






To contribute normative data for the Fototest from neurological patients with no cognitive impairment, including disaggregated data on each domain of the test (naming, free recall, total recall, and naming fluency).
Material and methodsWe performed a cross-sectional study in which neurological patients with no cognitive impairment were tested with the Fototest; we recorded total and domain scores. We performed a descriptive study of the total and domain scores, with data disaggregated by sex, age (over/under 65 years), and level of education (primary education completed/not completed; further study completed).
ResultsWe included a sample of 1055 patients, who were mainly women (57.1%), aged over 65 (60.6%), and had a low level of education (38.6% had not completed primary education). Sex, age, and level of education influence total Fototest score (34.6 ± 5.3; P10: 28; P5: 27) and free recall (8.5 ± 2.2; 6; 4), total recall (10.0 ± 1.5; 8; 7), and naming fluency scores (18.7 ± 4.9; 13; 12). For total score, the multivariate analysis revealed values of 1.5 ± 0.3 (ß ± SD) for sex (female), –2.4 ± 0.3 for age (>65), and –1.6 ± 0.4 and 3.3 ± 0.4 for incomplete primary education and completed post-primary education, respectively (completed primary study was used as a reference).
ConclusionsWe provide normative data for total and domain Fototest results for each of the groups defined according to sex, age, and level of education. We also provide a percentile distribution of scores. We hope that these normative data will translate into increases in efficiency in Fototest administration in the clinical setting.
Proporcionar valores normativos del Fototest relativos a pacientes neurológicos sin deterioro cognitivo, que incluyan datos desagregados para cada uno de los dominios que conforman este instrumento (denominación, recuerdo libre, recuerdo total y fluidez de nombres).
Material y MétodosEstudio transversal en pacientes neurológicos sin deterioro cognitivo a los que se aplicó el Fototest, registrándose las puntuaciones desagregadas y total. Estudio descriptivo de los resultados totales y desagregados del Fototest estratificados por sexo, edad (<65/>65 años) y estudios ( <primaria rimaria="" />primaria).
ResultadosMuestra de 1055 sujetos con predominio de mujeres (57.1%), mayores de 65 años (60.6%) y con bajo nivel educativo (36.8% sin tan siquiera estudios primarios). La puntuación total del Fototest (34.6 ± 5.3; 28; 27 [media ± d.e.; P10; P5]), así como las desagregadas para denominación (5.9 ± 0.3; 6; 5), recuerdo libre (8.5 ± 2.2; 6; 4), recuerdo total (10.0 ± 1.5; 8; 7) y fluidez de nombres (18.7 ± 4.9; 13; 12) están influidas por sexo, edad y nivel educativo. Para la puntuación total, los resultados del estudio multivariante son: sexo (mujer) 1.5 ± 0.3 (ß ± e.e.), edad (>65 años) −2.4 ± 0.3, estudios < Primaria −1.6 ± 0.4 y estudios > Primaria 3.3 ± 0.4 (Primaria = referencia estudios).
ConclusiónSe proporcionan valores normativos (media ± d.e, P10; P5) del Fototest para cada uno de los estratos definidos por las variables sexo, edad y estudios tanto para las puntuaciones totales como desagregadas del Fototest, así como distribución percentual para cada uno de los valores posibles de estas puntuaciones. Estos valores normativos es de esperar que se traduzcan en una mayor eficiencia del Fototest en el ámbito clínico.
The Fototest is a very brief (< 3 minutes) cognitive test suitable for illiterate individuals and not including paper and pencil tasks1; the instrument comprises 3 tasks assessing language (naming), memory (free recall [FR] and cued recall [CR]), and executive function (naming fluency [NF]).
The Fototest has been useful in detecting cognitive impairment in primary care2,3 and general neurology4 studies in Spain and abroad,5 as well as in a meta-analysis.6 The instrument has been shown to be more cost-effective than the more widely used classic instruments (Mini–Mental State Examination,7 Memory Impairment Screen8),9 newer but longer tests (eg, the Eurotest10), and other tests suitable for illiterate individuals (eg, the Memory Alteration Test11).12 It has high test-retest and inter-rater reliability,13 and 3 equivalent, parallel versions of the test are available, making it suitable for patient follow-up, particularly when the test is administered by different professionals.14
A normative study was performed for the Fototest, with data from a sample of healthy volunteers who had no subjective memory complaints; were independent in the activities of daily living; had no history of alcohol or drug abuse, neurological disease (epilepsy, brain injury, stroke, or neurodegenerative processes), or uncontrolled systemic or psychiatric disorders; and were using no drugs with potential to compromise cognition.13 There is extensive discussion around the most appropriate characteristics in a normative sample; while they are usually composed of “hypernormal” individuals (ie, healthy individuals not reporting memory loss, with no medical history or treatments that may affect cognitive performance), as in the Fototest normative study,13 normative data from such a sample should only be applied to subjects with similar sociodemographic and clinical characteristics.15 In the clinical setting in general and in neurology departments in particular, these “hypernormal” individuals are more the exception than the rule. A majority of patients will have habits, clinical history, or treatments that may affect their cognition, or consult specifically due to memory complaints. The application of normative data from selected “hypernormal” individuals may be acceptable in population studies, but it is not appropriate in the clinical setting, as diagnostic parameters derived from these data would give a biased, inflated view of the instrument’s sensitivity, with lower specificity. Following this line of reasoning, we believe that normative samples for instruments intended for use in clinical practice should be composed of individuals attended in the same clinical setting, excluding only those with cognitive impairment (ie, not patients with memory complaints or whose clinical history or treatments could potentially affect cognition).16
All studies using the Fototest consider the global score, as is typical with this type of instrument. However, it is not uncommon in practice for low scores in some domains to be concealed and compensated for by normal or high scores in others. Therefore, it is common for isolated alterations in the naming domain, often associated with specific language alterations that are apparent during administration of the test, to go unnoticed in the analysis of the global score due to better performance in other tasks. For this reason, we deem it valuable to provide normative data for each domain in the Fototest.
This study aims to provide normative data for the Fototest from a broad sample of neurology patients without cognitive impairment, as well as disaggregated data enabling identification of specific alterations in each of the instrument’s domains.
Material and methodsDesign and participantsWe performed a cross-sectional study of a heterogeneous sample of patients attended at a neurology department, explicitly verifying the absence of cognitive impairment. The sample is made up of neurology patients without cognitive impairment who were included in various studies:
Transversal study1: a cross-sectional phase II study into the diagnostic usefulness of the Fototest with a sample of patients older than 60 years attended at a general neurology department.
Fototrans study4: a multi-centre study with patients older than 60 years followed up at general neurology departments.
ETS study12: a prospective study in which consecutive patients were systematically recruited from 4 health centres over a period of one year. No age limits were applied, and patients had suspected cognitive impairment either due to subjective memory complaints or due to their carers’ or physicians’ suspicion; all patients were referred to a neurology department for testing.
Parkinson’s disease study17: prospective study to evaluate the prevalence of cognitive impairment among patients with Parkinson’s disease, including all patients attended at our hospital’s movement disorders unit in 2009.
2017 consultation data: all patients without cognitive impairment attended by one of the authors (CCP) in 2017 were systematically and prospectively included in the study.
ProcedureIn the Fototrans and Transversal studies, normal cognition was verified by the different researchers involved. In these studies, all participants reported no memory complaints and were completely independent, with normal scores on other cognitive tests (different tests were administered by different researchers: the Eurotest10 and Semantic Verbal Fluency test18 in the Transversal study, and the original7 and Spanish-language19 versions of the Mini–Mental State Examination, the Eurotest, or the Clock Drawing Test20 in the Fototrans study).
All patients in the ETS and Parkinson’s disease studies and patients consulting due to cognitive complaints in 2017 underwent a thorough neuropsychological test battery; results were normal in all cases.
The remaining patients in the 2017 dataset were considered not to have cognitive impairment if they answered “no” to the question “do you have any memory or cognitive problems?” and scored within the normal range on the Semantic Verbal Fluency test, or answered “yes” but tested normal in a more extensive cognitive battery including the Eurotest, the Clock Drawing Test (simplified version described in the Spanish-language version of the Seven Minute Screen test21), the Mini-Cog,22 and the Semantic Verbal Fluency test.
InstrumentsAll patients took the original version of the Fototest1; we recorded disaggregated data for naming, FR, total recall (TR), NF, and the global score, in addition to data on patients’ age, sex, and level of schooling.
Statistical analysisWe performed a descriptive study of Fototest results, calculating the mean (standard deviation) and distribution (percentiles). A multivariate linear regression analysis was also conducted, with Fototest results as the dependent variable and sex (male/female), age (<65/>65 years), and level of schooling (incomplete primary education/primary education/post-primary education) as independent variables.
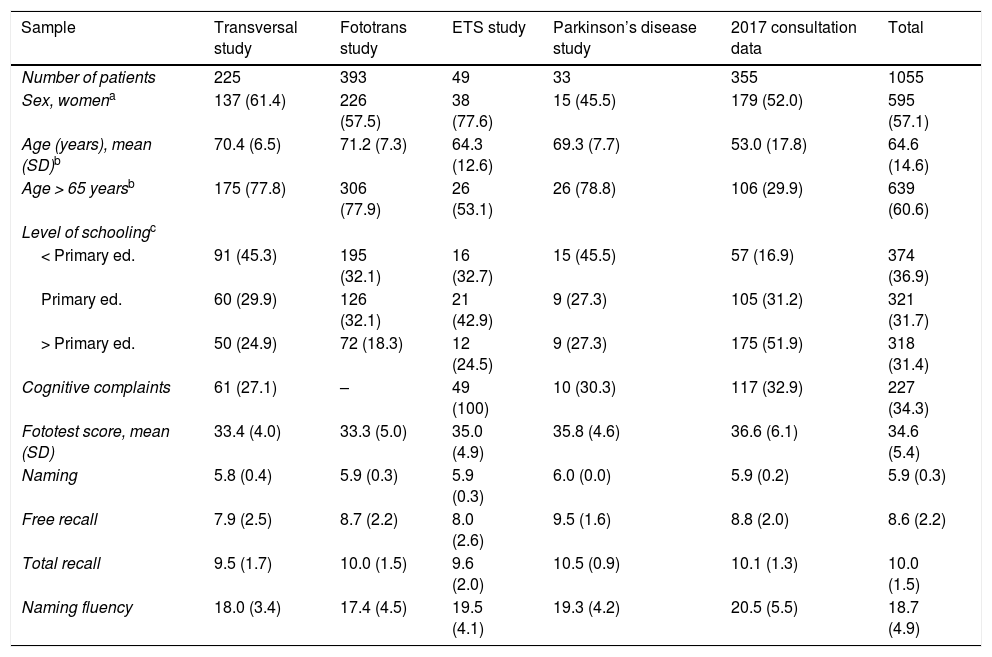
ResultsThe total sample comprised 1055 individuals. Global and disaggregated Fototest scores and sociodemographic data are presented in Table 1. Data are shown for the complete sample and the subgroups from each study. As we might expect of samples selected according to different inclusion criteria, differences were observed between groups for sex, age, and Fototest results. Overall, our sample displayed a broad age range (15 to 94 years), with most participants (60.6%) being aged over 65 years; women accounted for 57.1% of the sample. Overall, participants had a low level of schooling: 36.8% had not completed primary education, and only 31.4% had studied beyond primary level.
Sociodemographic characteristics of the sample.
| Sample | Transversal study | Fototrans study | ETS study | Parkinson’s disease study | 2017 consultation data | Total |
|---|---|---|---|---|---|---|
| Number of patients | 225 | 393 | 49 | 33 | 355 | 1055 |
| Sex, womena | 137 (61.4) | 226 (57.5) | 38 (77.6) | 15 (45.5) | 179 (52.0) | 595 (57.1) |
| Age (years), mean (SD)b | 70.4 (6.5) | 71.2 (7.3) | 64.3 (12.6) | 69.3 (7.7) | 53.0 (17.8) | 64.6 (14.6) |
| Age > 65 yearsb | 175 (77.8) | 306 (77.9) | 26 (53.1) | 26 (78.8) | 106 (29.9) | 639 (60.6) |
| Level of schoolingc | ||||||
| < Primary ed. | 91 (45.3) | 195 (32.1) | 16 (32.7) | 15 (45.5) | 57 (16.9) | 374 (36.9) |
| Primary ed. | 60 (29.9) | 126 (32.1) | 21 (42.9) | 9 (27.3) | 105 (31.2) | 321 (31.7) |
| > Primary ed. | 50 (24.9) | 72 (18.3) | 12 (24.5) | 9 (27.3) | 175 (51.9) | 318 (31.4) |
| Cognitive complaints | 61 (27.1) | – | 49 (100) | 10 (30.3) | 117 (32.9) | 227 (34.3) |
| Fototest score, mean (SD) | 33.4 (4.0) | 33.3 (5.0) | 35.0 (4.9) | 35.8 (4.6) | 36.6 (6.1) | 34.6 (5.4) |
| Naming | 5.8 (0.4) | 5.9 (0.3) | 5.9 (0.3) | 6.0 (0.0) | 5.9 (0.2) | 5.9 (0.3) |
| Free recall | 7.9 (2.5) | 8.7 (2.2) | 8.0 (2.6) | 9.5 (1.6) | 8.8 (2.0) | 8.6 (2.2) |
| Total recall | 9.5 (1.7) | 10.0 (1.5) | 9.6 (2.0) | 10.5 (0.9) | 10.1 (1.3) | 10.0 (1.5) |
| Naming fluency | 18.0 (3.4) | 17.4 (4.5) | 19.5 (4.1) | 19.3 (4.2) | 20.5 (5.5) | 18.7 (4.9) |
Data are presented as number (percentage), except where otherwise specified.
More than one-third of all patients (excluding those from the Fototrans study, which did not record this variable) had memory complaints, which were the reason for consultation in many cases (all cases in the ETS study).
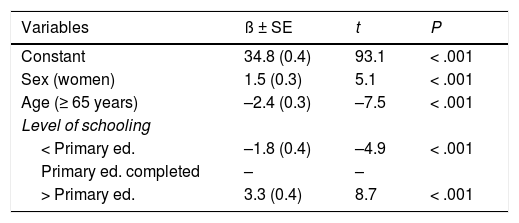
A multivariate linear regression analysis (Table 2) found that Fototest scores in this sample were influenced by sex (Fig. 1), age (Fig. 2), and level of schooling (Fig. 3).
Multivariate linear regression model.
| Variables | ß ± SE | t | P |
|---|---|---|---|
| Constant | 34.8 (0.4) | 93.1 | < .001 |
| Sex (women) | 1.5 (0.3) | 5.1 | < .001 |
| Age (≥ 65 years) | –2.4 (0.3) | –7.5 | < .001 |
| Level of schooling | |||
| < Primary ed. | –1.8 (0.4) | –4.9 | < .001 |
| Primary ed. completed | – | – | |
| > Primary ed. | 3.3 (0.4) | 8.7 | < .001 |
ß: coefficient of regression; SE: standard error; t: t statistic.
 and the mean (standard deviation).")
Violin plots showing the distribution of Fototest results by sex.
The white dots represent median scores; the ends of the black boxes represent the 25th and 75th percentiles; and the length of the line is 1.5 times the interquartile range; the violin shape represents the density distribution of the data, extending to the highest and lowest values. The values inside the violin indicate the number of individuals (N) and the mean (standard deviation).

 and the mean (standard deviation).")
Violin plots showing the distribution of Fototest scores by level of schooling.
The white dots represent median scores; the ends of the black boxes represent the 25th and 75th percentiles; and the length of the line is 1.5 times the interquartile range; the violin shape represents the density distribution of the data, extending to the highest and lowest values. The values inside the violin indicate the number of individuals (N) and the mean (standard deviation).
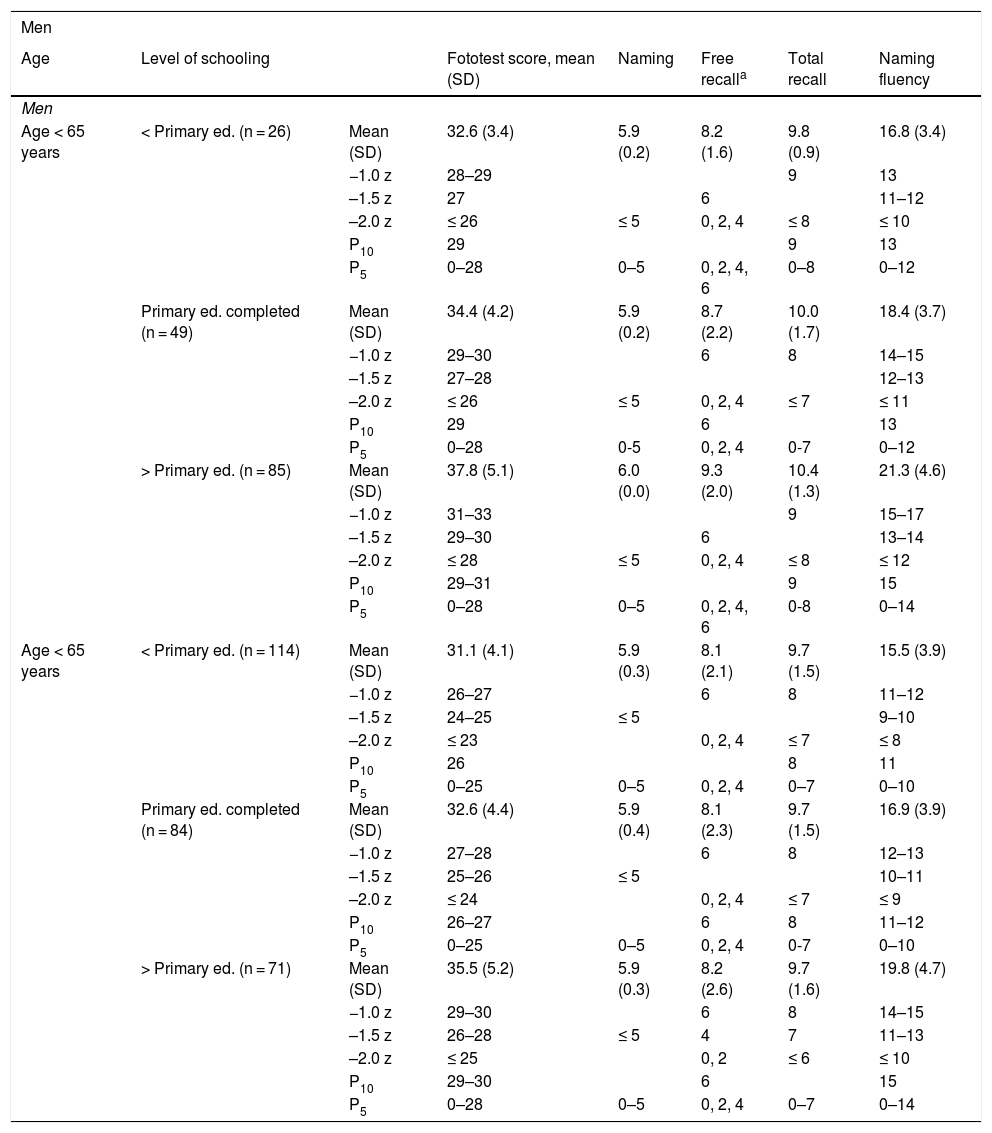
Table 3 summarises the normative data for global and domain scores, stratified by sex (male/female), age (<65/>65 years), and level of schooling (incomplete primary education/primary education/post-primary education), including the z-scores and percentiles of greatest diagnostic interest. Supplementary Tables S1 to S12 present detailed data on the percentile distribution of each stratum, for both global and domain scores.
Normative data for global and domain Fototest scores, stratified by sex, age, and level of schooling.
| Men | |||||||
|---|---|---|---|---|---|---|---|
| Age | Level of schooling | Fototest score, mean (SD) | Naming | Free recalla | Total recall | Naming fluency | |
| Men | |||||||
| Age < 65 years | < Primary ed. (n = 26) | Mean (SD) | 32.6 (3.4) | 5.9 (0.2) | 8.2 (1.6) | 9.8 (0.9) | 16.8 (3.4) |
| −1.0 z | 28–29 | 9 | 13 | ||||
| –1.5 z | 27 | 6 | 11–12 | ||||
| –2.0 z | ≤ 26 | ≤ 5 | 0, 2, 4 | ≤ 8 | ≤ 10 | ||
| P10 | 29 | 9 | 13 | ||||
| P5 | 0–28 | 0–5 | 0, 2, 4, 6 | 0–8 | 0–12 | ||
| Primary ed. completed (n = 49) | Mean (SD) | 34.4 (4.2) | 5.9 (0.2) | 8.7 (2.2) | 10.0 (1.7) | 18.4 (3.7) | |
| −1.0 z | 29–30 | 6 | 8 | 14–15 | |||
| –1.5 z | 27–28 | 12–13 | |||||
| –2.0 z | ≤ 26 | ≤ 5 | 0, 2, 4 | ≤ 7 | ≤ 11 | ||
| P10 | 29 | 6 | 13 | ||||
| P5 | 0–28 | 0-5 | 0, 2, 4 | 0-7 | 0–12 | ||
| > Primary ed. (n = 85) | Mean (SD) | 37.8 (5.1) | 6.0 (0.0) | 9.3 (2.0) | 10.4 (1.3) | 21.3 (4.6) | |
| −1.0 z | 31–33 | 9 | 15–17 | ||||
| –1.5 z | 29–30 | 6 | 13–14 | ||||
| –2.0 z | ≤ 28 | ≤ 5 | 0, 2, 4 | ≤ 8 | ≤ 12 | ||
| P10 | 29–31 | 9 | 15 | ||||
| P5 | 0–28 | 0–5 | 0, 2, 4, 6 | 0-8 | 0–14 | ||
| Age < 65 years | < Primary ed. (n = 114) | Mean (SD) | 31.1 (4.1) | 5.9 (0.3) | 8.1 (2.1) | 9.7 (1.5) | 15.5 (3.9) |
| −1.0 z | 26–27 | 6 | 8 | 11–12 | |||
| –1.5 z | 24–25 | ≤ 5 | 9–10 | ||||
| –2.0 z | ≤ 23 | 0, 2, 4 | ≤ 7 | ≤ 8 | |||
| P10 | 26 | 8 | 11 | ||||
| P5 | 0–25 | 0–5 | 0, 2, 4 | 0–7 | 0–10 | ||
| Primary ed. completed (n = 84) | Mean (SD) | 32.6 (4.4) | 5.9 (0.4) | 8.1 (2.3) | 9.7 (1.5) | 16.9 (3.9) | |
| −1.0 z | 27–28 | 6 | 8 | 12–13 | |||
| –1.5 z | 25–26 | ≤ 5 | 10–11 | ||||
| –2.0 z | ≤ 24 | 0, 2, 4 | ≤ 7 | ≤ 9 | |||
| P10 | 26–27 | 6 | 8 | 11–12 | |||
| P5 | 0–25 | 0–5 | 0, 2, 4 | 0-7 | 0–10 | ||
| > Primary ed. (n = 71) | Mean (SD) | 35.5 (5.2) | 5.9 (0.3) | 8.2 (2.6) | 9.7 (1.6) | 19.8 (4.7) | |
| −1.0 z | 29–30 | 6 | 8 | 14–15 | |||
| –1.5 z | 26–28 | ≤ 5 | 4 | 7 | 11–13 | ||
| –2.0 z | ≤ 25 | 0, 2 | ≤ 6 | ≤ 10 | |||
| P10 | 29–30 | 6 | 15 | ||||
| P5 | 0–28 | 0–5 | 0, 2, 4 | 0–7 | 0–14 | ||
| Women | |||||||
|---|---|---|---|---|---|---|---|
| Age | Level of schooling | Fototest score, mean (SD) | Naming | Free recall | Total recall | Naming fluency | |
| Age < 65 years | < Primary ed. (n = 54) | Mean (SD) | 33.2 (4.0) | 5.8 (0.4) | 8.9 (1.9) | 10.2 (1.3) | 17.2 (3.2) |
| −1.0 z | 28–29 | 9 | 13–14 | ||||
| –1.5 z | 26–27 | 6 | 12 | ||||
| –2.0 z | ≤ 25 | ≤ 5 | 0, 2, 4 | ≤ 8 | ≤ 11 | ||
| P10 | 28–29 | 0-12 | |||||
| P5 | 0–27 | 0–5 | 0, 2, 4, 6 | 0–8 | 13–14 | ||
| Primary ed. completed (n = 77) | Mean (SD) | 36.4 (5.2) | 5.9 (0.3) | 9.0 (2.0) | 10.3 (1.3) | 20.3 (4.6) | |
| −1.0 z | 30–31 | 9 | 14–16 | ||||
| –1.5 z | 27–29 | ≤ 5 | 6 | ≤ 8 | 12–13 | ||
| –2.0 z | ≤ 26 | 0, 2, 4 | ≤ 11 | ||||
| P10 | 30–31 | 9 | 15 | ||||
| P5 | 0–29 | 0–5 | 0, 2, 4, 6 | 0–8 | 0–14 | ||
| > Primary ed. (n = 97) | Mean (SD) | 40.8 (5.6) | 5.9 (0.1) | 9.4 (1.9) | 10.4 (1.3) | 24.4 (5.2) | |
| −1.0 z | 33–35 | 9 | 18–19 | ||||
| −1.5 z | 31–32 | 6 | ≤ 8 | 15–17 | |||
| −2.0 z | ≤ 30 | ≤ 5 | ≤ 14 | ||||
| P10 | 35 | 9 | 18 | ||||
| P5 | 0–34 | 0–5 | 0, 2, 4, 6 | 0–8 | 0–17 | ||
| Age < 65 years | < Primary ed. (n = 178) | Mean (SD) | 32.3 (4.4) | 5.8 (0.4) | 8.2 (2.4) | 9.7 (1.8) | 16.8 (3.8) |
| −1.0 z | 27–28 | 6 | 8 | 12–13 | |||
| –1.5 z | 25–26 | 7 | 10–11 | ||||
| –2.0 z | ≤ 24 | ≤ 5 | 0, 2, 4 | ≤ 6 | ≤ 9 | ||
| P10 | 26 | 6 | 7 | 11–12 | |||
| P5 | 0–25 | 0–5 | 0, 2, 4 | 0–6 | 0–10 | ||
| Primary ed. completed (n = 105) | Mean (SD) | 33.9 (3.9) | 5.8 (0.4) | 8.3 (2.1) | 9.8 (1.5) | 18.2 (3.4) | |
| −1.0 z | 29–30 | 6 | 8 | 14–15 | |||
| –1.5 z | 27–28 | 11–13 | |||||
| –2.0 z | ≤ 26 | ≤ 5 | 0, 2, 4 | ≤ 7 | ≤ 10 | ||
| P10 | 28-29 | 7 | 14–15 | ||||
| P5 | 0–27 | 0–5 | 0, 2, 4 | 0–6 | 0–13 | ||
| > Primary ed. (n = 61) | Mean (SD) | 36.0 (5.1) | 5.9 (0.3) | 8.7 (2.5) | 9.9 (1.7) | 20.2 (4.8) | |
| −1.0 z | 29–31 | 6 | 8 | 14–15 | |||
| –1.5 z | 27–28 | 7 | 12–13 | ||||
| –2.0 z | ≤ 26 | ≤ 5 | 0, 2, 4 | ≤ 6 | ≤ 11 | ||
| P10 | 30 | 7–8 | 13–14 | ||||
| P5 | 0–29 | 0–5 | 0, 2, 4 | 0–6 | 0–12 |
We present normative data for global and domain (naming, FR, TR, and NF) Fototest scores from a broad sample of neurology patients without cognitive impairment. CR scores are not included as they were of no diagnostic interest: low values may be observed both in patients with excellent recall (perfect FR) and in those with severe memory impairment. Also due to a lack of diagnostic value, NF scores for naming women and for naming men are not differentiated, since no significant difference was detected between the scores or distributions of these variables, as was the case in the previous normative study. Therefore, the NF values shown are the sums of scores for naming men and naming women.
These normative data are more appropriate for use in the clinical setting (particularly in neurology departments, but also in other specialties and primary care), especially when assessing individuals with memory complaints. In clinical use, specificity should take precedence over sensitivity. The use of “hypernormal” individuals for brief cognitive tests may inflate sensitivity values, leading to an increased false positive rate and consequently to unnecessary complementary studies, with a negative effect on the instrument’s efficiency.
We also offer disaggregated normative data for the various domains of the Fototest, as our experience has shown that poor performance in one domain can often be overlooked due to compensation by better performance in other domains. We therefore recommend recording both global and domain Fototest scores, as follows: total (naming, FR + CR, NF). This would allow for different profiles to be identified and modelled, which may inform studies aiming to determine aetiology. For example, a global score of 25 may be interpreted in different ways according to domain scores: 25 (6, 0 + 1, 18) clearly suggests a memory problem that is not substantially improved with cueing, whereas 25 (6, 6 + 2, 11) suggests an alteration affecting executive function; finally, 25 (3, 6 + 3, 13) suggests an alteration mainly affecting naming, indicating agnosia or naming impairment as the cause.
One strength of our study is its large sample size and the naturalistic, pragmatic sampling method used; however, we must also acknowledge certain limitations. While the use of samples from different studies may be considered a weakness, the fact that all samples were drawn from clinical practice results in a naturalistic total sample and therefore in greater external validity.
The main weakness is the study’s cross-sectional methodology, with a single measurement taken from each participant; this prevents us from ruling out the possibility that some participants may have been in an incipient phase of cognitive impairment. This risk is particularly apparent in our sample, which includes patients whose circumstances (medical history, treatments, etc) suggest a clear risk of cognitive impairment, particularly those with subjective cognitive complaints that may be compatible with the new concept of subjective cognitive decline.23 In many cases, this may reflect a very early phase of Alzheimer disease or some other neurodegenerative process, rather than being a risk factor.24 We aimed to compensate for this weakness by conducting a more thorough, detailed examination of patients with cognitive complaints, with a formal cognitive assessment in most cases. Nonetheless, we agree with other authors that establishing “consistent” norms, reliably excluding individuals who subsequently develop cognitive impairment,25 is possible only by conducting repeated assessments over time.26 We deem this costly methodology not to be justified for a brief cognitive test with notable limitations in terms of diagnosis and applicability.27 Despite their usefulness and adaptability for multiple functions (screening, follow-up, classification, etc), these tests should never be used for diagnosis. No brief cognitive test used in Spain uses this type of norms, not even the Mini–Mental State Examination (the longest and most widely used, despite its limitations)28 or the NEURONORMA project,29 an essential reference for normative studies in our setting.
The normative data presented here will lead to better use and greater diagnostic usefulness of the Fototest. We should emphasise that the results obtained in this or any other brief cognitive test should never take the place of clinical judgement, but rather should support or reinforce it.27
Conflicts of interestC. Carnero-Pardo is the author of the Fototest and Eurotest. The remaining authors have no conflicts of interest to declare.
The Fototest and Eurotest are subject to a Creative Commons licence.
The following are Supplementary data to this article:
Please cite this article as: Carnero Pardo C, Carrera Muñoz I, Triguero Cueva L, López Alcalde S, Vílchez Carrillo R. Valores normativos del Fototest en pacientes neurológicos sin deterioro cognitivo. Neurología. 2022;37:45–52.
