



The incidence of stroke in Spain has been evaluated in several studies, whose results are highly variable and not comparable. No studies of stroke have analysed epidemiological changes in younger patients.
MethodWe conducted a retrospective observational study using the Spanish health system's Minimum Data Set and included all patients older than 19 hospitalised due to stroke (ICD-9-CM codes 434.01, 434.11, 434.91, 430, 431, 432.9, 436, and 435) between 2002 and 2013. The analysis was performed using joinpoint regression.
ResultsA total of 39321 patients were identified (47.25% were women); 3.73% were aged 20-44, 6.29% were 45-54, 11.49% were 55-64, 23.89% were 65-74, and 54.60% were >74 years. The hospitalisation rate due to ischaemic stroke has increased significantly in men aged 45-54 (+6.7%; 95% CI, 3.3-10.2) and in women aged 20-44 and 45-54 (+6.1%; 95% CI, 0.8-11.7 and +5.7%; 95% CI, 3.0-8.4, respectively). We also observed a significant increase in the rate of hospitalisation due to ischaemic stroke in men aged over 74 (+4.2%; 95% CI, 1.3-7.2). The rate of hospitalisations due to transient ischaemic attack has also increased significantly whereas the rate of hospitalisations due to brain haemorrhage has stabilised over time.
ConclusionsOur results provide indirect evidence that the epidemiological profile of stroke is changing based on the increase in hospitalisation rates in young adults.
La incidencia del ictus en nuestro medio ha sido evaluada en diferentes estudios con amplia variabilidad y no comparables. Tampoco hay estudios que analicen los cambios epidemiológicos en pacientes más jóvenes.
MétodoEstudio retrospectivo observacional. Conjunto Mínimo Básico de Datos. Se seleccionó a todos los pacientes mayores de 19 años hospitalizados por ictus (códigos ICD-9-CM 434.01, 434.11, 434.91, 430, 431, 432.9, 436 y 435) en el periodo 2002-2013. Análisis mediante el método de regresión lineal segmentada.
ResultadosUn total de 39.321 casos fueron identificados. El 47,25% mujeres. Un 3,73% tenía entre 20-44 años, el 6,29% entre 45-54, el 11,49% entre 55-64, el 23,89% entre 65-74 y un 54,60% más de 74 años. Se demuestra un incremento significativo en la tasa de hospitalización por ictus isquémico en varones de 45-54 años, +6,7% (IC del 95%: 3,3-10,2) y en mujeres de 20-44 y 45-54 años, +6,1% (IC del 95%: 0,8-11,7) y+5.7% (IC del 95%: 3,0-8,4), respectivamente. También se observa un incremento significativo de la tasa de hospitalización de ictus isquémico en varones mayores de 74 años, +4,2% (IC del 95%: 1,3-7,2). El análisis para los ataques isquémicos transitorios reproduce lo que ocurre en el ictus isquémico. El mismo análisis para el caso de la hemorragia confirma una estabilización en las tasas de hospitalización en el tiempo.
ConclusionesEste estudio demuestra de una forma indirecta los cambios epidemiológicos que se están produciendo en el ictus. Existe suficiente evidencia que indica un cambio epidemiológico al aumentar la tasa de hospitalizaciones en adultos jóvenes.
Stroke is one of the most frequent causes of disability among adults worldwide.1 The epidemiology of the condition varies greatly between countries and over time; the reasons for this are not well understood.2 A systematic review of population-based studies published between 1970 and 2008 reported a decrease in the incidence of stroke in high-income countries and a considerable increase in low- and middle-income countries; incidence trends in Europe were not uniform.3 Some studies conducted in European populations have observed an increase in rates of hospitalisation due to cerebrovascular disease among people aged 30 to 65 years old.4 The increased incidence of stroke at younger ages has also been observed in the United States.5 This may be explained by a change in demographic risk factors for stroke.6
The incidence of stroke in our setting has been analysed in various studies with considerable methodological differences; differences in age limits do not allow us to compare their results. No studies have specifically analysed epidemiological changes among younger patients.7 One of the most recent epidemiological studies published in Spain estimated the incidence of stroke at 187 cases per 100000 person-years; stroke is more common in men and incidence peaks at the age of 85.8
The study objective was to analyse trends in stroke hospitalisation rates in Extremadura between 2002 and 2014, paying special attention to age- and sex-related differences. Data was gathered from the minimum basic dataset (MBDS), which has been shown to provide reliable information about hospital activity and has previously been used in stroke research.9,10
MethodsThis retrospective, observational study used the ALCOR clinical statistics analysis tool and the MBDS. This database is administrated by the Department of Health and Social Affairs of the autonomous community of Extremadura and gathers data from the region's public hospitals, including over 95% of all hospital discharges. Maintenance of the MBDS is regulated; the database undergoes periodic auditing. Since 2002, the MBDS has included comprehensive data from all health districts in Extremadura. The diagnostic criteria for stroke are defined according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
We selected all patients aged 20 years and older who had been admitted to hospital due to ischaemic stroke (ICD-9-CM codes 434.01, 434.11, and 434.91), haemorrhagic stroke (codes 430, 431, and 432.9), acute but ill-defined cerebrovascular disease (code 436), and transient ischaemic attack (TIA) (code 435). Our study included all patients discharged between 1 January 2002 and 31 December 2014 whose main diagnosis was among those mentioned above.
Crude hospitalisation rates were calculated using population estimates for the study period. We calculated sex- and age-specific rates (age groups 20 to 44, 45 to 54, 55 to 64, 65 to 74, and older than 74). To standardise rates by the direct method we used the standard European population in 1976 for the period 2002-2008 and the 2013 standard European population proposed by Eurostat for the period 2013 onwards. This process is necessary to adapt the population to Europe's current situation, especially due to population ageing and the enlargements of the European Union since the 1970s.
Statistical analysisWe performed a descriptive statistical analysis for the 4 conditions evaluated, stratifying data by sex and age group. A joinpoint regression analysis was performed to identify joinpoints indicating a statistically significant change in the slope of the linear function. This type of analysis identifies joinpoints indicating significant changes in a rate. The analysis starts with the smallest number of joinpoints, and tests whether one or more joinpoints are statistically significant and must therefore be added to the model. In the final model, each segment indicates a statistically significant change in the trend. This type of analysis also provides the average annual percentage change (AAPC) for each of these trends by means of general linear models, assuming a Poisson distribution. Crude and standardised hospitalisation trends were calculated using a Microsoft® Excel spreadsheet. Joinpoint regression analysis was performed with Joinpoint statistical software version 4.2.0.2 (Surveillance Research Programme, US National Cancer Institute). The software searches for the simplest model fitting the data using the weighted least-squares technique and estimates statistical significance using the Monte Carlo Permutation method. Statistical significance was set at P<.05.
EthicsData confidentiality was guaranteed in accordance with the Spanish legislation. Patient identification numbers were deleted from the database before authors used it in order to preserve patients’ confidentiality. Individual patients cannot therefore be identified either in this article or in the database. Informed consent was not necessary as all data were anonymous. Data use was authorised by the General Directorate for Health Planning, Training, and Quality of the regional government of Extremadura.
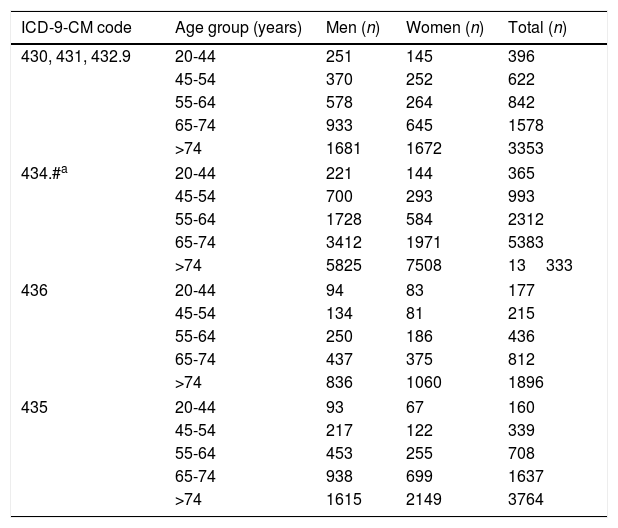
ResultsA total of 39321 patients aged 20 years and older were hospitalised with a main diagnosis of some type of acute cerebrovascular event during the study period. Women accounted for 47.25% of the sample (n=18555). By age, 3.73% of patients were 20 to 44 years old, 6.29% were 45 to 54, 11.49% were 55 to 64, 23.89% were 65 to 74, and 54.60% were older than 74. By condition, 82.7% had ischaemic events and 17.3% had haemorrhagic events; 22386 patients had ischaemic strokes, 6796 had haemorrhagic strokes, 3536 had acute but ill-defined cerebrovascular disease, and 6608 had TIAs. Table 1 shows the distribution by age, sex, and diagnosis of the patients hospitalised in our region during the study period.
Age and sex distribution of the number of patients aged 20 years and older admitted to hospital with a diagnosis of cerebrovascular disease, broken down by main diagnosis (2002-2014).
| ICD-9-CM code | Age group (years) | Men (n) | Women (n) | Total (n) |
|---|---|---|---|---|
| 430, 431, 432.9 | 20-44 | 251 | 145 | 396 |
| 45-54 | 370 | 252 | 622 | |
| 55-64 | 578 | 264 | 842 | |
| 65-74 | 933 | 645 | 1578 | |
| >74 | 1681 | 1672 | 3353 | |
| 434.#a | 20-44 | 221 | 144 | 365 |
| 45-54 | 700 | 293 | 993 | |
| 55-64 | 1728 | 584 | 2312 | |
| 65-74 | 3412 | 1971 | 5383 | |
| >74 | 5825 | 7508 | 13333 | |
| 436 | 20-44 | 94 | 83 | 177 |
| 45-54 | 134 | 81 | 215 | |
| 55-64 | 250 | 186 | 436 | |
| 65-74 | 437 | 375 | 812 | |
| >74 | 836 | 1060 | 1896 | |
| 435 | 20-44 | 93 | 67 | 160 |
| 45-54 | 217 | 122 | 339 | |
| 55-64 | 453 | 255 | 708 | |
| 65-74 | 938 | 699 | 1637 | |
| >74 | 1615 | 2149 | 3764 | |
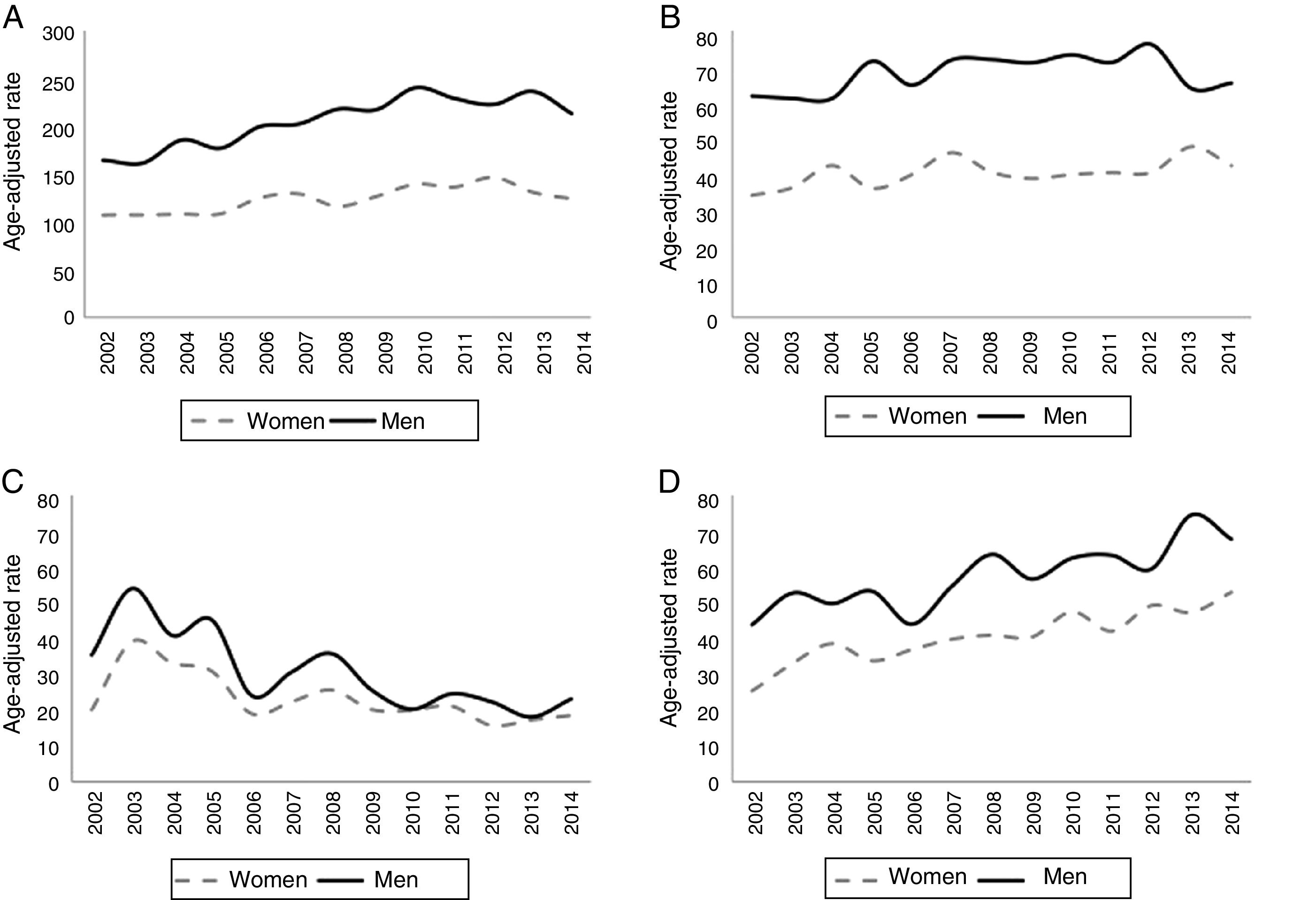
In general terms, the standardised hospitalisation rate (SHR) per 100000 person-years increased from 164.9 cases in 2002 to 213.2 cases in 2014 in men, and from 107.9 cases in 2002 to 124.0 in 2014 in women. The SHR for haemorrhagic stroke did not change significantly in men (61.8 cases in 2002 and 65.3 cases in 2014); in women, this rate was 34.1 cases in 2002 and 42.3 in 2014. The SHR for acute but ill-defined cerebrovascular disease decreased over time. The number of patients hospitalised due to TIA increased slightly during the study period. Fig. 1 shows the standardised rates of hospitalisation due to cerebrovascular disease per 100000 person-years during the study period.
 of hospitalisation due to cerebrovascular disease (number of cases per 100000 person-years) during the study period. (A) Ischaemic stroke (ICD-9-CM codes 434.01, 434.11, and 434.91). (B) Haemorrhagic stroke (ICD-9-CM codes 430, 431, and 432.9). (C) Acute but ill-defined cerebrovascular disease (ICD-9-CM code 436). D) Transient ischaemic attack (ICD-9-CM code 435).")
Standardised rates (direct method) of hospitalisation due to cerebrovascular disease (number of cases per 100000 person-years) during the study period. (A) Ischaemic stroke (ICD-9-CM codes 434.01, 434.11, and 434.91). (B) Haemorrhagic stroke (ICD-9-CM codes 430, 431, and 432.9). (C) Acute but ill-defined cerebrovascular disease (ICD-9-CM code 436). D) Transient ischaemic attack (ICD-9-CM code 435).
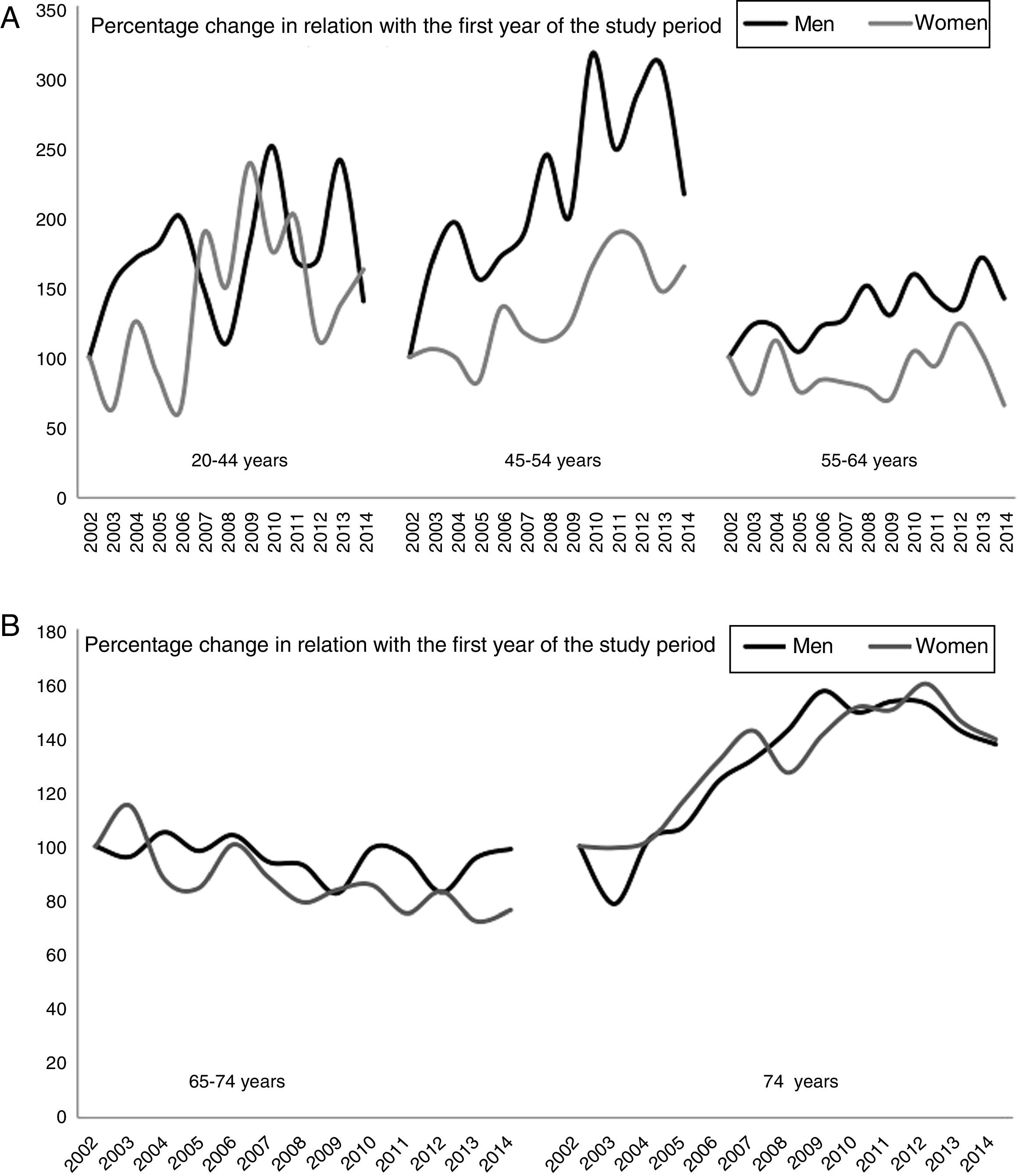
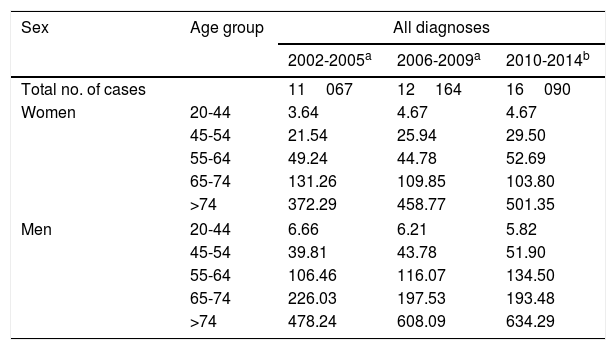
Table 2 shows the trends in hospitalisation rates over 3 periods for the different age and sex groups. Hospitalisation rates increased in both men and women younger than 65 and decreased slightly in both men and women aged 65 to 74. The sharpest increase was observed in patients older than 74. Fig. 2 shows the percentage change in crude rates of hospitalisation due to ischaemic stroke by age and sex. We provide a graphic representation of ischaemic stroke only as this was the group of greatest clinical interest. The graph shows an increase in relation to the first year in younger individuals, especially in those aged 20 to 54. A slight decrease is observed between the ages of 65 and 74.
Crude rates of hospitalisation for any cerebrovascular event per 100000 person-years in each period, by age and sex.
| Sex | Age group | All diagnoses | ||
|---|---|---|---|---|
| 2002-2005a | 2006-2009a | 2010-2014b | ||
| Total no. of cases | 11067 | 12164 | 16090 | |
| Women | 20-44 | 3.64 | 4.67 | 4.67 |
| 45-54 | 21.54 | 25.94 | 29.50 | |
| 55-64 | 49.24 | 44.78 | 52.69 | |
| 65-74 | 131.26 | 109.85 | 103.80 | |
| >74 | 372.29 | 458.77 | 501.35 | |
| Men | 20-44 | 6.66 | 6.21 | 5.82 |
| 45-54 | 39.81 | 43.78 | 51.90 | |
| 55-64 | 106.46 | 116.07 | 134.50 | |
| 65-74 | 226.03 | 197.53 | 193.48 | |
| >74 | 478.24 | 608.09 | 634.29 | |
 Percentage change in hospitalisation rates for ischaemic stroke, broken down by sex and age (individuals younger than 65 years). (B) Percentage change in hospitalisation rates for ischaemic stroke, broken down by sex and age (individuals older than 74 years). The 2002 hospitalisation rate was used as a reference; percentage changes are calculated in relation with the first year of the study period.")
(A) Percentage change in hospitalisation rates for ischaemic stroke, broken down by sex and age (individuals younger than 65 years). (B) Percentage change in hospitalisation rates for ischaemic stroke, broken down by sex and age (individuals older than 74 years). The 2002 hospitalisation rate was used as a reference; percentage changes are calculated in relation with the first year of the study period.
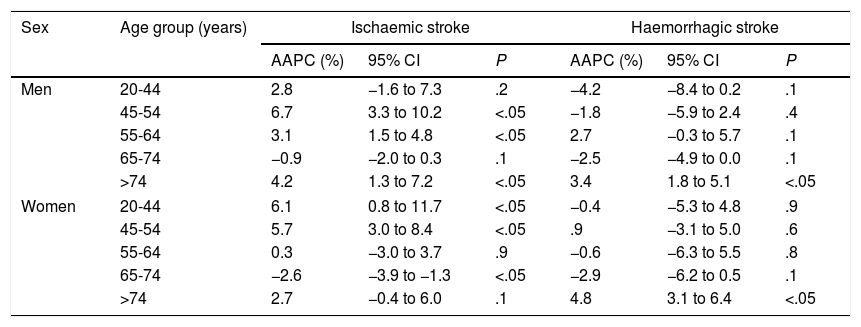
Joinpoint regression confirmed a significant increase in rates of hospitalisation for ischaemic stroke in patients younger than 55 years old, both in men and in women: +6.7% (95% CI, 3.3-10.2) in men aged 45 to 54, and +6.1% (95% CI, 0.8-11.7) in women aged 20 to 44 and +5.7% (95% CI, 3.0-8.4) in women aged 45 to 54. We also observed a significant increase in the rate of hospitalisation for ischaemic stroke in men older than 74, with an AAPC of +4.2% (95% CI, 1.3-7.2). The AAPC for TIA is similar to that of ischaemic stroke: +4.6% (95% CI, 0.9-8.4) in men aged 45 to 54, and +13.3% (95% CI, 6.7-20.4) in women aged 20 to 44 and +5.6% (95% CI, 0.4-11.2) in women aged 45 to 54. The rate of hospitalisation for ischaemic stroke also increased significantly in both men and women older than 74, with an AAPC of +5.4% and +8.6%, respectively. Trend analysis for haemorrhagic stroke confirms that hospitalisation rates stabilised in younger patients; we even observed a decrease among patients younger than 55 years old, although these differences were not statistically significant. A decrease was observed over the study period in rates of hospitalisation for acute but ill-defined cerebrovascular disease in men of all ages and in women aged 20 to 44 and in those older than 64. Table 3 shows trends in hospitalisation rates for each condition from 2002 to 2014, according to the joinpoint regression analysis.
Trends in rates of hospitalisation for each of the diagnoses in Extremadura for the period 2002-2014, broken down by sex. Joinpoint regression.
| Sex | Age group (years) | Ischaemic stroke | Haemorrhagic stroke | ||||
|---|---|---|---|---|---|---|---|
| AAPC (%) | 95% CI | P | AAPC (%) | 95% CI | P | ||
| Men | 20-44 | 2.8 | −1.6 to 7.3 | .2 | −4.2 | −8.4 to 0.2 | .1 |
| 45-54 | 6.7 | 3.3 to 10.2 | <.05 | −1.8 | −5.9 to 2.4 | .4 | |
| 55-64 | 3.1 | 1.5 to 4.8 | <.05 | 2.7 | −0.3 to 5.7 | .1 | |
| 65-74 | −0.9 | −2.0 to 0.3 | .1 | −2.5 | −4.9 to 0.0 | .1 | |
| >74 | 4.2 | 1.3 to 7.2 | <.05 | 3.4 | 1.8 to 5.1 | <.05 | |
| Women | 20-44 | 6.1 | 0.8 to 11.7 | <.05 | −0.4 | −5.3 to 4.8 | .9 |
| 45-54 | 5.7 | 3.0 to 8.4 | <.05 | .9 | −3.1 to 5.0 | .6 | |
| 55-64 | 0.3 | −3.0 to 3.7 | .9 | −0.6 | −6.3 to 5.5 | .8 | |
| 65-74 | −2.6 | −3.9 to −1.3 | <.05 | −2.9 | −6.2 to 0.5 | .1 | |
| >74 | 2.7 | −0.4 to 6.0 | .1 | 4.8 | 3.1 to 6.4 | <.05 | |
| Acute but ill-defined CVD | TIA | ||||||
|---|---|---|---|---|---|---|---|
| Men | 20-44 | −6.6 | −12.1 to −0.8 | <.05 | 6.4 | −1.2 to 14.6 | .1 |
| 45-54 | −1.9 | −6.3 to 2.8 | .4 | 4.6 | 0.9 to 8.4 | <.05 | |
| 55-64 | −0.9 | −7.6 to 6.2 | .8 | 4.7 | 1.3 to 8.2 | <.05 | |
| 65-74 | −9.9 | −14.4 to −5.1 | <.05 | −1.1 | −3.1 to 0.9 | .3 | |
| >74 | −9.4 | −13.3 to −5.4 | <.05 | 5.4 | 3.6 to 7.3 | <.05 | |
| Women | 20-44 | −2.1 | −8.9 to 5.1 | .5 | 13.3 | 6.7 to 20.4 | <.05 |
| 45-54 | 0.4 | −5.3 to 6.4 | .9 | 5.6 | 0.4 to 11.2 | <.05 | |
| 55-64 | 1.1 | −4.9 to 7.5 | .7 | 1.9 | −1.4 to 5.4 | .2 | |
| 65-74 | −5.2 | −7.9 to −2.5 | <.05 | −1.0 | −1.0 to −4.2 | .5 | |
| >74 | −8.2 | −11.8 to 4.6 | <.05 | 8.6 | 6.1 to 11.2 | <.05 | |
95% CI: 95% confidence interval; AAPC: average annual percentage change; CVD: cerebrovascular disease; TIA: transient ischaemic attack.
Our retrospective, observational study conducted in the region of Extremadura included over 39000 cerebrovascular events. Hospitalisation rates for ischaemic stroke and TIA have increased in the past 13 years (2002-2014), whereas the hospitalisation rate for haemorrhagic stroke has stabilised and that for acute but ill-defined cerebrovascular disease has decreased significantly in the groups studied. In Spain, the incidence of cerebrovascular disease has been evaluated in several studies showing considerable methodological differences.7 Incidence rates range from 120 to 350 cases per 100000 person-years.11,12 Our results stand in contrast with the decrease in the incidence of cerebrovascular disease described in recent decades in Spain7 and in other countries,13,14 and which seems to be linked to the measures adopted for controlling risk factors. In the United Kingdom, for example, the incidence of stroke decreased by 29% between 1999 and 2008, coinciding with a marked increase in the prescription of primary and secondary prevention measures for vascular diseases in primary care.15 However, our data are consistent with those of a recent study including over 400000 patients, which describes the trends in the incidence of stroke in a similar period: after adjusting for confounding variables, the incidence of stroke was found to increase 2% or 3% per year from 2003 to 2013 in patients with and without diabetes, respectively.10
The purpose of our study was to evaluate changes in hospitalisation rate trends by sex, age, and diagnosis, as healthcare professionals believe that the number of young patients hospitalised due to stroke is increasing. According to our results, the rate of hospitalisation for ischaemic stroke during the study period increased until 2010 and then stabilised, behaving similarly in men and women. The hospitalisation rate for haemorrhagic stroke (including subarachnoid haemorrhage) was stable during the study period, with no significant differences between sexes. One of the most striking findings of the study is the fact that rates of hospitalisation for TIA increased progressively in both men and women; this may be due to increased awareness and understanding of the condition among the general population. The number of people seeking medical care when TIA is suspected is increasing,12 although no specialised outpatient resources are available for quick management of these cases. Hospitalisation rates for acute but ill-defined cerebrovascular disease follow a pronounced downward trend, which may indicate better access to neuroimaging and aetiology studies, improving classification and diagnostic coding.
By age group, hospitalisation rates for ischaemic stroke and TIA show a significant, progressive increase in men aged 45 to 64, and in women aged 20 to 54. The percentage of patients younger than 65 who had ischaemic stroke at the beginning of the study period was 14.3%, increasing to 19.1% by the end of the study. This change in the epidemiology of ischaemic stroke has also been observed in other European countries and in the United States.5,15–17 A study conducted in the Netherlands reported a 20% increase in the incidence of ischaemic stroke in men and a 33% increase in women aged 35 to 64 between 1997 and 2005, and no changes in people older than 65.17 Another recent study conducted in Sweden, covering the period between 1987 and 2010, found a marked decrease in the incidence of ischaemic stroke from the mid 1990s in individuals aged 65 to 84 years old, a decrease in incidence among middle-aged individuals (45-64 years), and a constant increase among individuals aged 18 to 44 years old (approximately 1.5% during the study period).18 This increase in the incidence of stroke is explained mainly by an increase in the incidence of ischaemic stroke, whereas the incidence of haemorrhagic stroke remained stable16; this was also true in our series. The greater incidence of stroke at younger ages has also been observed in the United States. In a population study into incidence trends for cerebrovascular disease in a population of over 1.3 million people, the mean age of patients with a first-ever stroke decreased from 71 years for the period 1993-1994 to 69 years in 2005. Likewise, the percentage of cerebrovascular events occurring in patients aged 20 to 54 years old increased from 13% to 19% for the same time periods.5
One of the highest-quality epidemiological studies in the literature, which was conducted in Spain and published in 2012,8 estimated the incidence of cerebrovascular disease at 202.5 new cases per 100000 men and 172.6 new cases per 100000 women; 21.1% of patients were younger than 65 and incidence peaked at ages older than 84 years. Incidence rates throughout Spain are not homogeneous: the rates observed in southern and north-western Spain are much higher than those reported for the central region and the areas located along the Mediterranean coast. The incidence rates of stroke in Extremadura, in south-western Spain, are higher than the Spanish average.19 This, combined with the region's ageing population (in both rural and urban settings20), may contribute to the increasing hospitalisation rates observed in individuals older than 74, except for acute but ill-defined cerebrovascular disease, as mentioned previously.
There has been a clear shift in the incidence of TIA and ischaemic stroke, affecting younger individuals. The reasons for this alarming change are not precisely known and cannot be inferred from the results of this or similar studies.5,15–18 There is increased understanding and awareness of cerebrovascular disease among the general population as well as healthcare professionals,21 thanks to specific strategies such as code stroke and awareness campaigns; this may have led people to seek medical care for less severe events. Diagnostic techniques and access to neuroimaging tests have also improved, especially in the case of MRI, whose use for ischaemic stroke has become considerably more widespread in the past 15 years.22 MRI is far superior to CT for diagnosing stroke, as it detects subtle ischaemic changes, determines the location of ischaemia, and helps determine aetiology in some cases.23 However, these factors do not fully explain the problem.
Another more likely explanation involves a demographic change in stroke risk factors, the increased incidence of obesity in children and young adults, poor eating habits, and sedentary lifestyles; these factors may result in premature cerebrovascular disease.6 A population-based study into the prevalence of vascular risk factors in Extremadura reported higher incidence of diabetes and obesity than most studies conducted in Spain (in Extremadura, obesity is more prevalent among men), and revealed that tobacco use is still one of the most prevalent risk factors despite restrictions. However, prevalence of arterial hypertension and hypercholesterolaemia in Extremadura is in line with estimations for Spain.24 Perceived psychosocial stress is another factor receiving little attention but which may play a prominent role in the pathophysiology of stroke in younger patients.25 Psychosocial stress has been strongly associated with coronary artery disease.26 Although the association with cerebrovascular disease is less clear, stress is commonly perceived to be a risk factor for stroke.21,27 Some studies have identified an association between perceived psychosocial stress and cerebrovascular disease28; further high-quality, well designed studies with sufficient follow-up periods are needed to determine the strength of this association.
LimitationsSome of this study's strengths include its large sample size, the length of the study period (13 years), and the standardised methodology, which has previously been used in other studies.7,9,10,18 However, our study also has a number of limitations. Data were drawn from the MBDS; this database contains data about administrative discharges of patients hospitalised in our autonomous community and uses the information disclosed by the physician in the discharge report; the data are therefore subject to a selection bias. As data were anonymised, we were unable to distinguish between first-ever events and recurrent events. Therefore, our results cannot be strictly compared to those from population studies about the incidence of cerebrovascular disease; in any case, this was not one of the aims of the study. Our data may also include readmissions; we attempted to prevent this by including only the main diagnosis. Previous studies using the MBDS have shown that readmissions account for less than 10% of hospitalisations due to stroke29 and would therefore have only a limited impact on our results.
ConclusionsStroke has traditionally been considered a disease of the elderly. This study aimed to analyse, at least indirectly, the changes observed in the demography of stroke. The evidence suggests an epidemiological change in ischaemic stroke: the hospitalisation rate among young adults has increased. The greater incidence of stroke at younger ages has a great impact on the global burden of the disease due to the lost productivity and increasing health expenses over time; preventive measures should be taken to revert this alarming trend. Governmental support is necessary to develop strategies and campaigns targeting the younger population and to promote healthy lifestyle and eating habits.
FundingThis study was made possible by a research grant awarded by the Health Service of Extremadura.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank Rubén David Arranz from the Health Service of Extremadura's Information Systems Service for his valuable contribution. We also wish to thank the General Directorate for Healthcare Planning, Training, and Quality of the regional government of Extremadura for their commitment to the project.
Please cite this article as: Ramírez-Moreno JM, Felix-Redondo FJ, Fernández-Bergés D, Lozano-Mera L. Tendencias en las tasas de hospitalización por ictus en Extremadura en el periodo 2002–2014. Cambiando la idea del ictus como una enfermedad propia de la senectud. Neurología. 2018;33:561–569.
