



Methanol poisoning is a severe condition that leads to acute metabolic acidosis, neurological alterations, blindness, and even death. Methanol is not a toxic substance in itself; toxicity occurs when it is metabolised to formic acid, whose accumulation in the body causes the above-mentioned symptoms.1
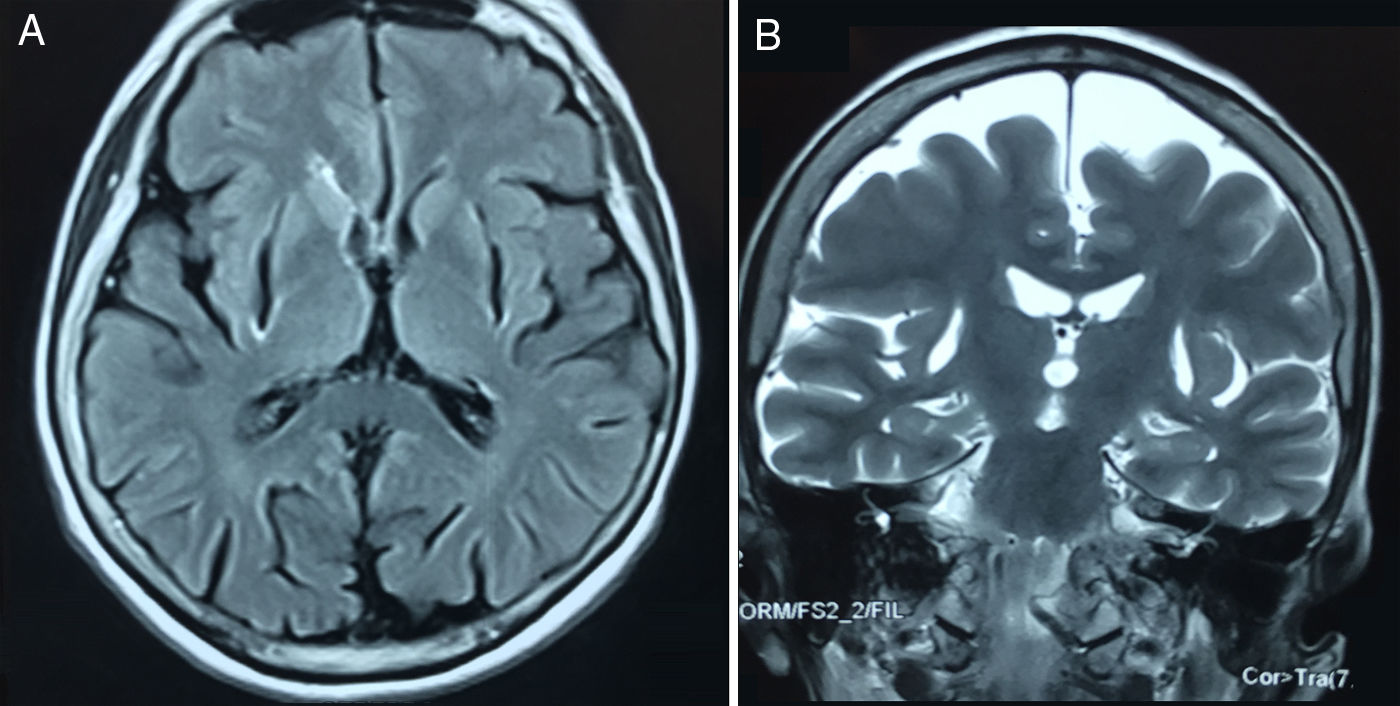
We present the case of a 66-year-old Hispanic patient who visited the neurology clinic due to a 25-year history of postural instability, limited upper limb movement, and dysphonia with no dysphagia or tremor. Physical examination revealed vision loss with no changes in eye movements, bradykinesia, left laterocollis, and upper limb stiffness with no tremor. She also reported previous treatment with amantadine and levodopa/carbidopa, which did not improve her symptoms. A magnetic resonance imaging (MRI) scan showed bilateral lesions in the putamina (Fig. 1). In view of this finding, the patient was interviewed again and described an episode of alcohol intoxication at the age of 22, which caused her vision loss. The poisoning was caused by methanol, a common substance in adulterated alcoholic drinks.
 and coronal T2-weighted (B) MRI sequences showing bilateral absence of the putamina.")
The mechanisms by which methanol causes neurological damage are not fully understood, but formic acid, methanol's toxic metabolite, is believed to be responsible. Formic acid metabolism is very slow, causing it to accumulate in the body, generating a severe metabolic acidosis with an increased osmolar gap.2
The neuropathy and subsequent vision loss secondary to methanol intake are caused by the interruption of the mitochondrial function in cells of the optic nerve, leading to hyperaemia, oedema, and atrophy over a period of 12-24hours after consumption. Damage affects the retrolaminar portion of the optic nerve; minimal or no damage to the retina is observed.3
The literature includes few reports of parkinsonism as a long-term consequence of methanol poisoning, due to infarction and subsequent necrosis of the putamen. Formic acid has classically been identified as a mitochondrial toxin which can alter cytochrome c oxidase function, leading to ATP depletion. Another theory suggests that formic acid causes damage by intervening in dopaminergic pathways and increasing dopamine-B-hydroxylase activity.4 However, there is no clear explanation of why formic acid particularly affects the retina, the optic nerve, and the basal ganglia (putamen) but not other areas of the brain. It has been suggested that excessive accumulation of formic acid may be the cause of the damage; this may be explained by expression of aquaporins, especially aquaporin 1, 3, and 4, which are essential for osmotic and water balance of cells in the brain and the optic nerve.5 These cells are responsible for transporting not only water, but also polar molecules such as glycerol or methanol to these tissues.
The patient gave written informed consent for the publication of the case and the corresponding images.
FundingThis study has not received funding from any source.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank Dr Helen Reina for her assistance with the manuscript.
Please cite this article as: Enriquez-Marulanda A, Ospina-Delgado D, Arias-Mora F, Amaya-González P, Orozco JL. Paciente con parkinsonismo y un antecedente de intoxicación por metanol. Neurología. 2019;34:555–556.
