



Camptocormia is characterized by an abnormal posture of the trunk with marked forward flexion of the thoracolumbar spine, which accentuates during standing and walking and abates in the recumbent position.
Material/methodsCase report.
ResultsWe describe a 62-year-old woman with L1 vertebral body collapse and partial compression of the cauda equine underwent surgery decompression and stabilization with instrumentation technique. She was discharged 5 days later with ambulation preserved but with camptocormia. Electromyography of lumbar and lower thoracic paraspinal muscles showed denervation.
DiscussionA pathophysiological mechanism triggered by surgery with instrumentation technique resulted in denervation and atrophy of paraspinal muscles.
La camptocormia es una postura anormal del tronco caracterizada por flexión de la columna tóraco-lumbar que se acentúa durante la marcha y desaparece durante el decúbito.
Material y métodoCaso clínico.
ResultadoPaciente de 62 años de edad que presentó colapso de L1 secundario a metástasis por lo que requirió cirugía descompresiva y estabilización con técnica de instrumentación. Egresó a los 5 días con deambulación conservada, pero con camptocormia.
DiscusiónEn este caso se podría postular como mecanismo fisiopatológico desencadenante la cirugía con técnica de instrumentación lumbar, y la alteración y el reemplazo graso secundario de los músculos paravertebrales.
Camptocormia comes from the Greek kamptos (stoop/bend) and kormos (trunk) and is characterized by an abnormal posture of the trunk with marked forward flexion of the thoracolumbar spine, which accentuates during standing and walking and abates in the recumbent position.1 First described by Brodie in 1818 and designated by Souques and Rosanoff-Saloff in 1915,2 camptocormia may be observed in various neurological conditions including Parkinson's disease (PD), dystonia, myopathy, and cerebrovascular, idiopathic and psychogenic disease.1 We report the case of a patient with camptocormia secondary to a neuro-oncologic lumbar spine surgery with instrumentation technique.
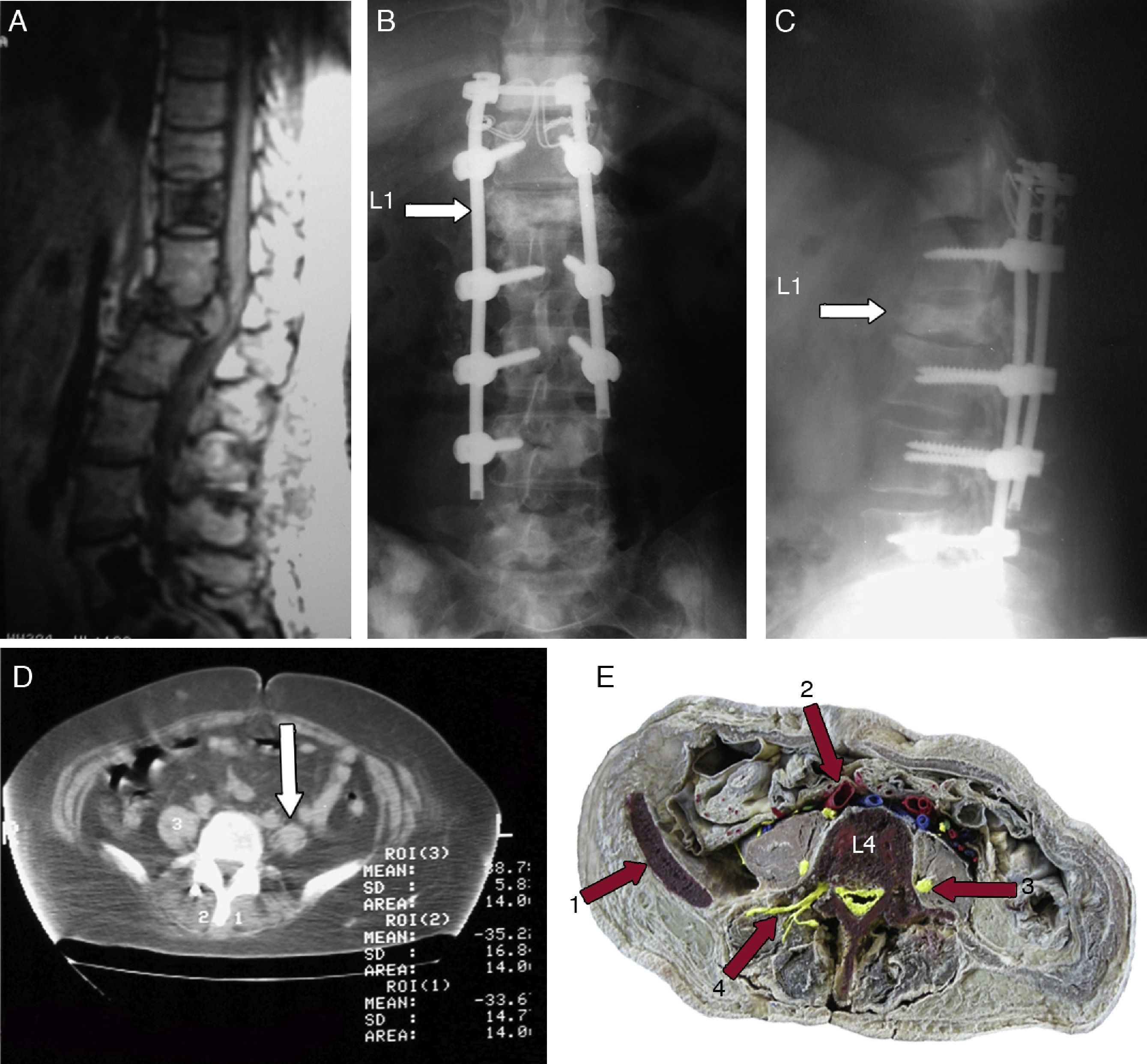
Case reportA 62-year-old woman was diagnosed with breast cancer in February 2006 and began chemotherapy with adriamycin 75mg/m2 and docetaxel 50mg/m2 every 21 days. Due to febrile neutropenia she received only a single dose and then continued with tamoxifen 20mg/day. In February 2008 she complained of severe low back pain. A bone scan showed increased uptake in the spine from D7 to D11. Magnetic resonance imaging (MRI) showed multiple metastasis on vertebral bodies with L1 body collapsed with partial compression of the conus medullaris and cauda equine (Fig. 1A). In October 2008 the patient underwent surgery decompression and stabilization with pedicle screws and paraspinal rods from D11 through L4 and arthrodesis with autologous bone graft (Fig. 1B and C). The patient was discharged 5 days later with ambulation preserved but with a marked forward flexion posture of her trunk during standing and gait that disappeared when she lied down. Postoperative serum creatine phosphokinase (CPK) levels were not studied. A K-Taylor brace was indicated by an orthopedic surgeon. Due to persistence of the severe abnormal posture, in April 2009 the patient was referred to our department of neurology. She presented with marked forward flexion posture of her trunk during standing and gait which disappeared when lying down on the exam table. Her standing and ambulation were aided with a cane. There was no family history for neurological or muscular diseases. Physical examination showed only camptocormia and residual 4/5 paresis of right inferior limb. C-reactive protein, ESR and CPK were normal. Electromyography of lumbar and lower thoracic paraspinal muscles (erector spinae musculus) demonstrated denervation. A lumbar spine CT showed a diminished density of paraspinal muscles with fatty replacement (−35.2HU, controls+50HU), matched with psoas muscle density (+38.7HU) (Fig. 1D).
 MRI (sagittal T1-weighted image). Metastatic lesions in vertebrae D11, L5 and S1. L1 vertebral body collapse and conus medullaris/cauda equina compression. (B and C) Post-surgical AP and lateral plain radiograph of the lumbar spine. Note instrumentation technique. (D) Axial computed tomography image without contrast. Note the lower density of paraspinal muscles (−35.2HU and −33.6HU), and left psoas muscle markedly hypotrophic (arrow). (E) Anatomical correlation at similar CT level (1) Crista iliaca, (2) Arteria iliaca comunis, (3) Nervus femoralis, (4) Nervi dorsal rami.")
Imaging studies and anatomical correlation. (A) MRI (sagittal T1-weighted image). Metastatic lesions in vertebrae D11, L5 and S1. L1 vertebral body collapse and conus medullaris/cauda equina compression. (B and C) Post-surgical AP and lateral plain radiograph of the lumbar spine. Note instrumentation technique. (D) Axial computed tomography image without contrast. Note the lower density of paraspinal muscles (−35.2HU and −33.6HU), and left psoas muscle markedly hypotrophic (arrow). (E) Anatomical correlation at similar CT level (1) Crista iliaca, (2) Arteria iliaca comunis, (3) Nervus femoralis, (4) Nervi dorsal rami.
Camptocormia is a recognized feature of PD. Tiple et al. observed a 6.9% prevalence, found in patients with more severe PD as clinically assessed by Hoehn-Yahr staging and the UPDRS motor score.3,4 Some authors postulate onset of camptocormia secondary to lesions in the lenticular nucleus.5 Camptocormia and lumbar surgery for herniated discs have been reported once.1 In our case, camptocormia was secondary to neuro-oncologic lumbar surgery without other associated diseases. The role of peripheral trauma and movement disorders is not clear, although there are some clinical criteria that could establish a relationship between them: severity of trauma, time interval between trauma and onset of symptoms (< 1 year), and anatomical relationship between both.6 The lumbar instrumentation technique has shown some side effects that affect paravertebral muscles, such as atrophy and fatty replacement. This could be explained by the denervation of the paraspinal muscles, as shown by Tsutsumimoto et al. who compared the conventional surgical technique with other small incisions.7 It should be kept in mind that fibers of the dorsal rami are the only ones that supply the paraspinal muscles, which themselves lack intersegmental innervations (Fig. 1E). In spine surgery, muscle injury can be inflicted by the large midline incision, by disruption of muscle fibers through dissection, by intraoperative bleeding, and by forceful abduction through the use of retractors in achieving proper lateral–medial screw trajectory, as evidenced by the higher levels of CPK during the first postoperative week. Advances in mini-open methods have been designed to reduce the length of the incision. Likewise, blunt dissection using the fingers and the use of expandable tubular retractors provided a lower intraoperative muscle and neuropathic injury.7
We postulate a pathophysiological mechanism triggered by surgery with instrumentation technique: (a) vessel section and hemorrhage; (b) section of the lumbar nerves dorsal rami for the erector spinae musculus; (c) compression and ischaemia as a consequence of the retractors.
Alone or combined, these resulted in denervation and atrophy of paraspinal muscles in our patient. To our knowledge, this is the first time this association has been shown.
Ethical standardsThe authors confirm that the patient involved in this case report gave her informed consent prior to her inclusion in this study.
Conflict of interestThe authors have no conflict of interest to declare.
