



Piloerection which is considered predominantly vestigial in humans, has its basis in the autonomic circuits of the brains. It can herald a disorder especially form the temporal lobe. We describe three cases with distinct etiologies to highlight the same.
Cases reportsCase 1: A 52-year man presented with recurrent episodes of piloerection accompanied by autonomic symptoms and was diagnosed to have temporal lobe glioma. Case 2: A 36-year woman presented with recurrent episode of pioerection accompanied by chills and was found to have temporal lobe cyst with contralateral oedema. Case 3: A 61-year man developed unilateral piloerection and chills and was found to have Lgi1 encephalitis.
ConclusionThis case series highlights the significance of ictal piloerection, the diverse etiologies, its localization to temporal lobe structures, its association with the limbic system, and the unique ipsilateral lateralization seen with this semiology.
La piloerección, que se considera predominantemente vestigial en humanos, tiene su base en los circuitos autónomos del cerebro. Puede anunciar un trastorno especialmente del lóbulo temporal. Describimos tres casos con etiologías distintas para resaltar el mismo.
CasosCaso 1: un hombre de 52 años presentó episodios recurrentes de piloerección acompañados de síntomas autonómicos y se le diagnosticó glioma del lóbulo temporal. Caso 2: una mujer de 36 años presentó un episodio recurrente de piloerección, acompañado de escalofríos y se encontró que tenía un quiste en el lóbulo temporal con edema contralateral. Caso 3: un hombre de 61 años desarrolló piloerección unilateral y escalofríos y se encontró que tenía encefalitis Lgi1.
ConclusiónEsta serie de casos destaca la importancia de la piloerección ictal, las diversas etiologías, su localización en las estructuras del lóbulo temporal, su asociación con el sistema límbico y la lateralización ipsilateral única observada con esta semiología.
Piloerection or goosebumps refers to the autonomic phenomenon when the hair stands on its end. It has predominant functionality in animals, increasing the amount of insulation when exposed to cold, or by making the form appear larger when facing a threat.1 But it is considered vestigial in humans, having evolutionally lost its original functions, except when being fictionally referred in a certain Peter Parker about to face danger, referred notoriously as the spidey sense. Scientifically piloerection has its basis in the autonomic circuits of the brain and can herald a neurological disorder.2 We describe a series of three patients with etiologically different lesions in the temporal lobe presenting with pilomotor seizures as the predominant issue.
Case vignetteCase 1A 52-year male, with no prior comorbidities, developed a left-sided headache, dull aching with moderate severity, intermittent, twenty days before presentation, with no associated nausea, visual changes or specific aggravating factors. Ten days later the patient developed episodic piloerection over both upper limbs, with associated giddiness, palpitations and sweating lasting for 30s. The episodes occurred 20–30 times per day, with more alleged clustering around 1100 am. No loss of awareness, posturing or clonic movements. Neurological examination was normal. Gadolinium-enhanced MRI brain revealed irregular heterogeneously enhancing intra-axial lesion with areas of necrosis and haemorrhage in the anterior temporal lobe with surrounding oedema, elevated choline creatinine ratio, and increased perfusion, f/s/o suggestive of high-grade glioma (Fig. 1A). He was advised EEG, initiated on AEDs and he was referred for a neurosurgical consult.
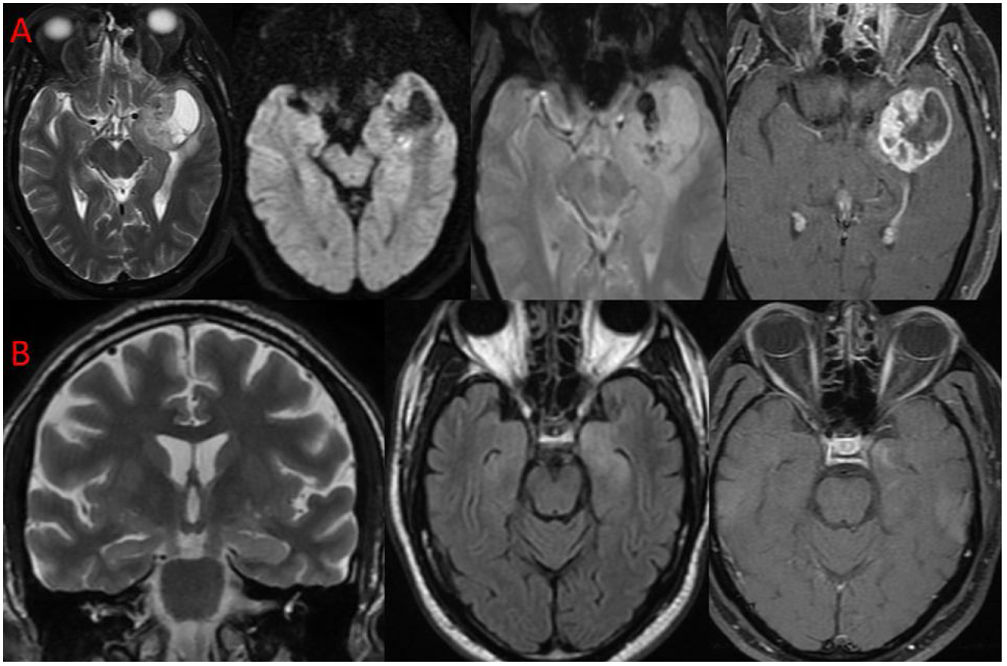
 T2 axial, DWI, GRE, T1FS post contrast. Solid-cystic mass lesion in left anterior temporal lobe with peripheral thick nodular enhancement and central necrotic area. Solid component of lesion showing few foci of haemorrhage within. Left mesial temporal lobe structures are infiltrated. (B) T2 oblique coronal, T2 FLAIR axial, T1FS post contrast. T2-FLAIR hyperintensity involving the bilateral mesial temporal lobes (L>R) with subtle enhancement in left amygdala and hippocampal head.")
(A) T2 axial, DWI, GRE, T1FS post contrast. Solid-cystic mass lesion in left anterior temporal lobe with peripheral thick nodular enhancement and central necrotic area. Solid component of lesion showing few foci of haemorrhage within. Left mesial temporal lobe structures are infiltrated. (B) T2 oblique coronal, T2 FLAIR axial, T1FS post contrast. T2-FLAIR hyperintensity involving the bilateral mesial temporal lobes (L>R) with subtle enhancement in left amygdala and hippocampal head.
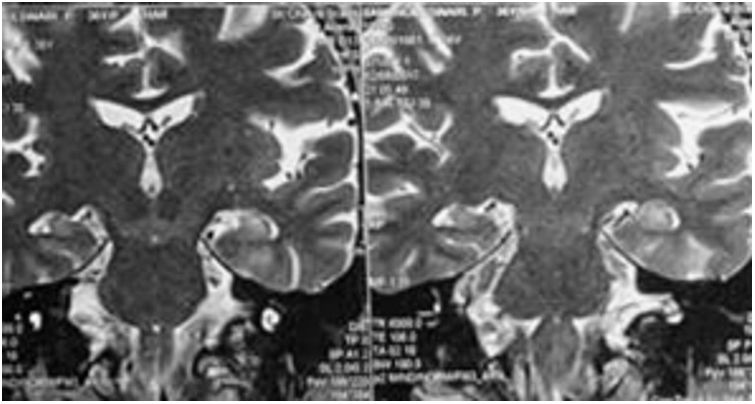
A 36-year female, diabetic developed sudden episodic piloerection over the left upper limb, associated with a shock-like chilly sensation rising from her fingertip to the ipsilateral face region, followed by an inability to respond for 2–3s. These episodes were not associated with falls, tonic posturing or clonic movements. The number of episodes increased from once a week to 2–3 times per week. Her neurological evaluation was otherwise unremarkable. MRI brain revealed cystic foci in the right hippocampal body, with left hippocampal T2/FLAIR hyperintensity, with no evidence of hippocampal atrophy (Fig. 2). EEG repeated twice was normal, despite studying for 1h. Her episodes reduced when she was initiated on AEDs (levetiracetam and oxcarbazepine) and is on follow-up.
Case 3
A 61-year male, hypertensive and diabetic, presented with recurrent episodes of piloerection, which started with a sense of unease, followed by piloerection, predominantly seen over the left upper limb, accompanied by a sense of chilly paresthesia over the entire body. In some instances he noted that the chills were prominent, followed by piloerection. The episodes were initially two or three times a day, progressing to around 10–20 times per day. His neurological examination during and between the episodes was otherwise unremarkable. Gadolinium-enhanced MRI brain showed T2/FLAIR hyperintensities in bilateral medial temporal lobes (left>right) with a mild enhancement of the left medial temporal lobe noted (Fig. 1B). EEG was normal and the patient was started on anti-epileptics and anti-viral drugs. CSF AE encephalitis panel sent was positive for LGi1 encephalitis. Following high dose pulse steroid therapy, the patient's seizures remitted. He is presently on AEDs, and is on follow-up for the last two years.
DiscussionPiloerection occurs due to contraction of the Arrector pili muscles in response to a sympathetic stimulus or as a thermoregulatory response.3 But not all sympathetic stimuli elicit piloerection, leading to several hypotheses including the “peak arousal hypothesis” which states that stimuli causing a higher physiological or emotional arousal are more likely to cause it, and the more evolutionary “separation call hypothesis” which emphasises more on fear.4 Physiologically thermoregulatory response to cold starts with cutaneous vasoconstriction, behavioural changes then shivering and is chiefly mediated by the anterior hypothalamus. This region receives rich afferents from the limbic system and the temporal cortex, especially the hippocampus.5 So an epileptic focus close to the limbic structures or the temporal lobe can eventually elicit the thermoregulatory response, which starts with the vasoconstriction response, mediated by the sympathetic system, also presumably contracting the arrector pili muscles causing piloerection. Stimulation of the insula, hippocampus, amygdala, midbrain and neocortical areas in the temporal and parietal lobe have elicited piloerection, but the review of the literature reveals the temporal lobe as the most commonly encountered site.6
Very often the piloerection reaction is associated with a subjective experience of chills, described as chills down the spine, observed in two of the above patients. The localization of these chills is also debated to be the subjective sensory interpretation of the piloerection per se. Studies using high-density EEG to study patients with musical chills identified greater activities in the insula, prefrontal cortex (ventro-medial pre-frontal cortex, orbitofrontal cortex) and supplementary motor area, which correspond to the previously established neuroimaging findings as well.7 High-density EEGs produce recordings by using a higher spatial sampling of scalp electrodes when compared with the standard EEG, demonstrating improved localization of epileptogenic foci. Moreover, increased EEG activity was noted over the superior temporal gyrus, which is relevant for musical like/dislike tendencies and has connections with the orbitofrontal cortex.7 But whether the chills lead to piloerection or both are independent phenomenon is unclear. A review of literature where the semiology is documented in details shows, that they have predominantly been described without much differentiating into which came first except in the study by Stefan et al., 5 where he describes eight cases where the sensation of chills preceded the piloerection similar to some of our cases. This also fits in with the temporal origin of the phenomenon before the epileptic activity spreads to the autonomic network.
Various etiologies have been associated with pilomotor seizures including tumours most commonly glioblastoma, trauma, mesial temporal sclerosis, infections especially viral encephalitis, and antibody-mediated encephalitis with the encountered antibody being anti-LGi1. Vascular causes like strokes were not as frequently associated with this semiology.8 Ipsilateral lateralizing value of piloerection when present unilaterally has been described in the literature,9 especially in males10 which were observed in one of our cases with the other two being either bilateral presentation or having lesions on both sides.9 These seizures are refractory to antiepileptic therapy, with a systematic review describing nearly 68% refractoriness, and AEDs have to be individualized.10 The patients in the above cases had normal EEGs. Interictal EEGs may be normal in up to 50% of the patients with epilepsy, with their yield accentuated by sleep deprivation, increasing the duration of EEG and using activation procedures. Moreover, patients with deep-seated epileptogenic foci can have normal routine EEGs.
In conclusion, we report a series of three cases with focal non-motor onset autonomic seizures with preserved awareness, with localization of lesion to the temporal lobe and its connections This case series, highlights the significance of ictal piloerection, the diverse etiologies, its localization to temporal lobe structures, its association with the limbic system, and the unique ipsilateral lateralization seen with this semiology.
Ethical approvalNot obtained as it was a case report[s].
FundingNone declared.
Competing interestsNone declared.
Authors’ contributionsDr Rithvik Ramesh – conception and design, data acquisition, interpretation, drafting and revision.
Dr Philo hazeena – drafting and revising it for critical intellectual content.
Dr Shankar – final approval.
Dr Harsha Vardhan – Data ACQUISITION, final approval.
