





Communication and language skills are among the most severely affected domains in individuals with autistic spectrum disorder (ASD). When a child diagnosed with ASD lives in a bilingual environment, the parents often express concerns about whether their child should learn both languages simultaneously, turning to specialists for advice. Despite the lack of evidence of any negative effect, some professionals disagree on this subject. In this systematic review we study whether bilingualism affects language development in children with ASD.
MethodsWe reviewed the literature published in 4 different databases. After applying a series of selection criteria, we selected 12 scientific articles, including a total of 328 children diagnosed with ASD (169 bilingual and 159 monolingual), with ages ranging from 3 to 12 years. These patients were evaluated with different receptive and expressive language assessment instruments covering several areas. The assessments were performed directly on the children, although indirect assessment of parents was also performed in some studies.
ConclusionsThere seems to be consensus regarding the assertion that bilingualism does not entail any additional difficulty for language development in children with ASD from the age of 3.
La comunicación y el lenguaje de las personas con trastorno del espectro autista (TEA) son algunos de los aspectos que más frecuentemente se ven alterados en este trastorno del neurodesarrollo. Cuando un niño que recibe el diagnóstico de TEA vive en un entorno bilingüe, los padres con frecuencia manifiestan su preocupación sobre si sus hijos deberían aprender dos idiomas simultáneamente y acuden a especialistas para ser aconsejados al respecto. A pesar de que no exista evidencia de sus efectos negativos, algunos profesionales se han mostrado en desacuerdo. Este trabajo pretende conocer si el bilingüismo afecta al lenguaje de niños con TEA.
DesarrolloSe ha realizado una revisión de la literatura científica publicada en cuatro bases de datos y siguiendo una serie de criterios se han seleccionado 12 artículos publicados en revistas científicas. Participaron 328 niños diagnosticados con TEA (169 bilingües y 159 monolingües) con edades entre los 3 y 12 años, evaluados con diferentes pruebas de lenguaje receptivo y expresivo que abarcan áreas diversas. La evaluación se realizó de modo directo a los niños, aunque también se evaluaron indirectamente a los padres en algunos trabajos.
ConclusionesSe ha comprobado en esta revisión que existe acuerdo sobre que el bilingüismo no supone ninguna dificultad adicional para el desarrollo del lenguaje de niños con TEA a partir de los 3 años.
Bilingualism is a very frequent condition, with more than half of the world’s population speaking more than one language.1 As in monolingual children, language development in children who speak more than one language plays an important role in cultural identity, personal and familial well-being, and personal identity.2 For typically developing (TD) bilingual children, earlier acquisition of the second language is associated with greater proficiency. Thus, bilingualism is classified as simultaneous if it occurs from birth and sequential if the second language is acquired after the first 3 years of life.3 Several studies have shown that age at acquisition of the second language has an impact on the child’s skills in both languages. For instance, some researchers have found that simultaneous bilingual people are more competent in the second language than sequential bilingual individuals.4
Many studies have shown than speaking more than one language is associated with academic, social, emotional, and cognitive benefits.5,6 Furthermore, TD bilingual children do not show deficiencies in language and communication skills compared to monolingual children.1,7 However, differences have been reported between bilingual and monolingual children in the first years of life.8 Specifically, some factors influencing language and communication development are age at acquisition of the second language, amount of exposure to that language, and the social context of exposure to that language.4,5,9
Given the trajectory of language development in TD bilingual children, there is much interest in establishing whether these characteristics are also reflected in children with atypical speech and language development. For instance, the parents of children with autistic spectrum disorder (ASD) have expressed doubt over the years as to whether simultaneously exposing their children to 2 languages may be beneficial.10 Whereas the parents of TD children generally take a positive view of second language learning, this is not always the case for children with ASD.11 Parents are often concerned that exposure to 2 languages may lead to problems developing one of them in children with ASD, opting instead to raise their children in a monolingual environment.12 Similar considerations are described regarding education, with bilingual schooling raising the most questions for parents of children with ASD.13
ASD is a neurodevelopmental disorder characterised by difficulties with social interaction and communication, with patients presenting restricted, repetitive patterns of behaviour, interests, and activities.14 It occurs in all ethnicities, independently of socio-economic situation, with an incidence rate of 1 case per 59 children; boys are more frequently affected than girls (male-to-female ratio of 4:1).15
In addition to the social/communication difficulties that are common to all these patients, children with ASD present difficulties with receptive and/or expressive language. A recent meta-analysis found that, globally, children with ASD present expressive and receptive language skills 1.5 standard deviations below the mean for their peers, in different stages of development, in both direct assessment (direct measurement of performance) and indirect assessment (information reported by third parties, such as parents or teachers); however, some patients seem to display better expressive language development.16
The alterations observed in structural and functional components of language vary greatly across patients with ASD. Thus, we may observe a spectrum from children with large vocabularies and preserved structural skills but with impaired pragmatic abilities (a universal feature of ASD) and prosodic variations, to those at the other extreme who are completely unable to speak.17,18
Despite parents’ concerns, the limited available evidence on the effects of bilingualism in children with ASD (ASD-B) does not suggest any negative effects on language,19–21 as they seem to develop diverse skills in both languages at the same level as monolingual children with ASD (ASD-M). However, several factors have been described that do affect the development of the second language, including ASD severity, level of intelligence, and the frequency with which both languages are used.13,19,22,23
Generally, studies analysing language in ASD-B compare these children against ASD-M or TD bilingual children (TD-B) of similar age. The results reported in the various studies on language in ASD-B suggest that they are not disadvantaged with respect to ASD-M.24 Previous literature reviews, such as that conducted by Wang et al.25 of articles published until 2016, including the grey literature, lectures, and theses, compare the cognitive, behavioural, and language performance of children with ASD in bilingual and monolingual settings, finding no evidence of an unfavourable effect of bilingualism on development. ASD-B children are also reported to display advantages in cognition, pragmatic language/communication, and expressive vocabulary.25,26 However, consensus on these conclusions is not universal due to the great heterogeneity of this patient population.25
In the light of all of the above, the evidence in the literature seems to suggest that exposure to a second language has no negative effect on language development in children with ASD. Wang et al.25 showed that language analysis may not be essential in ASD-B; rather, emphasis should be placed on language comprehension, communication, and clinical practice. However, as these authors’ review was limited to articles published until 2016, there may have been advances in recent years. Therefore, this systematic review aims to update, describe, analyse, and synthesise the evidence from the last 5 years on language development in ASD-B.
MethodsSearch strategyThe literature search and drafting of this study observed the recommendations of the PRISMA and MOOSE statements.27,28
The search was conducted on the MEDLINE (via PubMed), PsycINFO, PSICODOC, and Scopus databases. The descriptors considered suitable for subsequent searches were: “language,” bilingual,” “multilingual,” “children,” “autism spectrum disorder,” “Asperger.” The final search strategy, developed for MEDLINE and adapted for each database consulted, combined these search terms with the Boolean operators AND and OR, as follows: ((Autism Spectrum Disorder OR Asperger [Title/Abstract]) AND (Bilingual [Title/Abstract]) OR Multilingual [Title/Abstract]) AND (language [Title/Abstract]) AND children [Title/Abstract])).
Results were filtered by date (from 2015 to September 2020) and language of publication (English and Spanish).
In a second search, we consulted other sources to identify other relevant works that were not identified in the initial search.
Selection strategyHaving identified articles according to the procedure described above, we eliminated duplicates and analysed titles and abstracts to screen articles according to the following inclusion criteria: a) published in scientific journals; b) focusing on bilingual or multilingual children diagnosed with ASD and aged older than 3 years; c) including a comparison group; and d) addressing any area of language.
Analysis strategyArticles were analysed according to the PICOS strategy (population, intervention, comparison, outcomes, study design).
We developed an original recording protocol to codify variables of interest and results. The variables extracted in this process were sample size, sex, age, type of bilingualism, type of assessment, instruments used, area of language evaluated, and main results.
Qualitative and quantitative synthesis of the data focused on language characteristics and how they were affected by the different variables listed above.
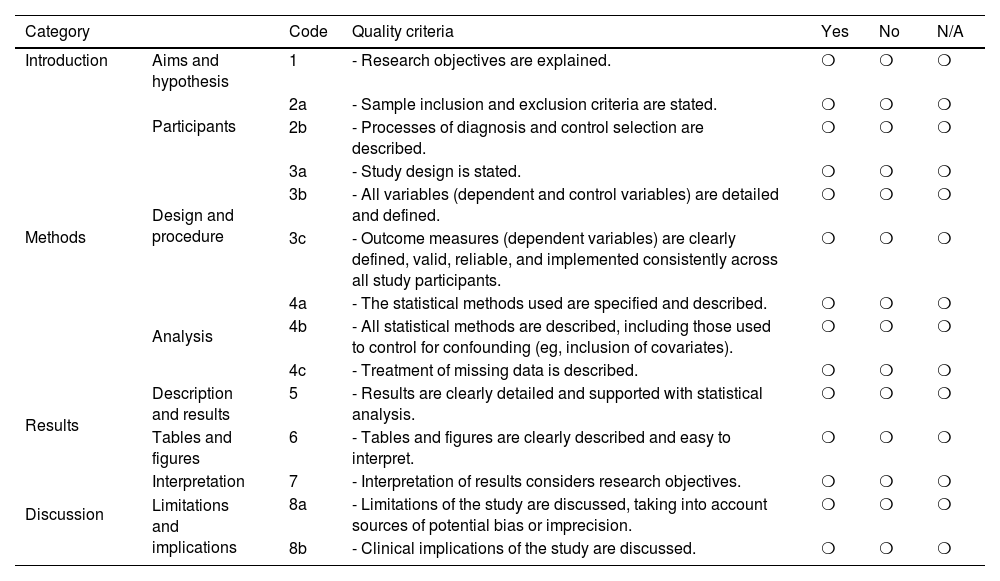
Assessment of methodological qualityMethodological quality of the included studies was evaluated with a scale (Table 1) based on the STROBE statement29 and the scale developed by the National Institute of Health (NIH) for the reporting of observational research.30 Each item was scored 1 or 0, according to whether each study met that criterion.
Characteristics of the studies included in our review article.
| Category | Code | Quality criteria | Yes | No | N/A | |
|---|---|---|---|---|---|---|
| Introduction | Aims and hypothesis | 1 | - Research objectives are explained. | ❍ | ❍ | ❍ |
| Methods | Participants | 2a | - Sample inclusion and exclusion criteria are stated. | ❍ | ❍ | ❍ |
| 2b | - Processes of diagnosis and control selection are described. | ❍ | ❍ | ❍ | ||
| Design and procedure | 3a | - Study design is stated. | ❍ | ❍ | ❍ | |
| 3b | - All variables (dependent and control variables) are detailed and defined. | ❍ | ❍ | ❍ | ||
| 3c | - Outcome measures (dependent variables) are clearly defined, valid, reliable, and implemented consistently across all study participants. | ❍ | ❍ | ❍ | ||
| Analysis | 4a | - The statistical methods used are specified and described. | ❍ | ❍ | ❍ | |
| 4b | - All statistical methods are described, including those used to control for confounding (eg, inclusion of covariates). | ❍ | ❍ | ❍ | ||
| 4c | - Treatment of missing data is described. | ❍ | ❍ | ❍ | ||
| Results | Description and results | 5 | - Results are clearly detailed and supported with statistical analysis. | ❍ | ❍ | ❍ |
| Tables and figures | 6 | - Tables and figures are clearly described and easy to interpret. | ❍ | ❍ | ❍ | |
| Discussion | Interpretation | 7 | - Interpretation of results considers research objectives. | ❍ | ❍ | ❍ |
| Limitations and implications | 8a | - Limitations of the study are discussed, taking into account sources of potential bias or imprecision. | ❍ | ❍ | ❍ | |
| 8b | - Clinical implications of the study are discussed. | ❍ | ❍ | ❍ | ||
The quality of the articles was also analysed using impact metrics from Journal Citation Report (JCR) and Web of Science (WOS).
ResultsStudy characteristicsThe initial search yielded a total of 186 articles (Fig. 1). Of these, we eliminated 82 duplicate results; 2 additional articles were identified from the references sections of the studies identified.

In the screening phase, after reading titles and abstracts we eliminated articles unrelated to bilingualism, ASD, or children, and systematic reviews, resulting in a total of 43 articles. In the selection phase, we read the full texts of articles, eliminating 31 that did not focus on language or included patients younger than 3 years.
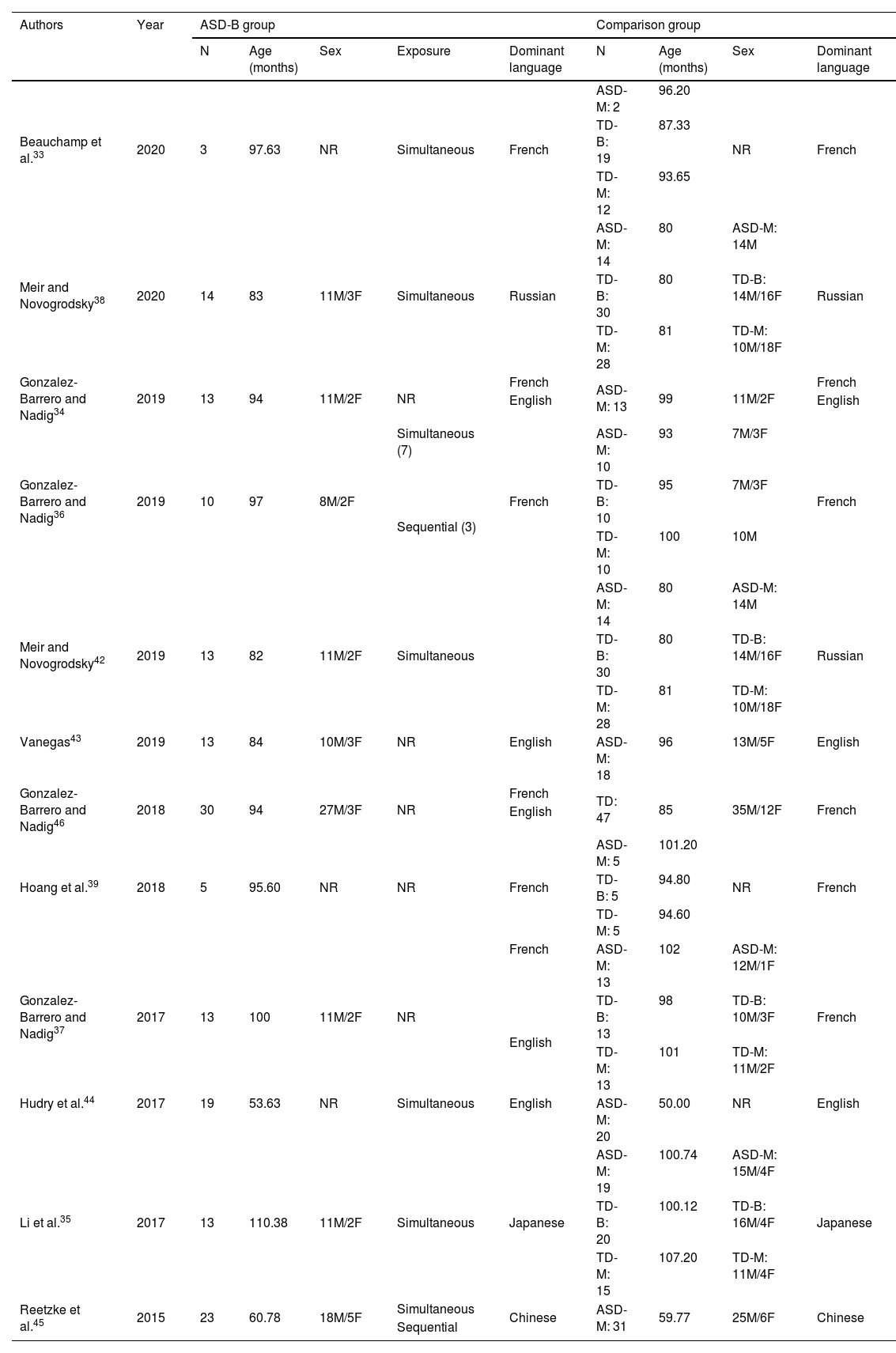
Therefore, a total of 12 studies were included for review (Tables 2 and 3), all of which addressed language in children with ASD older than 3 years, raised in a bilingual environment, and included comparison groups.
Characteristics of the studies included.
| Authors | Year | ASD-B group | Comparison group | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Age (months) | Sex | Exposure | Dominant language | N | Age (months) | Sex | Dominant language | ||
| Beauchamp et al.33 | 2020 | 3 | 97.63 | NR | Simultaneous | French | ASD-M: 2 | 96.20 | NR | French |
| TD-B: 19 | 87.33 | |||||||||
| TD-M: 12 | 93.65 | |||||||||
| Meir and Novogrodsky38 | 2020 | 14 | 83 | 11M/3F | Simultaneous | Russian | ASD-M: 14 | 80 | ASD-M: 14M | Russian |
| TD-B: 30 | 80 | TD-B: 14M/16F | ||||||||
| TD-M: 28 | 81 | TD-M: 10M/18F | ||||||||
| Gonzalez-Barrero and Nadig34 | 2019 | 13 | 94 | 11M/2F | NR | French | ASD-M: 13 | 99 | 11M/2F | French |
| English | English | |||||||||
| Gonzalez-Barrero and Nadig36 | 2019 | 10 | 97 | 8M/2F | Simultaneous (7) | French | ASD-M: 10 | 93 | 7M/3F | French |
| Sequential (3) | TD-B: 10 | 95 | 7M/3F | |||||||
| TD-M: 10 | 100 | 10M | ||||||||
| Meir and Novogrodsky42 | 2019 | 13 | 82 | 11M/2F | Simultaneous | ASD-M: 14 | 80 | ASD-M: 14M | Russian | |
| TD-B: 30 | 80 | TD-B: 14M/16F | ||||||||
| TD-M: 28 | 81 | TD-M: 10M/18F | ||||||||
| Vanegas43 | 2019 | 13 | 84 | 10M/3F | NR | English | ASD-M: 18 | 96 | 13M/5F | English |
| Gonzalez-Barrero and Nadig46 | 2018 | 30 | 94 | 27M/3F | NR | French | TD: 47 | 85 | 35M/12F | French |
| English | ||||||||||
| Hoang et al.39 | 2018 | 5 | 95.60 | NR | NR | French | ASD-M: 5 | 101.20 | NR | French |
| TD-B: 5 | 94.80 | |||||||||
| TD-M: 5 | 94.60 | |||||||||
| Gonzalez-Barrero and Nadig37 | 2017 | 13 | 100 | 11M/2F | NR | French | ASD-M: 13 | 102 | ASD-M: 12M/1F | French |
| English | TD-B: 13 | 98 | TD-B: 10M/3F | |||||||
| TD-M: 13 | 101 | TD-M: 11M/2F | ||||||||
| Hudry et al.44 | 2017 | 19 | 53.63 | NR | Simultaneous | English | ASD-M: 20 | 50.00 | NR | English |
| Li et al.35 | 2017 | 13 | 110.38 | 11M/2F | Simultaneous | Japanese | ASD-M: 19 | 100.74 | ASD-M: 15M/4F | Japanese |
| TD-B: 20 | 100.12 | TD-B: 16M/4F | ||||||||
| TD-M: 15 | 107.20 | TD-M: 11M/4F | ||||||||
| Reetzke et al.45 | 2015 | 23 | 60.78 | 18M/5F | Simultaneous | Chinese | ASD-M: 31 | 59.77 | 25M/6F | Chinese |
| Sequential | ||||||||||
ASD: autistic spectrum disorder; ASD-B: bilingual children with ASD; ASD-M: monolingual children with ASD; F: female; M: male; NR: not reported; TD-B: bilingual children with typical development; TD-M: monolingual children with typical development.
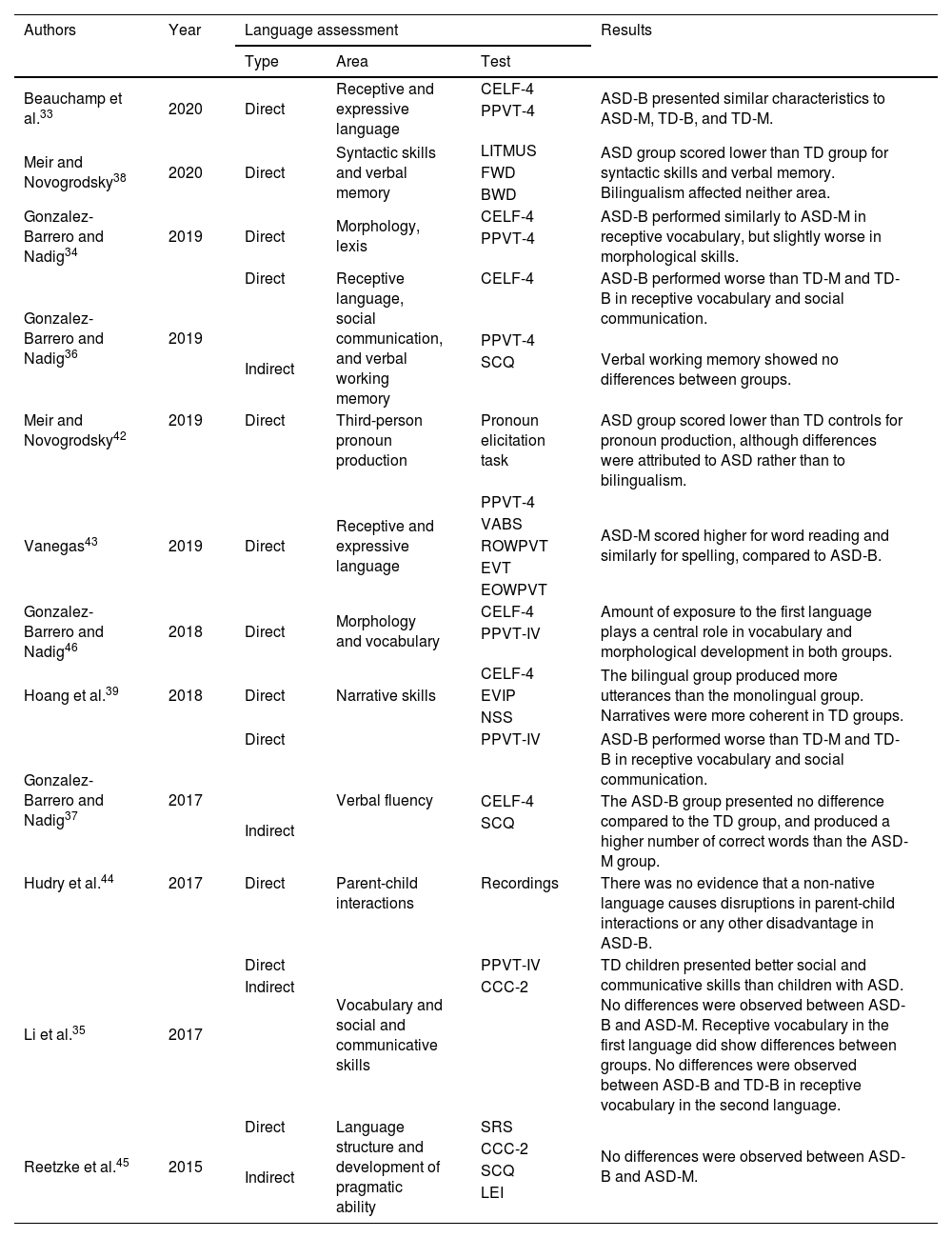
Assessment characteristics and main results of the studies reviewed.
| Authors | Year | Language assessment | Results | ||
|---|---|---|---|---|---|
| Type | Area | Test | |||
| Beauchamp et al.33 | 2020 | Direct | Receptive and expressive language | CELF-4 | ASD-B presented similar characteristics to ASD-M, TD-B, and TD-M. |
| PPVT-4 | |||||
| Meir and Novogrodsky38 | 2020 | Direct | Syntactic skills and verbal memory | LITMUS | ASD group scored lower than TD group for syntactic skills and verbal memory. Bilingualism affected neither area. |
| FWD | |||||
| BWD | |||||
| Gonzalez-Barrero and Nadig34 | 2019 | Direct | Morphology, lexis | CELF-4 | ASD-B performed similarly to ASD-M in receptive vocabulary, but slightly worse in morphological skills. |
| PPVT-4 | |||||
| Gonzalez-Barrero and Nadig36 | 2019 | Direct | Receptive language, social communication, and verbal working memory | CELF-4 | ASD-B performed worse than TD-M and TD-B in receptive vocabulary and social communication. |
| Indirect | PPVT-4 | Verbal working memory showed no differences between groups. | |||
| SCQ | |||||
| Meir and Novogrodsky42 | 2019 | Direct | Third-person pronoun production | Pronoun elicitation task | ASD group scored lower than TD controls for pronoun production, although differences were attributed to ASD rather than to bilingualism. |
| Vanegas43 | 2019 | Direct | Receptive and expressive language | PPVT-4 | ASD-M scored higher for word reading and similarly for spelling, compared to ASD-B. |
| VABS | |||||
| ROWPVT | |||||
| EVT | |||||
| EOWPVT | |||||
| Gonzalez-Barrero and Nadig46 | 2018 | Direct | Morphology and vocabulary | CELF-4 | Amount of exposure to the first language plays a central role in vocabulary and morphological development in both groups. |
| PPVT-IV | |||||
| Hoang et al.39 | 2018 | Direct | Narrative skills | CELF-4 | The bilingual group produced more utterances than the monolingual group. Narratives were more coherent in TD groups. |
| EVIP | |||||
| NSS | |||||
| Gonzalez-Barrero and Nadig37 | 2017 | Direct | Verbal fluency | PPVT-IV | ASD-B performed worse than TD-M and TD-B in receptive vocabulary and social communication. |
| Indirect | CELF-4 | The ASD-B group presented no difference compared to the TD group, and produced a higher number of correct words than the ASD-M group. | |||
| SCQ | |||||
| Hudry et al.44 | 2017 | Direct | Parent-child interactions | Recordings | There was no evidence that a non-native language causes disruptions in parent-child interactions or any other disadvantage in ASD-B. |
| Li et al.35 | 2017 | Direct | Vocabulary and social and communicative skills | PPVT-IV | TD children presented better social and communicative skills than children with ASD. No differences were observed between ASD-B and ASD-M. Receptive vocabulary in the first language did show differences between groups. No differences were observed between ASD-B and TD-B in receptive vocabulary in the second language. |
| Indirect | CCC-2 | ||||
| Reetzke et al.45 | 2015 | Direct | Language structure and development of pragmatic ability | SRS | No differences were observed between ASD-B and ASD-M. |
| Indirect | CCC-2 | ||||
| SCQ | |||||
| LEI | |||||
ASD: autistic spectrum disorders; ASD-B: bilingual children with ASD; ASD-M: monolingual children with ASD; BWD: Hebrew Backward Digit Span; CCC-2: Children’s Communication Checklist-241; CELF-4: Clinical Evaluation of Language Fundamentals, fourth edition32; EOWPVT: expressive one-word picture vocabulary test50; ÉVIP-II: Évaluation de Vocabulaire en Image Peabody-deuxième edition; EVT: expressive vocabulary test51; FWD: Hebrew forward digit span; LEI: language environment interview; LITMUS: the Russian LITMUS-CLT task48; MCDIs: MacArthur Communicative Development Inventory: words and sentences52; MSEL: Mullen Scales of Early Learning53; NSS: Narrative Scoring Scheme54; PPVT-4: Peabody Picture Vocabulary31; ROWPVT: Receptive One-Word Picture Vocabulary Test50; SCQ: Social Communication Questionnaire40; SRS: social responsiveness scale55; TD: typically developing children; TD-B: bilingual TD children; TD-M: monolingual TD children; VABS-II: Vineland Adaptive Behavior Scale-Communication Subscale.49
The total sample for all studies included 613 children, 328 (53.51%) of whom had a diagnosis of ASD. The TD group included 285 children (46.49%), of whom 127 were bilingual and 111 were monolingual; the number of languages spoken was not specified for the remaining 47. The study samples are heterogeneous. Firstly, the age of participants ranged from 4 to 9 years. The weighted mean age was 6.96 years for ASD-B, 6.80 years for ASD-M, 7.32 years for TD-B, and 7.41 years for TD-M. The majority of participants were boys (72.78%). Most studies (58.33%) included simultaneously bilingual patients with ASD (n=69); 2 also included patients with sequential bilingualism (n=3). Five studies (41.67%) did not report the type of bilingualism. The dominant language was French in 6 studies (50%), English in 5 (42%), Russian in 2 (17%), and Japanese and Chinese in one study each (8%).
The studies reviewed displayed great homogeneity in terms of language assessment, with 100% opting to conduct direct assessment. Indirect assessment, with data reported by parents, was also conducted in 33.33%. The different studies assessed a diverse range of language domains: receptive language, expressive language, and social and pragmatic communication. The most frequently studied characteristic was receptive vocabulary, in 7 studies (58.33%). The most frequently used assessment instruments were the Peabody Picture Vocabulary Test (PPVT-IV)31 and the Clinical Evaluation of Language Fundamentals (CELF-4),32 in 6 (50%) and 5 studies (42%), respectively.
Synthesis of evidenceThe majority of studies report similar findings, observing no difference between ASD-B and ASD-M in diverse areas of language.
According to the age of each study sample, the 2 studies including ASD-B younger than 6 years found no language differences compared to ASD-M; studies including older children report mixed results. Unfortunately, we are unable to analyse results by sex or type of bilingualism as the studies reviewed do not report differences between sexes, and the studies indicating the type of bilingualism all included samples of patients with simultaneous bilingualism.
With regard to language assessment, heterogeneous results are reported, according to the area assessed. Specifically, mixed results are reported for receptive vocabulary. Three studies33–35 found no differences between the comparison groups and ASD-B, whereas 2 studies36,37 report lower-than-expected receptive vocabulary in the ASD-B group. Results for working memory and verbal fluency are mixed,36–38 although morphological skills did show differences.34 Regarding narrative skills, one study found that although the ASD-B group produced more utterances, the narrative was not as coherent as in TD children.39 ASD-B children also show poorer social communication skills (evaluated with the Social Communication Questionnaire [SCQ]40 and Children’s Communication Checklist-2 [CCC-2]41).35–37 These children also show poorer syntactic skills, spelling, and third-person pronoun use.40,42,43 However, as most studies used direct assessment, it was not possible to analyse results according to the type of assessment used.
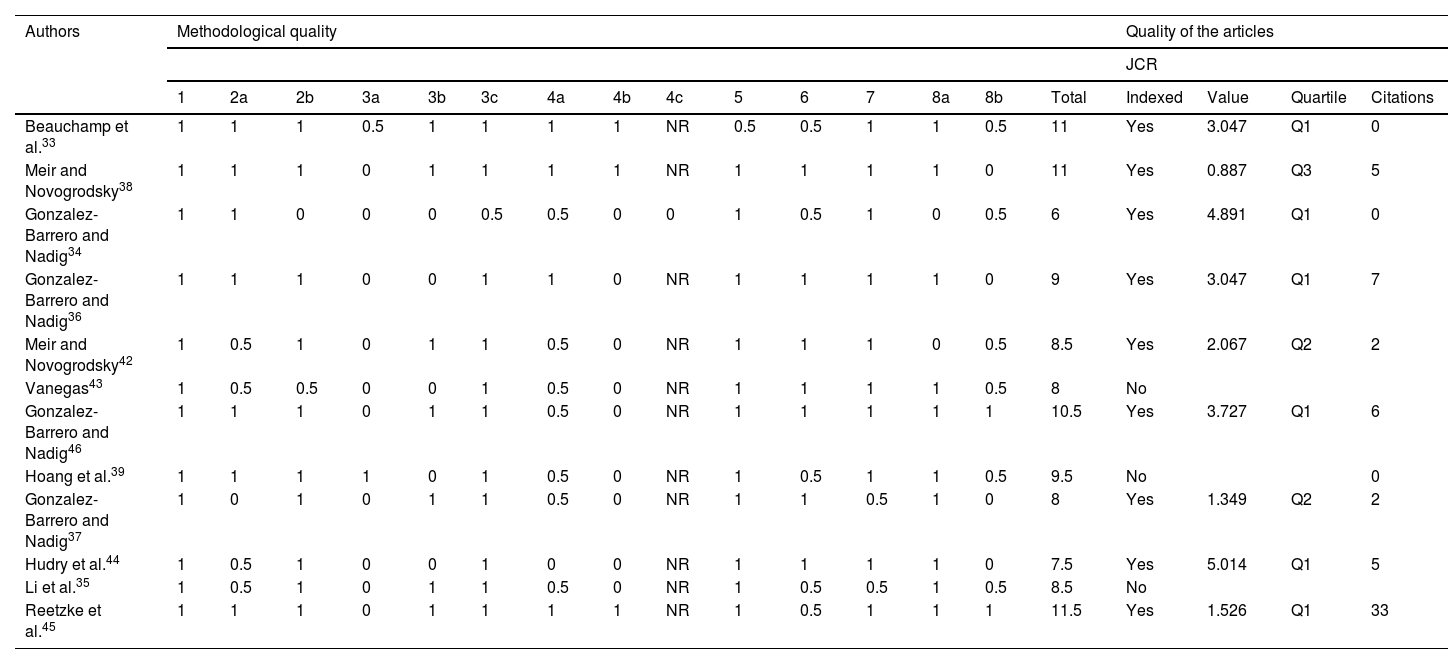
Methodological quality of the studiesAccording to the methodological quality assessment (Table 4; Fig. 2), 25% of studies were of high quality and 75% of moderate quality. Specifically, studies scored between 6 and 11 out of a maximum of 14 points; the mean score was 9 (Table 1). Therefore, studies presented moderate-high quality on average.
Methodological quality of studies included in the literature review.
| Authors | Methodological quality | Quality of the articles | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| JCR | |||||||||||||||||||
| 1 | 2a | 2b | 3a | 3b | 3c | 4a | 4b | 4c | 5 | 6 | 7 | 8a | 8b | Total | Indexed | Value | Quartile | Citations | |
| Beauchamp et al.33 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | NR | 0.5 | 0.5 | 1 | 1 | 0.5 | 11 | Yes | 3.047 | Q1 | 0 |
| Meir and Novogrodsky38 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | NR | 1 | 1 | 1 | 1 | 0 | 11 | Yes | 0.887 | Q3 | 5 |
| Gonzalez-Barrero and Nadig34 | 1 | 1 | 0 | 0 | 0 | 0.5 | 0.5 | 0 | 0 | 1 | 0.5 | 1 | 0 | 0.5 | 6 | Yes | 4.891 | Q1 | 0 |
| Gonzalez-Barrero and Nadig36 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | NR | 1 | 1 | 1 | 1 | 0 | 9 | Yes | 3.047 | Q1 | 7 |
| Meir and Novogrodsky42 | 1 | 0.5 | 1 | 0 | 1 | 1 | 0.5 | 0 | NR | 1 | 1 | 1 | 0 | 0.5 | 8.5 | Yes | 2.067 | Q2 | 2 |
| Vanegas43 | 1 | 0.5 | 0.5 | 0 | 0 | 1 | 0.5 | 0 | NR | 1 | 1 | 1 | 1 | 0.5 | 8 | No | |||
| Gonzalez-Barrero and Nadig46 | 1 | 1 | 1 | 0 | 1 | 1 | 0.5 | 0 | NR | 1 | 1 | 1 | 1 | 1 | 10.5 | Yes | 3.727 | Q1 | 6 |
| Hoang et al.39 | 1 | 1 | 1 | 1 | 0 | 1 | 0.5 | 0 | NR | 1 | 0.5 | 1 | 1 | 0.5 | 9.5 | No | 0 | ||
| Gonzalez-Barrero and Nadig37 | 1 | 0 | 1 | 0 | 1 | 1 | 0.5 | 0 | NR | 1 | 1 | 0.5 | 1 | 0 | 8 | Yes | 1.349 | Q2 | 2 |
| Hudry et al.44 | 1 | 0.5 | 1 | 0 | 0 | 1 | 0 | 0 | NR | 1 | 1 | 1 | 1 | 0 | 7.5 | Yes | 5.014 | Q1 | 5 |
| Li et al.35 | 1 | 0.5 | 1 | 0 | 1 | 1 | 0.5 | 0 | NR | 1 | 0.5 | 0.5 | 1 | 0.5 | 8.5 | No | |||
| Reetzke et al.45 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | NR | 1 | 0.5 | 1 | 1 | 1 | 11.5 | Yes | 1.526 | Q1 | 33 |
NR: not reported.

With regard to the assessment of article quality (Table 4), 75% were indexed on JCR. Specifically, 50% were published in quartile 1 journals, 17% in quartile 2 journals, and 8% in quartile 3 journals. Regarding the JCR index, articles presented a mean value of 2.84; the mean number of citations on WOS was 6.00.
DiscussionThe aim of this review is to describe and synthesise the available evidence from the last 5 years on the impact of bilingualism on language in children older than 3 years with ASD, and to analyse a range of factors with the potential to influence the reported findings.
The majority of studies conclude that bilingualism does not have a negative impact on language in ASD. This contrasts with a widespread belief among the families of these children, also shared by some healthcare professionals, that children with ASD raised in a bilingual environment may have greater difficulty in language development.10 Furthermore, bilingualism and its effect on language in children with ASD is a subject of considerable interest, given the great repercussions on the family setting and on education. This is supported by the fact that 50% of the articles reviewed were published in the last 2 years.
Although the overall results suggest that bilingualism is not associated with any negative impact on language in ASD, the results are not homogeneous and certain peculiarities must be taken into account. It is important to note that, while not all of the studies analysed mention the sex of the participants, the great majority were boys due to the much lower prevalence of ASD in girls (Baio et al.33 report a male-to-female ratio of 4:1). Most studies include participants with simultaneous bilingualism, either because the parents had different first languages or because the language spoken at school was different to the language spoken at home.
A diverse range of language variables were studied, with nearly all aspects of receptive language being addressed by some study. These included lexical, grammatical, and syntactic skills, as well as verbal fluency and word production. Lexis was one of the most extensively studied areas, addressed in more than half of studies.
After analysis of factors potentially affecting outcomes, the age of the participants and the language domain assessed seem to have an effect. Regarding age, despite the lack of differences between ASD-B, ASD-M, and TD-B in children younger than 6 years,46,47 differences do appear after that age.
With respect to language domains, results for receptive vocabulary, verbal working memory, and verbal fluency are inconclusive.19,33–36,38 However, ASD-B children do display differences compared to the other groups in morphological and syntactic skills, spelling, narrative coherence, production of third-person pronouns, and social communication.19,34–36,38,39,42,43
Regarding vocabulary in particular, the study by González-Barrero and Nadig46 found that the level of exposure to language plays a key role in the development of lexical and morphological skills, both in TD children and those with ASD. ASD-B children presented very similar scores to controls for receptive vocabulary.34 In verbal fluency, ASD-B children presented no significant differences with respect to TD children, although they did display a somewhat lower number of correct words produced.37
Bilingual children also showed greater narrative coherence than monolingual children.39 However, ASD-M and TD children scored slightly higher than ASD-B children for verbal memory, pronoun production, and word reading.42,43
Unfortunately, we were unable to analyse the potential effects of sex, type of bilingualism, and type of assessment, as the studies reviewed were homogeneous with respect to these variables. However, some articles did use indirect assessment, with such instruments as the CCC-2 and SCQ,41,42 to complement the direct assessment, reaching similar conclusions to those derived from direct assessment.
Clinical implicationsBased on the findings from our review, and despite the relatively small number of articles identified, there appear not to be differences between ASD-B and ASD-M children in different areas of language.33 It is essential for healthcare professionals to provide guidance to the families of children with ASD living in bilingual settings on the subject of second language acquisition, reassuring them that this will not lead to deficits in development. On the contrary, children will benefit from the learning and development inherent to bilingualism. Despite this, Yu12 asserts that families’ language-related decisions in their children with ASD depend on the languages used at home and at school/in the community, as well as the social prestige associated with each. Furthermore, there is a need to broaden training in this field to ensure that healthcare professionals can adequately advise families, taking into account sociocultural factors.
The conclusions of this study are relevant both in the research setting and in clinical practice. The strengths of the review are the fact that the literature search was conducted in 4 different databases, and that we analysed the quality both of the studies and of the selected articles, as well as the potential influence of different factors on the results reported. Therefore, this review both complements the findings of previous systematic reviews on the subject, and paves the way for future lines of research.
LimitationsThis review presents certain limitations that should be addressed and resolved in future studies. With regard to the study methodology, the search terms and descriptors used may have limited the studies identified and analysed. As noted throughout the article, the great heterogeneity observed in the areas of language studied made it difficult to analyse results as a function of certain variables and to draw generalisable conclusions.
Future studies should consider employing larger samples and longitudinal designs, with follow-up until adolescence or adulthood, in order to establish whether the linguistic conditions observed persist and to extrapolate their findings. Furthermore, similar studies could be conducted in other populations with different disorders with a view to assisting healthcare professionals working with patients presenting such comorbidities as Down syndrome, intellectual disability, or attention-deficit/hyperactivity disorder.
ConclusionsThis review of the available evidence demonstrates the importance of different components of language for second language acquisition in a bilingual environment in children with ASD. Most of the studies reviewed conclude that simultaneous language development has no negative effect for children with ASD, and does not represent an additional hindrance in any area of language development. Therefore, they support the assertion that bilingualism does not negatively impact language development in these children, as suggested by Nichols et al.56 In conclusion, there is a great need for further studies to continue developing these lines of research, which may be beneficial both for clinicians and for the quality of life of bilingual children with ASD and their families.
FundingThis study has received no specific funding from any public, commercial, or non-profit organisation.
Conflicts of interestThe authors have no conflicts of interest to declare.
