



I wish to respond to the remarks made by Olazarán and Bermejo1 in reference to the article ‘Should the Mini-Mental State Examination be retired?’.2 I must acknowledge that my arguments are based not only on my particular clinical experience (characterised by lack of time and a population with a low educational level) but also on other personal circumstances such as the fact that I created other short cognitive tests that may be considered alternatives to the Mini-Mental State Examination (MMSE), as I clearly stated in my article.2 Regardless of these circumstances and their potential influence on my argument, I am convinced that there are a number of objective reasons to suggest that the MMSE be retired. This, however, should not be considered an insult, but rather a desirable circumstance which can only be achieved after a tool has been used extensively and made a significant contribution to medicine, as I emphasised in my article.
The fact that the MMSE has several versions and nearly 30000 hits in PubMed does not necessarily make it a good standard. A good standard (for example, the INR for coagulation) provides stable, reliable, valid, and universal results, and this is not precisely the case with the MMSE.
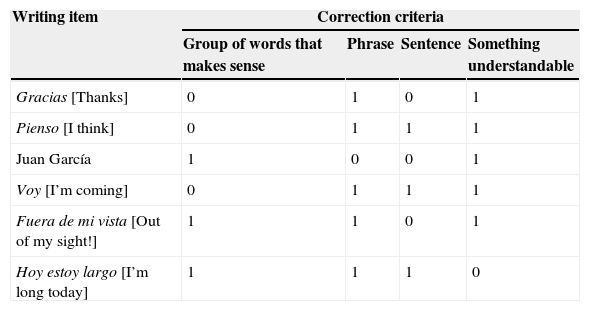
What then does it mean to score 22 on the MMSE? That depends. Not only on patients’ characteristics (age, sex, educational level, etc.) and the version and items used, but also, and this is serious, on the evaluator. Let us take, for example, the ‘writing’ item in the Spanish version of the MMSE published by TEA Ediciones, which asks the patient to ‘write a phrase that makes sense’. The wording is apparently clear and easy to understand (according to the Royal Academy of the Spanish Language, a phrase [frase] is a group of words that is sufficient to communicate meaning). The task, however, becomes more ambiguous and open to various interpretations when we read the instructions for assessment, stating that the phrase must contain a subject and a verb in addition to making sense. The problem arises because ‘phrases’ do not necessarily contain these elements, which are required in ‘sentences’. As a consequence, the evaluator may not know what exactly is being asked for in this item: a ‘phrase’, a ‘sentence’, ‘a group of words that makes sense’, or ‘something understandable’: these are completely different concepts. Table 1 shows some examples of responses and the assessment according to the criterion followed by the evaluator; all of these examples are at least partially compatible with the instructions for evaluating the item. But this is not the only ambiguous item. The patient is also asked to provide the state in which he/she is located, but the concept of ‘state’ may be subjective for some patients and evaluators, and even be influenced by where the assessment takes place. The political situation in Spain, for example, may result in a number of responses, which may in turn be regarded as correct or incorrect depending on the evaluator and the region where the interview is conducted. These are 2 examples of items whose responses may be regarded as either correct or incorrect depending on the evaluator's perspective. This factor, along with the variability tolerated for some items, the lack of a standardised administration procedure, and inconsistencies in the administration of certain tasks, result in poor reliability, and we must face that there can be no validity without reliability.
Examples of responses to the writing item on the MMSE, corrected according to different criteria.
| Writing item | Correction criteria | |||
|---|---|---|---|---|
| Group of words that makes sense | Phrase | Sentence | Something understandable | |
| Gracias [Thanks] | 0 | 1 | 0 | 1 |
| Pienso [I think] | 0 | 1 | 1 | 1 |
| Juan García | 1 | 0 | 0 | 1 |
| Voy [I’m coming] | 0 | 1 | 1 | 1 |
| Fuera de mi vista [Out of my sight!] | 1 | 1 | 0 | 1 |
| Hoy estoy largo [I’m long today] | 1 | 1 | 1 | 0 |
While it is true that we have found good results of the MMSE in a cohort with a high percentage of illiterate individuals,3 these results were obtained after a reanalysis of data from 2 previous independent studies in which we applied a different cut-off point from the usually recommended one and did not correct scores for age and educational level. When the recommended cut-off points were applied in these 2 original studies, results were not as good.4,5 Researchers should not have to wait for results from a large sample in order to determine the optimal cut-off point. Using a different version for each situation (illiterate subjects, etc.) is not practical; likewise, modifying or correcting items according to each subject's particularities or the location where the assessment takes place is hardly ideal. In daily practice, healthcare professionals need a tool that can be applied to all subjects and circumstances, regardless of their personal characteristics, with clear, concrete, and precise administration instructions. The MMSE does not meet these requirements.
Comparing the results of the usefulness of several tools using data from different studies, as do the authors of this letter, is methodologically incorrect in addition to misleading. Even if the MMSE, with the new cut-off points that we propose, were to show similar efficacy and effectiveness to the Mini-Cog, MIS, and Fototest, the latter tools can be applied in 2-3minutes, which is considerably shorter than the time required to administer the MMSE. This results in lower costs and increased efficiency. The study comparing the effectiveness of Fototest, MMSE, and MIS5 used the cut-off points recommended at that time. If we had applied the cut-off points that we would later recommend,3 the MMSE would have shown itself more effective while still being the most costly and least efficient tool of all. This study was conducted under conditions providing the highest level of scientific evidence according to the principles of evidence-based medicine.6
The fact that there are no claims of inappropriate use of the MMSE does not prove or guarantee that the rights of the copyright holders are being protected. The restrictions for use of the Spanish-language version of the MMSE strictly prohibit full or partial reproduction of the questionnaire in any form or by any means, and regardless of where it will be used; these restrictions are even stricter in the United States. The authors of this letter seem to suggest that it is tolerable to view illegal copies of films at home and that this practice should only be limited when the films will be shown for profit.
Regardless of the personal circumstances which have inevitably influenced my argument, I feel that there are scientific, pragmatic, economic, and legal reasons to grant the MMSE an honourable retirement in light of its nearly 40 years of dedicated service. I can only cite sentimental reasons for continuing to recommend this questionnaire.
Conflicts of interestC. Carnero-Pardo is the author of Fototest and Eurotest.
Please cite this article as: Carnero-Pardo C. Las razones para jubilar al Mini-Mental. Neurología. 2015;30:588–589.
