



Progressive deterioration in patients with amyotrophic lateral sclerosis (ALS) has a major impact on their health-related quality of life (HRQOL). The objectives of this study are to evaluate HRQOL in a sample of patients diagnosed with ALS and estimate the predictive capability of a set of sociodemographic variables for the different scales covered by a general health survey.
MethodsA total of 63 patients diagnosed with ALS were assessed using a sociodemographic questionnaire and the SF-36 general health survey. The sociodemographic variables studied were sex, age, presence of a caregiver, employment status, and time from diagnosis of disease.
ResultsThe SF-36 survey shows positive correlations between the different scales composing it, which proves its reliability. The mean scores obtained for each of the SF-36 scales were higher in men than in women, although the only statistically significant difference was for the Physical Role scale. The lowest age range (less than 56 years) presented the highest mean scores for most of these dimensions. Most of the variance in the test is explained by the variable ‘presence of caregiver’.
ConclusionsThe SF-36 health survey has been confirmed as a valid and useful tool for evaluating HRQOL in ALS patients, and it discriminates between patients in different states of health according to their level of dependency.
El deterioro progresivo de los pacientes con esclerosis lateral amiotrófica (ELA) genera un gran impacto sobre su calidad de vida relacionada con la salud (CVRS). En este estudio se evalúa la CVRS en una muestra de pacientes diagnosticados de ELA y se pretende estimar la capacidad predictiva de un conjunto de variables sociodemográficas en las distintas dimensiones que conforman el cuestionario.
MétodosSe evaluó a un total de 63 pacientes diagnosticados de ELA, a través de un cuestionario sociodemográfico y del cuestionario genérico de salud SF-36. Se estudiaron variables sociodemográficas como sexo, edad, existencia de cuidador, situación laboral y tiempo desde el diagnóstico de la enfermedad.
ResultadosEl cuestionario SF-36 muestra una correlación positiva entre las diferentes dimensiones que la componen lo que demuestra su confiabilidad. Las puntuaciones medias obtenidas en cada una de las dimensiones del SF-36 son mayores en hombres que en mujeres, aunque esta diferencia es significativa solo en la dimensión Rol físico, siendo el grupo de pacientes de menor edad (menos de 56 años) quienes presentan puntuaciones medias más altas en la mayoría de las dimensiones del SF-36. La mayor parte de la variancia de la prueba queda explicada por la variable existencia de cuidador.
ConclusionesSe confirma la capacidad del SF-36 como medida válida y fiable de la CVRS para pacientes con un diagnóstico de ELA, que discrimina entre pacientes con diferentes estados de salud según su nivel de dependencia.
Patients’ degree of health and health-related quality of life (HRQoL) are increasingly important as means of estimating the results of healthcare programmes or interventions. Although there is no consensus on the definition of HRQoL, most authors maintain that it is a subjective, multidimensional concept according to which health is associated with a number of factors rather than being defined as the mere absence of illness. The definition of HRQoL proposed by Shumaker and Naughton (1995) in a review of existing definitions may be one of the most useful: “people's subjective evaluations of the influences of their current health status, health care, and health-promoting activities on their ability to achieve and maintain a level of overall functioning that allows them to pursue valued life goals, and that is reflected in their general well-being”.1
The most relevant dimensions related to HRQoL are social, physical, and cognitive function; mobility and personal care; and emotional well-being. This definition is based on an individual's impression of his or her health, and it is often used interchangeably with the concept of self-perceived health. The construct of HRQoL is therefore an overarching and multidimensional concept referring to both objective conditions and subjective components, and these include all relevant and health-related aspects of the patient's life.2
Nevertheless, this construct has undergone significant developments as it has evolved from offering an awareness-raising perspective to becoming an agent for change. In this way, it has had an impact on health policy, clinical practice, and the evaluation of healthcare services, as a means of identifying outcome-predicting variables.3
One of the neurodegenerative diseases with the most serious effects on HRQoL is amyotrophic lateral sclerosis (ALS). ALS is an incurable progressive neuromuscular disorder with an incidence of approximately 2 out of 100000 residents.4 In advanced stages of the disease, patients present complete paralysis accompanied by exaggerated deep tendon reflexes as a result of loss of inhibitory control over muscle. Cognitive dysfunction also arises in 20% to 50% of all cases, and dementia in 5% to 15%. Most of these cases are frontotemporal dementia, with executive dysfunction and behavioural changes. At the same time, other brain functions remain unaltered, including intelligence and sensory perception; likewise, there are no changes in motor neurons that control extrinsic eye muscles or the muscles responsible for sphincter control.5,6 Death by respiratory failure occurs 2 to 4 years after onset of symptoms, although between 5% and 10% of patients may live for a decade or more.7 Age at onset is typically between 43 and 52 years.8
Patients with ALS suffer from multiple symptoms including pain, fatigue, dyspnoea, and sialorrhoea. Emotional challenges are also extreme, involving loss of independence, loss of the ability to communicate, and hopelessness. ALS elicits a progressive decrease in autonomy and increased need for assistance in all activities of daily life. Carers must also dedicate increasing amounts of time to patient care, and their social and personal burden increases9,10 as their task becomes more psychologically and emotionally difficult.11,12 If the patient effectively loses the ability to communicate, a carer may feel intellectually and emotionally isolated.13,14 Emotional lability is experienced by at least 50% of this patient population, but it is not correlated with cognitive impairment.15,16
The functional disability resulting from this type of disease is such that after a few years of disease progression, many patients present significant decreases in both autonomy and in HRQoL. For this reason, daily care for patients rests with family members in most cases. This situation contributes to a lower quality of life in the family unit, and its economic impact is also significant. As a result, healthcare planning for this group of patients and their families should be oriented towards preserving HRQoL for patients as much as possible, and towards providing support for families involved in caregiving tasks.4,9,17–21 Factors such as perceived physical health, psychological state, independence levels, social relationships, and relationship with surroundings are vital to our success in the complex task of providing quality of life standards for these patients and their families.
For all these reasons, the objectives of this article are as follows: (a) to describe the specific characteristics of self-perceived health in a sample of patients diagnosed with ALS, using the SF-36 questionnaire as an assessment tool and (b) to estimate the predictive ability of a set of sociodemographic variables for the different dimensions that make up the questionnaire.
Patients and methodsThis transversal study included 63 patients diagnosed with ALS. Patients were recruited with the help of patient associations from 7 Spanish autonomous communities. In addition, we contacted members of the epidemiological network for research into rare diseases at Instituto de Salud Carlos III. In order to participate, patients had to meet the El Escorial World Federation of Neurology criteria for the diagnosis of ALS,22 and that diagnosis had to have been confirmed by a neurologist. Both patients and carers provided their informed consent before participating in the study. The procedure was approved by local clinical research ethics committees.
The study was based on information provided in the form of 2 self-administered surveys that were sent to patients and carers by physical mail. Participants who did not respond to the first mailing received a reminder 8 weeks after the surveys had been sent.
The first questionnaire collected sociodemographic information, including sex, age, time since diagnosis, carer presence, and employment status. Patients were grouped into 3 age ranges: 55 and younger, 56 to 66, and older than 66. Time since diagnosis was also classified into 3 groups: 18 months or less, between 18 months and 3 years, and more than 3 years. Employment status was presented as 4 categories: actively employed, home-maker, on temporary or permanent disability leave, or retired.
The second questionnaire evaluated the HRQoL of participants using the Spanish version of the SF-36 Health Survey.23,24 This questionnaire was developed for use in the Medical Outcomes Study, which contains a full battery of questionnaires that cover 40 health concepts.25 The questionnaire was modified in 1989 and once again in 1992 to give it its current form.26 The 1992 modification has given rise to different 12-item, 20-item, and 24-item versions, as well as a preference-based utility index (SF-6D). Despite the above, the 36-item version remains the most widely used in research and in the evaluation of clinical results. It is applicable to both the general population and to specific patient groups.27
SF-36 is a generic 36-item instrument that covers 8 health dimensions and profiles the patient's state of health. Its items detect both positive and negative aspects of health. For each dimension, items are coded, added up, and transformed into scores on a scale of 0 (the poorest state of health for that dimension) to 100 (the best state of health). This questionnaire was designed to deliver a global index. Its adaptation for the population of Spain has been shown to have good reliability and validity levels, and it is culturally equivalent to versions used in other countries.28 Furthermore, there are reference values for SF-36 scores in the general Spanish population which offer the possibility of evaluating the impact of the disease and the benefits of the health services both qualitatively and quantitatively.29–31
When analysing results, we used descriptive and exploratory data analysis methods applied to the different study variables. For comparison of means, t-tests were used according to needs of the study and the suitability of those tests with regard to the stated objectives.
Correlations between the different dimensions of the scale were estimated using Pearson's correlation coefficient.
Likewise, we created a stepwise linear regression model to estimate the predictive ability of each of the sociodemographic study variables on each of the dimensions included in SF-36. The model was tested for goodness of fit using the determination coefficient (R2). The test of whether the adjusted regression model explained a significant part of overall variability was performed using regression analysis of variance. We recorded confidence intervals, t-test values, and the coefficients’ significance levels. We also checked for data linearity, homoscedasticity, and normality using residual analysis. The Durbin–Watson statistic for serially correlated residuals was applied, along with methods for determining variance inflation factor (VIF) and tolerance.
ResultsA total of 63 patients diagnosed with ALS responded to the questionnaires. Men accounted for 55.4% (n=33) and women, 47.6% (n=30) of this total. Participants’ ages ranged from 21 to 78 years (mean±typical deviation=59.10±10.30); 88.9% of the patients were married or had a domestic partner (n=56) while 11.1% (n=7) lived alone. The most common employment situation in this sample was one of temporary or permanent disability leave, accounting for 49.2% of the population (n=31). This was followed by retirement in 27% (n=17), home-making in 17.5% (n=11), and active employment in 1.6% (n=1). Three patients (4.8%) did not answer the question. Patients had been diagnosed 18 months ago or less in 34.9% of the cases (n=22); between 18 months and 3 years in 28.6% (n=18); and more than 3 years ago in 30.2% (n=19). Four patients (6.3%) answered ‘unknown’ or left the question blank.
Carers assisted 77.8% of the patients (n=49), leaving 14 patients without carers (22.2%). Carers were predominantly female (in 44.4% of the total cases; n=28), with 28.6% of the total cared for by men (n=18). Three patients (4.8%) did not specify carer sex.
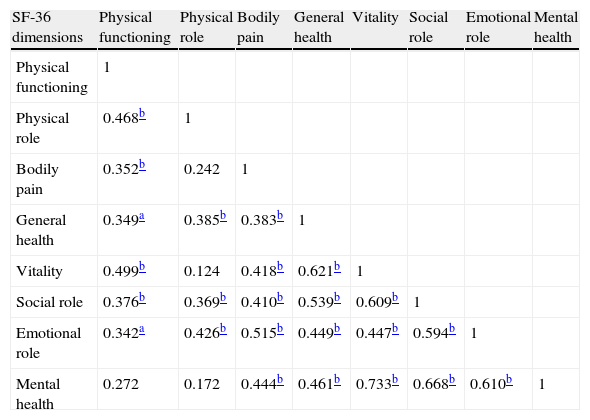
The highest correlation between different dimensions of the SF-36 was between the mental health and vitality dimensions (0.733); the lowest correlation was between emotional and physical role functioning (0.342). The statistical significance level was 0.01 in both cases. An important observation is that emotional role functioning, general health, and social role functioning all show positive, significant correlations to each of the dimensions in the questionnaire. Bodily pain is the dimension with the lowest number of significant correlations (see Table 1).
Correlations between different SF-36 dimensions.
| SF-36 dimensions | Physical functioning | Physical role | Bodily pain | General health | Vitality | Social role | Emotional role | Mental health |
| Physical functioning | 1 | |||||||
| Physical role | 0.468b | 1 | ||||||
| Bodily pain | 0.352b | 0.242 | 1 | |||||
| General health | 0.349a | 0.385b | 0.383b | 1 | ||||
| Vitality | 0.499b | 0.124 | 0.418b | 0.621b | 1 | |||
| Social role | 0.376b | 0.369b | 0.410b | 0.539b | 0.609b | 1 | ||
| Emotional role | 0.342a | 0.426b | 0.515b | 0.449b | 0.447b | 0.594b | 1 | |
| Mental health | 0.272 | 0.172 | 0.444b | 0.461b | 0.733b | 0.668b | 0.610b | 1 |
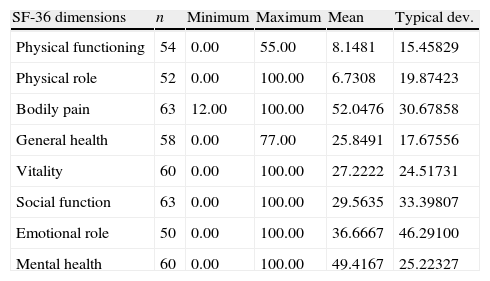
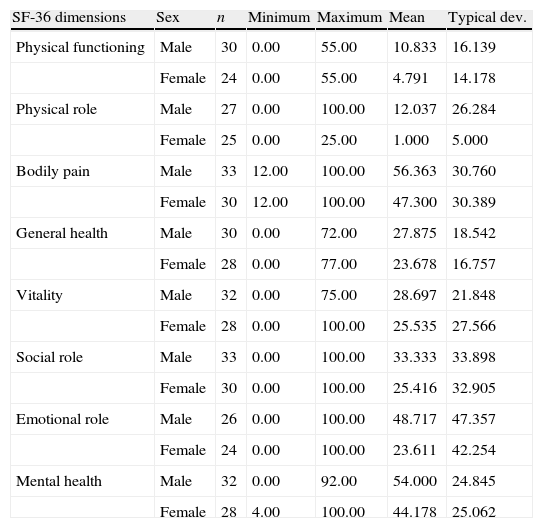
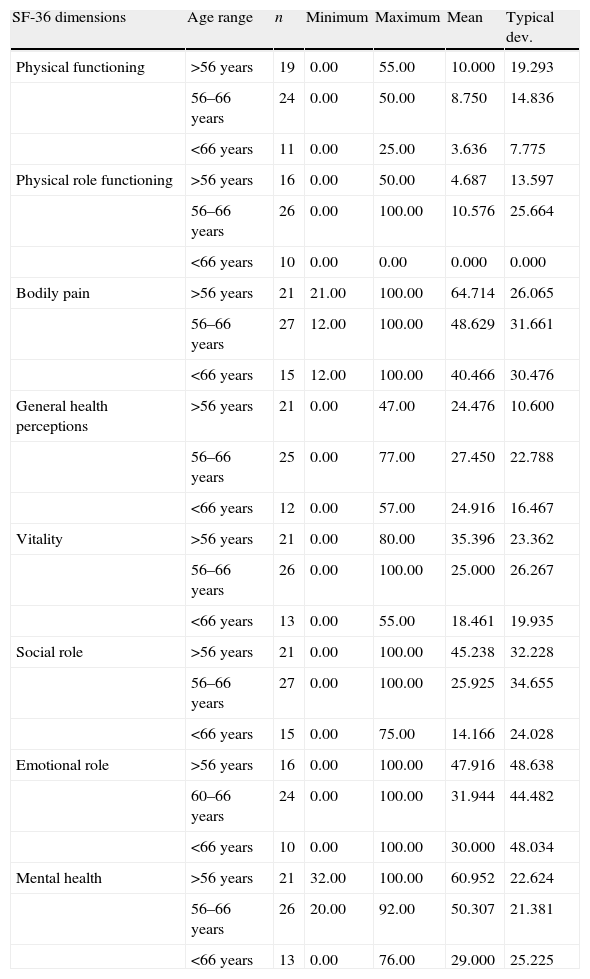
Descriptive results for the SF-36 dimensions are shown in Table 2; mean scores for the different SF-36 dimensions are displayed by sex in Table 3 and age range in Table 4. As we see, the mean score for all dimensions is higher in men than in women. Regarding age, mean scores were higher in the youngest age range (younger than 56) except for the physical role and general health dimensions, whose highest means were found in the middle age range (patients between 56 and 66).
Minimum, maximum, mean, and typical deviation in SF-36 dimensions.
| SF-36 dimensions | n | Minimum | Maximum | Mean | Typical dev. |
| Physical functioning | 54 | 0.00 | 55.00 | 8.1481 | 15.45829 |
| Physical role | 52 | 0.00 | 100.00 | 6.7308 | 19.87423 |
| Bodily pain | 63 | 12.00 | 100.00 | 52.0476 | 30.67858 |
| General health | 58 | 0.00 | 77.00 | 25.8491 | 17.67556 |
| Vitality | 60 | 0.00 | 100.00 | 27.2222 | 24.51731 |
| Social function | 63 | 0.00 | 100.00 | 29.5635 | 33.39807 |
| Emotional role | 50 | 0.00 | 100.00 | 36.6667 | 46.29100 |
| Mental health | 60 | 0.00 | 100.00 | 49.4167 | 25.22327 |
Minimum, maximum, mean, and typical deviation in SF-36 dimensions broken down by sex.
| SF-36 dimensions | Sex | n | Minimum | Maximum | Mean | Typical dev. |
| Physical functioning | Male | 30 | 0.00 | 55.00 | 10.833 | 16.139 |
| Female | 24 | 0.00 | 55.00 | 4.791 | 14.178 | |
| Physical role | Male | 27 | 0.00 | 100.00 | 12.037 | 26.284 |
| Female | 25 | 0.00 | 25.00 | 1.000 | 5.000 | |
| Bodily pain | Male | 33 | 12.00 | 100.00 | 56.363 | 30.760 |
| Female | 30 | 12.00 | 100.00 | 47.300 | 30.389 | |
| General health | Male | 30 | 0.00 | 72.00 | 27.875 | 18.542 |
| Female | 28 | 0.00 | 77.00 | 23.678 | 16.757 | |
| Vitality | Male | 32 | 0.00 | 75.00 | 28.697 | 21.848 |
| Female | 28 | 0.00 | 100.00 | 25.535 | 27.566 | |
| Social role | Male | 33 | 0.00 | 100.00 | 33.333 | 33.898 |
| Female | 30 | 0.00 | 100.00 | 25.416 | 32.905 | |
| Emotional role | Male | 26 | 0.00 | 100.00 | 48.717 | 47.357 |
| Female | 24 | 0.00 | 100.00 | 23.611 | 42.254 | |
| Mental health | Male | 32 | 0.00 | 92.00 | 54.000 | 24.845 |
| Female | 28 | 4.00 | 100.00 | 44.178 | 25.062 |
Minimum, maximum, mean, and typical deviation for SF-36 broken down by age range.
| SF-36 dimensions | Age range | n | Minimum | Maximum | Mean | Typical dev. |
| Physical functioning | >56 years | 19 | 0.00 | 55.00 | 10.000 | 19.293 |
| 56–66 years | 24 | 0.00 | 50.00 | 8.750 | 14.836 | |
| <66 years | 11 | 0.00 | 25.00 | 3.636 | 7.775 | |
| Physical role functioning | >56 years | 16 | 0.00 | 50.00 | 4.687 | 13.597 |
| 56–66 years | 26 | 0.00 | 100.00 | 10.576 | 25.664 | |
| <66 years | 10 | 0.00 | 0.00 | 0.000 | 0.000 | |
| Bodily pain | >56 years | 21 | 21.00 | 100.00 | 64.714 | 26.065 |
| 56–66 years | 27 | 12.00 | 100.00 | 48.629 | 31.661 | |
| <66 years | 15 | 12.00 | 100.00 | 40.466 | 30.476 | |
| General health perceptions | >56 years | 21 | 0.00 | 47.00 | 24.476 | 10.600 |
| 56–66 years | 25 | 0.00 | 77.00 | 27.450 | 22.788 | |
| <66 years | 12 | 0.00 | 57.00 | 24.916 | 16.467 | |
| Vitality | >56 years | 21 | 0.00 | 80.00 | 35.396 | 23.362 |
| 56–66 years | 26 | 0.00 | 100.00 | 25.000 | 26.267 | |
| <66 years | 13 | 0.00 | 55.00 | 18.461 | 19.935 | |
| Social role | >56 years | 21 | 0.00 | 100.00 | 45.238 | 32.228 |
| 56–66 years | 27 | 0.00 | 100.00 | 25.925 | 34.655 | |
| <66 years | 15 | 0.00 | 75.00 | 14.166 | 24.028 | |
| Emotional role | >56 years | 16 | 0.00 | 100.00 | 47.916 | 48.638 |
| 60–66 years | 24 | 0.00 | 100.00 | 31.944 | 44.482 | |
| <66 years | 10 | 0.00 | 100.00 | 30.000 | 48.034 | |
| Mental health | >56 years | 21 | 32.00 | 100.00 | 60.952 | 22.624 |
| 56–66 years | 26 | 20.00 | 92.00 | 50.307 | 21.381 | |
| <66 years | 13 | 0.00 | 76.00 | 29.000 | 25.225 |
In the next section, we will explain the significant differences among sociodemographic study variables with regard to each of the SF-36 dimensions.
- -
Physical functioning. This dimension showed significant differences in employment status (t[13]=2.639; P=.020) with higher scores among retired patients. This was also true of carer presence (t[16]=−2.454; P=.026), with scores being higher among patients without carers.
- -
Physical role functioning. There were significant sex differences, with men presenting higher scores (t[28]=2.140; P=.038). Age differences were also significant (t[25]=2.10; P=.046) with higher scores among patients in the middle age range (56–66 years).
- -
Bodily pain. There were significant differences for the age variable (t[34]=2.565; P=.015). Scores were higher among patients younger than 56. There were also significant differences associated with carer status (t[61]=2.699; P=.009) as patients without carers had higher scores. Scores were also higher for times since diagnosis of 18 months or less (t[38]=−2.137; P=.036).
- -
General health perceptions. In this dimension, there were only significant differences for employment status (t[21]=2.129; P=.044), with scores being higher for retired patients.
- -
Vitality. This dimension showed higher scores in patients younger than 56 (t[32]=2.168; P=.038). There were also significant differences for employment status (t[33]=−3.843; P=.001), with higher scores among patients on permanent or temporary disability leave.
- -
Social role functioning. Once again, age effect was significant in this dimension with higher scores among patients younger than 56 years (t[31]=3.155; P=.003); employment situation also showed significant differences, with higher scores in patients on permanent or temporary disability leave, as seen in the previous dimension (t[29]=2.160; P=.039).
- -
Mental health. This dimension showed significant age differences (t[32]=3.831; P=.001); scores were higher among patients younger than 56. The mental health dimension also showed variations with regard to employment status, since scores were higher in patients who were on permanent or temporary disability leave (t[38]=−3.321; P=.002). Differences were also statistically significant for time since diagnosis (t=[36]=−2.597; P=0.014); higher scores corresponded to patients who had been diagnosed more than 3 years before.
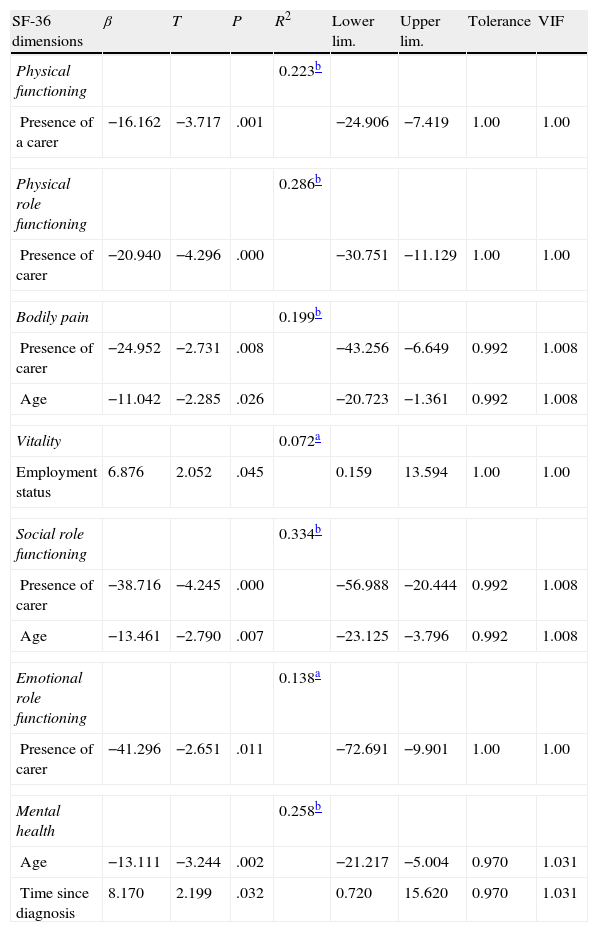
Lastly, taking into account the sociodemographic variables that accounted for significant differences in some of the dimensions making up the scale, we performed stepwise linear regression (Table 5).
Linear regression analysis of sociodemographic characteristics in SF-36 scores.
| SF-36 dimensions | β | T | P | R2 | Lower lim. | Upper lim. | Tolerance | VIF |
| Physical functioning | 0.223b | |||||||
| Presence of a carer | −16.162 | −3.717 | .001 | −24.906 | −7.419 | 1.00 | 1.00 | |
| Physical role functioning | 0.286b | |||||||
| Presence of carer | −20.940 | −4.296 | .000 | −30.751 | −11.129 | 1.00 | 1.00 | |
| Bodily pain | 0.199b | |||||||
| Presence of carer | −24.952 | −2.731 | .008 | −43.256 | −6.649 | 0.992 | 1.008 | |
| Age | −11.042 | −2.285 | .026 | −20.723 | −1.361 | 0.992 | 1.008 | |
| Vitality | 0.072a | |||||||
| Employment status | 6.876 | 2.052 | .045 | 0.159 | 13.594 | 1.00 | 1.00 | |
| Social role functioning | 0.334b | |||||||
| Presence of carer | −38.716 | −4.245 | .000 | −56.988 | −20.444 | 0.992 | 1.008 | |
| Age | −13.461 | −2.790 | .007 | −23.125 | −3.796 | 0.992 | 1.008 | |
| Emotional role functioning | 0.138a | |||||||
| Presence of carer | −41.296 | −2.651 | .011 | −72.691 | −9.901 | 1.00 | 1.00 | |
| Mental health | 0.258b | |||||||
| Age | −13.111 | −3.244 | .002 | −21.217 | −5.004 | 0.970 | 1.031 | |
| Time since diagnosis | 8.170 | 2.199 | .032 | 0.720 | 15.620 | 0.970 | 1.031 | |
For 3 dimensions, carer presence explained a significant part of the observed variance (physical functioning: r2=0.223; F[1,48]=13.814; P=.001; Durbin–Watson value=1.817. Physical role: r2=0.286; F[1,46]=18.457; P=.000; Durbin–Watson value=1.549. Emotional role: r2=0.138; F[1,44]=7.028; P=.011, Durbin–Watson value=1.992). Patients without carers had higher scores on these dimensions. On the ‘bodily pain’ and ‘social role’ dimensions, age and need for carer explained a significant part of the variance (Bodily pain: r2=0.199; F[2,56]=6.936; P=.002; Durbin–Watson value=2.079. Social role: r2=0.334; F[2,56]=14.040; P=.000; Durbin–Watson value=2.187). Younger patients (<56) and those without caregivers had higher scores on these dimensions.
Variance for the ‘vitality’ dimension was explained in part by employment situation (r2=0.072; F[1,54]=4.212; P=.045; Durbin–Watson value=1.783); patients on permanent or temporary disability leave had higher scores.
Two variables, age and time since diagnosis, explain part of the variance in the ‘mental health’ dimension (r2=0.258; F[2,53]=9.197; P=.000; Durbin–Watson value=1.837. Patients in the lowest age range (<56) and those with the longest time since diagnosis (>3 years) had the highest scores.
DiscussionFew studies have examined HRQoL among patients with ALS in Spain,32–34 despite the recent appearance of a growing number of international articles on HRQoL and ALS.35 Furthermore, most of the studies that do exist have small sample sizes. This situation seems to be linked to both the low frequency of the disease and ALS patients’ low rates of participation in this type of study.
The challenges we find when recruiting patients with rare diseases like ALS (low volumes of patients, geographical dispersion, etc.) may not be the same challenges and obstacles as those that arise in the study of other groups of patients with more common diseases.36 This is why researchers, when identifying and later recruiting potential participants in studies of patients with rare diseases, should use a variety of strategies favouring recruitment. On some occasions, these strategies may even differ from those we typically use to recruit patients with more frequent diseases.37 Such strategies include locating patients with the help of patient associations and support groups, which has been proved an effective means of recruitment.37,38
Most studies that focus on HRQoL in ALS have sample sizes similar to or smaller than the sample in our study.34,39–41 Nevertheless, the characteristics describing our participant sample (mean age and age range, sex distribution, degree of disability leave, and need for care) are in line with the general characteristics found in international literature on patients with ALS,33,40,42,43 and with the descriptions of patients belonging to the Spanish Association for Amyotrophic Lateral Sclerosis. This observation, together with the fact that sample sizes found in international literature are also small, make the results from this study comparable to those from earlier studies.41,44
Likewise, the use of standard instruments for measuring health (HRQoL) is being increasingly promoted as a fundamental way to gauge outcomes, whether in clinical trials or in surveys or descriptive studies like our own. In particular, the SF-36 is a widely used tool for measuring state of health, and it has been found to be useful and appropriate in patients with ALS. As earlier studies have shown,44,45 the SF-36 questionnaire used in ALS patients has discriminant ability for the different dimensions it measures.
Our study found positive and significant correlations between ‘emotional role functioning’, ‘general health perceptions’, and ‘social role functioning’ and all dimensions on this questionnaire. This leads us to believe that these aspects could greatly affect perception of HRQoL in these patients. Results include very low values for ‘physical functioning’ and ‘physical role functioning’, which clearly shows that patients have marked physical limitations, especially those affecting activities of daily life. Significant sex-related and age-related differences were also detected in these dimensions. The ‘physical role functioning’ dimension demonstrated significant sex differences, with men experiencing less interference with work and activities of daily living. Significant age differences were also detected for this dimension. Participants aged 56 to 66 (the middle range) experienced fewer difficulties on this dimension.
Significant differences in the ‘physical functioning’ dimension were related to the patient's employment situation; the best scores were found among pensioners and patients who did not need carers. These results do not concur with those obtained for ‘social role functioning’, ‘emotional role functioning’, and ‘mental health’, and this fact reinforces the concept of the well-being paradox described for ALS.32,41,46
These dimensions also show significant differences for some of the sociodemographic variables under study. In the ‘social role functioning’ and ‘mental health’ dimensions, the youngest patients and those on temporary or permanent disability leave had the best overall well-being and the lowest impact on social life. Based on these results, we can deduce that those patients on disability leave still had some contact with workplace and/or social activity.
The time since diagnosis variable is perhaps the most closely linked to the well-being paradox mentioned above. In our study, the highest scores on the ‘mental health’ dimension were found in patients with the longest times since diagnosis (more than 3 years). One explanation for this paradox may be the changing degrees of importance which patients attach to the different dimensions of self-perceived quality of life when they are in advanced or even terminal stages of the disease. It is possible that the development of coping strategies allows them to focus on and emphasise emotional and spiritual aspects of their lives that promote their mental health and morale (emotional role functioning), despite the physical impairment caused by rapidly progressing disease. These findings therefore call for meticulous evaluation and clinical management to improve the well-being of patients and their families.32,41,45
On the other hand, some authors have pointed out that some dimensions of the SF-36 may not be sensitive enough to measure change (deteriorating health) in patients with severe chronic illnesses or very elderly patients.35 This question was also raised by our study, since the ‘general health perceptions’ dimension, which was highly correlated with all other dimensions on the questionnaire, showed no significant differences for any of the sociodemographic study variables.
Regarding the variables explaining scores on the questionnaire, we observed that carer presence had an impact on a large part of the scores in the sample. Patients without carers assigned higher ratings to their HRQoL than patients who required assistance. As a result, presence of carers seems to be the best predictor of self-perceived quality of life among these patients.
In contrast, we find 2 dimensions that seem to be unaffected by carer presence. These are ‘vitality’, for which employment situation is the variable explaining only a low percentage of the variance, and ‘mental health’, for which time since diagnosis and age explain part of the variance.
These results may indicate that, given a lack of effective and proved therapeutic procedures for treating ALS and in light of the low availability of treatments that change the clinical course of the disease, measuring HRQoL may be a useful, valid, and practical strategy for understanding the response to symptomatic treatments and rehabilitation strategies that improve quality of life for these patients.35,47
Despite the limitations we listed for the recruitment process and sample size, this study provides relevant information about HRQoL in patients with ALS in our setting. It underlines the utility of SF-36 for this purpose and provides policy-makers and healthcare professionals with a profile of the needs of ALS patients and their families to permit revising the treatment strategies that improve and optimise their HRQoL.
FundingThis study was financed by FEDER [Spanish federation of rare diseases], Instituto de Salud Carlos III, Ministry of Health, Social Services, and Equality.
Conflicts of interestThe authors declare that they have no potential conflicts of interest related to the content of this article.
Please cite this article as: Sánchez-López CR, Perestelo-Pérez L, Ramos-Pérez C, López-Bastida J, Serrano-Aguilar P. Calidad de vida relacionada con la salud en pacientes con esclerosis lateral amiotrófica. Neurología. 2014;29:27–35.
