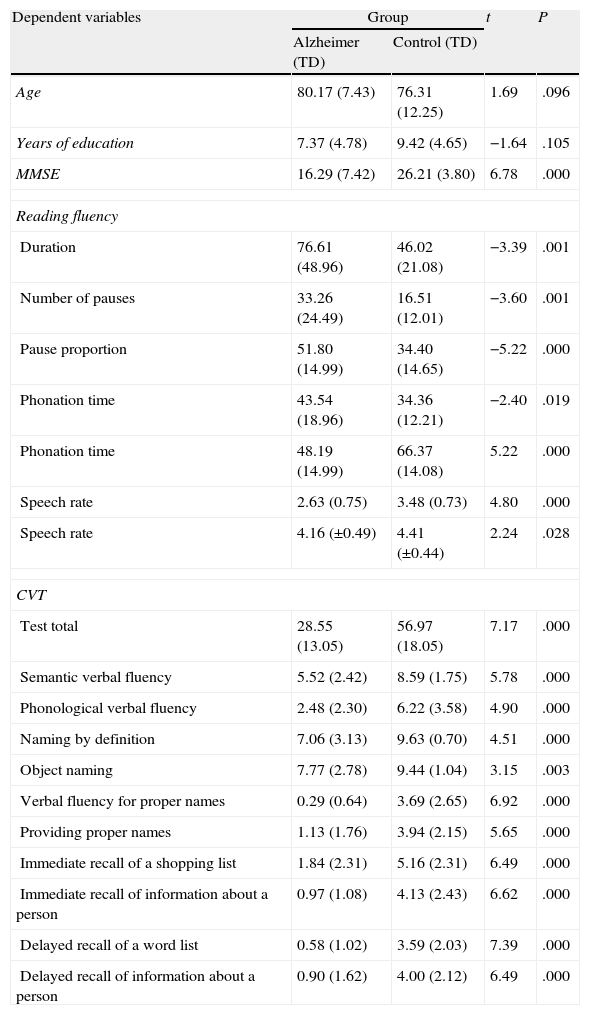
Comparison of means analysis for fluency parameters and results from neuropsychological tests showed significant differences between all study variables (Table 1).
Demographic information, descriptive statistics, and comparison of means of study variables between both groups.
| Dependent variables | Group | t | P | |
| Alzheimer (TD) | Control (TD) | |||
| Age | 80.17 (7.43) | 76.31 (12.25) | 1.69 | .096 |
| Years of education | 7.37 (4.78) | 9.42 (4.65) | −1.64 | .105 |
| MMSE | 16.29 (7.42) | 26.21 (3.80) | 6.78 | .000 |
| Reading fluency | ||||
| Duration | 76.61 (48.96) | 46.02 (21.08) | −3.39 | .001 |
| Number of pauses | 33.26 (24.49) | 16.51 (12.01) | −3.60 | .001 |
| Pause proportion | 51.80 (14.99) | 34.40 (14.65) | −5.22 | .000 |
| Phonation time | 43.54 (18.96) | 34.36 (12.21) | −2.40 | .019 |
| Phonation time | 48.19 (14.99) | 66.37 (14.08) | 5.22 | .000 |
| Speech rate | 2.63 (0.75) | 3.48 (0.73) | 4.80 | .000 |
| Speech rate | 4.16 (±0.49) | 4.41 (±0.44) | 2.24 | .028 |
| CVT | ||||
| Test total | 28.55 (13.05) | 56.97 (18.05) | 7.17 | .000 |
| Semantic verbal fluency | 5.52 (2.42) | 8.59 (1.75) | 5.78 | .000 |
| Phonological verbal fluency | 2.48 (2.30) | 6.22 (3.58) | 4.90 | .000 |
| Naming by definition | 7.06 (3.13) | 9.63 (0.70) | 4.51 | .000 |
| Object naming | 7.77 (2.78) | 9.44 (1.04) | 3.15 | .003 |
| Verbal fluency for proper names | 0.29 (0.64) | 3.69 (2.65) | 6.92 | .000 |
| Providing proper names | 1.13 (1.76) | 3.94 (2.15) | 5.65 | .000 |
| Immediate recall of a shopping list | 1.84 (2.31) | 5.16 (2.31) | 6.49 | .000 |
| Immediate recall of information about a person | 0.97 (1.08) | 4.13 (2.43) | 6.62 | .000 |
| Delayed recall of a word list | 0.58 (1.02) | 3.59 (2.03) | 7.39 | .000 |
| Delayed recall of information about a person | 0.90 (1.62) | 4.00 (2.12) | 6.49 | .000 |
MMSE: Mini-Mental State Examination; VCT: Cuetos-Vega test.
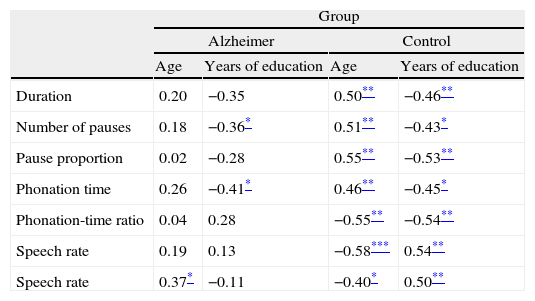
A correlation analysis showed that articulation rate was the only variable with a significant correlation to age (r2=0.37; P<.05), while years of education were correlated with the number of pauses (r2=–0.36; P<.05) and phonation time (r2=–0.41; P<.05). We must point out that in order for a test to be used in dementia screening, it must not be excessively sensitive to the effects of age and education within the dementia group. In contrast, all fluency variables correlated significantly with age and years of education in the control group, as would be expected in normal ageing (Table 2).
Correlations between reading fluency variables and age and years of education.
| Group | ||||
| Alzheimer | Control | |||
| Age | Years of education | Age | Years of education | |
| Duration | 0.20 | −0.35 | 0.50** | −0.46** |
| Number of pauses | 0.18 | −0.36* | 0.51** | −0.43* |
| Pause proportion | 0.02 | −0.28 | 0.55** | −0.53** |
| Phonation time | 0.26 | −0.41* | 0.46** | −0.45* |
| Phonation-time ratio | 0.04 | 0.28 | −0.55** | −0.54** |
| Speech rate | 0.19 | 0.13 | −0.58*** | 0.54** |
| Speech rate | 0.37* | −0.11 | −0.40* | 0.50** |
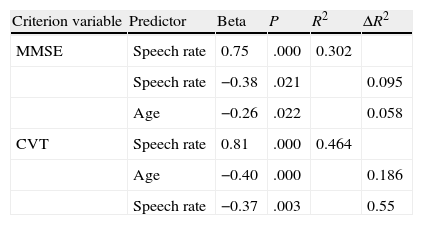
In order to evaluate the predictive capacity of reading fluency variables, we completed a stepwise regression analysis using scores from neuropsychological tests, age, and years of education. Three variables were shown to have a significant predictive capacity on subjects’ total scores on either the MMSE or the CVT: speech rate, articulation rate, and age (Table 3), which explained 45.5% and 70.05% of the variance in MMSE and CVT scores, respectively. The rest of the variables were excluded from the model. Speech rate was the variable with the best predictive capacity; articulation rate, in turn, had a lower predictive capacity but this additional information was significant in the regression equation.
Stepwise regression analysis of temporal parameters of reading fluency on total MMSE and CVT scores.
| Criterion variable | Predictor | Beta | P | R2 | ΔR2 |
| MMSE | Speech rate | 0.75 | .000 | 0.302 | |
| Speech rate | −0.38 | .021 | 0.095 | ||
| Age | −0.26 | .022 | 0.058 | ||
| CVT | Speech rate | 0.81 | .000 | 0.464 | |
| Age | −0.40 | .000 | 0.186 | ||
| Speech rate | −0.37 | .003 | 0.55 |
MMSE: Mini-Mental State Examination; CVT: Cuetos-Vega test.
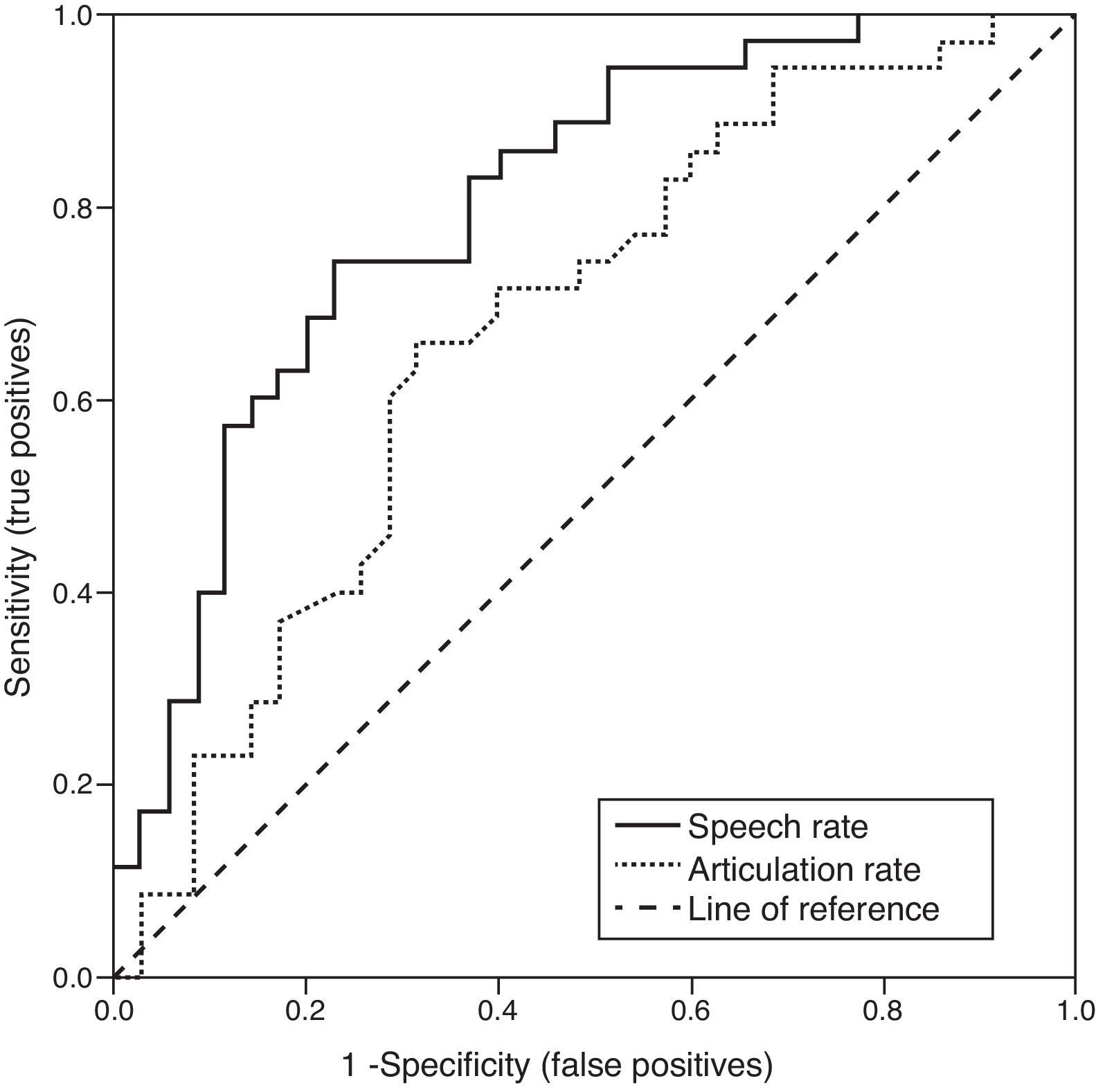
ROC curve analysis was used to calculate sensitivity and specificity of reading fluency variables with a predictive capacity for neurological test results (speech and articulation rate) compared to clinical diagnosis (Fig. 1). This analysis revealed a greater area under the curve (AUC) for speech rate (0.80, DT=.05; z=5.71, P<.001) than for articulation rate (0.67, DT=0.06; z=2.67, P<.001). The best cut-off point for speech rate was >3.08 syllables per second (sensitivity 74.29%, 95% CI: 56.7–87.5; specificity, 77.14, 95% CI: 59.9–89.6), with a likelihood ratio positive (LR+) of 3.25 (95% CI: 2.5–4.2) and a likelihood ratio negative (LR−) of 0.33 (95% CI: 0.1–0.8). The optimal cut-off point for articulation rate was >4.27 syllables per second (sensitivity 65.61%, 95% CI: 47.8–80.9; specificity 68.57%, 95% CI: 50.7–83.1), with a likelihood ratio positive (LR+) of 2.09 (95% CI: 1.5–2.9) and likelihood ratio negative (LR−) of 0.50 (95% CI: 0.3–1).
Discussion
The purpose of this study was to analyse the temporal parameters of reading fluency by using an automatic, objective evaluation procedure, and to evaluate this test's ability to discriminate between asymptomatic subjects and those with AD.
Results are able to discriminate between groups of patients with moderate cognitive impairment (GDS 4) and asymptomatic control subjects.
Concurrent validity is demonstrated by the test's acceptable results for diagnostic accuracy as expressed by the area under the ROC curve, especially for speech rate, and by the test's sensitivity and specificity levels. However, our results do not allow us to conclude that reading fluency analysis has excellent diagnostic accuracy; the area under the ROC curve did not reach the level of 0.90.
The 2 temporal parameters with the greatest discriminatory capacity were speech rate and articulation rate. Furthermore, earlier studies have shown that both variables can discriminate groups of subjects with MCI from controls,22,23 although we did not discover any studies with results similar to those obtained here in patients with AD.
These results are consistent with those obtained in tasks in which patients read rarely used words and irregular verbs. Studies of such tasks have demonstrated poorer performance associated with AD progression.9,17
We should state that reading capacity and reading comprehension are different concepts, and that while reading capacity may remain relatively intact, comprehension is more profoundly impaired during later stages of the disease.24,25 Petersen et al.26 showed that subjects with AD are able to read words without activating any of the areas of the brain linked to semantic association, which implies that they may read aloud without understanding the meaning of the words.
Although the number of pauses and their proportion have been shown to be significantly higher in the AD group, our results do not assign these factors as much importance as do other projects studying spontaneous verbal fluency.27 These studies regarded pauses as having discriminant validity for impairment, in addition to being an early marker of AD.
The CVT was shown to be more sensitive than the MMSE for predicting reading fluency results. We believe the reason is as follows: along with the test's high sensitivity and specificity levels,20 5 of the test's 10 tasks evaluate language, which makes the CVT more sensitive for evaluating language-related factors than the MMSE.
Our study also revealed a positive effect of level of education on reading fluency results. In the context of the studies evaluating the role of cognitive reserve28 in AD progression, the results may indicate that cognitive reserve has potential for slowing impairment of reading fluency. However, the nature of this study does not permit us to confirm results by studies showing that cognitive reserve slows AD progression,29 or other studies claiming an inverse effect.30
We must point out that reading fluency tests are limited in certain cases by variables that include presence of visual deficiencies, age, and level of education, which also affect results on traditional verbal fluency tests. However, these results show that evaluating temporal parameters of reading fluency is a technique that can discriminate between subjects with AD and asymptomatic controls. It is a relatively simple and fast procedure that causes the patient minimal discomfort, and it also meets many of the requirements established for neuropsychological tests that evaluate forms of dementia.31
While it is true that doctors often do not possess the equipment which we used to perform reading fluency analysis in this study, we feel that this is no obstacle to the procedure being used as a complementary test to measure language changes in AD which often remain undetected, even by experienced professionals. Furthermore, the procedure described in this study lets doctors calculate objective language impairment indexes that go beyond the simple word counts used in verbal fluency tests.
Future projects must evaluate the utility of the procedure described in this study in patients with MCI and include longitudinal studies to determine its usefulness as an AD screening method.
Lastly, we conclude that analysing temporal parameters for reading fluency, especially speech and articulation rates, allowed us to distinguish between asymptomatic subjects and patients in early stages of AD. The analysis also provided information about the state of language in these patients.
FundingThis study was performed within the framework of the cooperative research agreement between Instituto de Neurociencias de Castilla y León (InCyL) and Centro de Referencia Estatal de Atención a Personas con Enfermedad de Alzheimer y otras Demencias (CRE Alzheimer, Salamanca; IMSERSO).
Conflicts of interestThe authors have no conflicts of interest to declare.
| Measurement | Description |
| Duration | Total duration of reading task including pauses (seconds) |
| Number of pauses | Number of intersyllabic pauses >250ms (n) |
| Pause proportion | Pause time compared to total reading time (%) |
| Phonation time | Intra- and intersyllabic nuclei times without pauses (seconds) |
| Phonation proportion | Phonation time compared to total reading time (%) |
| Speech rate | Number of syllables/total reading time without pauses (syllables/second) |
| Articulation rate | Number of syllables/phonation time without pauses (syllables/second) |
Please cite this article as: Martínez-Sánchez F, et al. Análisis de la fluencia lectora en pacientes con la enfermedad de Alzheimer y controles asintomáticos. Neurología. 2013;28:325–31
