


To assess how the diet cost is associated with socio-demographic factors and adherence to Mediterranean diet in children.
MethodsData were obtained from a community-based survey of children selected from public elementary schools in Portugal. Of a total of 586 children attending these schools, 464 (6–12 years), were studied. Dietary intake was assessed by a 24hour recall and the adherence to Mediterranean diet was evaluated through the KIDMED index. The cost of the diet was calculated based on the collection of food prices of a national leader supermarket, and expressed as Total Daily Cost (TDC) and Total Daily Cost-Adjusted for Energy (TDEC). Anthropometric measures were taken and socio-demographic data were gathered from a questionnaire filled by parents. Logistic regression was used to quantify the association between diet cost, socio-demographics and adherence to Mediterranean diet.
ResultsThe average TDC was 4.58€ (SD=1.24). Most children (69.1%) reported medium adherence to Mediterranean diet, and 4.6% rated the higher score. TDC was higher for children with highest adherence to Mediterranean diet, compared to those with lowest adherence [TDC: OR=5.70 (95% CI 1.53, 21.33), p for trend=0.001; TDEC: OR=2.83 (95% CI 0.89, 8.96, p for trend 0.018)]. No meaningful variation in the diet cost with age and parental education was observed.
ConclusionHigher adherence to Mediterranean diet was associated with higher diet cost in children.
The Mediterranean Diet has been object of study since the 1950s1 and is nowadays recognized for its numerous health benefits, namely protection against weight gain, obesity and diabetes mellitus type 2, cardiovascular diseases, certain tumors and other oxidative stress-related diseases.2,3
However, its original defining-characteristics do not fully correspond to the diet practiced nowadays among populations living in the Mediterranean region.4 This dietary pattern was firstly characterized by a high consumption of fruits, vegetables and grains; moderate consumption of dairy products and wine and low consumption (and amount) of red meat. Olive oil would be the main source of dietary lipids.1 Regrettably, this dietary pattern is being replaced by unhealthier choices,5,6 similarly to what is happening around the world. A low consumption of fruits and vegetables7 parallel to a growing consumption of high-density energy foods – such as snacks, sugar-rich food, fast food and soft drinks – is well documented and associated with lifestyle changes.8 These dietary modifications contribute to poorer diet quality and have been indicted as a significant explanation for the rising obesity rates, specially concerning in children.8 The same phenomenon has been also documented in Portugal.9
Changes in the physical environment and food supply have been pointed recently as major causes of the Obesity epidemic,10 which is becoming to be perceived from an economic perspective. In fact, substantial research on diet cost has been performed in recent years, in the U.S.A. and some European countries. The results consistently show that the cost of food is a primary determinant of food choice11,12 and that higher energy density foods, which are less nutrient-rich, are associated with lower prices. On the other hand, low-energy-dense foods such as fruits and vegetables appear to be more expensive.11,13,14 In this context, healthier diets are associated with higher costs.14–17
Taking into account the benefits of the Mediterranean diet, its health promoter potential, as well as the importance of price as food choice determinant, we aimed to estimate the cost of children's diet according to the degree of adherence to Mediterranean diet. To the best of our knowledge, this is one of the first European studies on this topic in children, which may provide new information to health professionals and policy makers so they can better educate and act toward the availability of healthy eating at low cost to the common citizen. The objectives of this study were to estimate the daily cost of diet and to quantify its association with socio-demographic factors and the degree of adherence to the Mediterranean diet in children.
MethodsParticipantsThe data were derived from a community-based survey of children selected from 7 of the eighty public elementary schools in the city of Guimarães, Portugal, between October 2007 and March 2008. Letters were distributed to all parents or guardians outlining the aims of the study along with a consent form. From the total of 586 children attending these schools, 464 (225 boys and 239 girls) between 6 and 12 years accepted to participate in the study. Anthropometric measurements and dietary data were collected from all consenting children and questionnaires surveying sociodemographics and lifestyle information were distributed among parents or educational guardians, of which 405 have answered (87%).
The study was approved by the University of Porto Ethics Committee, the schools where the study was carried out and the Portuguese Data Protection Authority (CNPD-Comissão Nacional de Protecção de Dados, process number 7613/2008).
AssessmentsHeight and weight were measured by previously trained health professionals or students, following international standardized procedures.18,19 Children wore light indoor clothing and were barefooted. Weight was measured in an electronic scale, with an error of ±100g (Seca®, Model 703, Germany), and height was measured using a stadiometer, with the head in the Frankfort plane. BMI was calculated as weight (kg)/height2 (m)20 and children's weight status was categorized using the IOTF criteria and cut-points for BMI, defined specifically for sex and age.21 Only three categories were considered in analysis of results: normal, overweight and obesity.
Dietary intake information was assessed by a 24hour recall, in which children were asked to recall all food and beverages consumed in the previous 24h. A photographic manual of portion sizes and household measures (Manual of Food Quantification) was used22 as an auxiliary tool to estimate sizes of foods and beverages consumed.
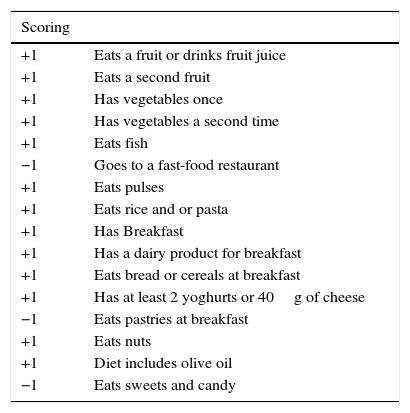
KIDMED index5 was applied to verify the adherence level to the Mediterranean diet. This index was created according to the Mediterranean diet principles and provides a score ranging from 0 to 12 according 16 questions. Questions denoting a negative connotation with respect to the Mediterranean diet were assigned a value of −1 and those with a positive aspect, +1. This score was applied according to the food consumption in the previous 24h, as described in Table 1. In accordance with the sum obtained, 3 classes were created: >8, high adherence to the Mediterranean diet; 4–7, medium adherence to the Mediterranean diet and ≤3, low adherence to the Mediterranean diet (Table 1).
Kidmed index used to access the adherence to the Mediterranean diet.
| Scoring | |
|---|---|
| +1 | Eats a fruit or drinks fruit juice |
| +1 | Eats a second fruit |
| +1 | Has vegetables once |
| +1 | Has vegetables a second time |
| +1 | Eats fish |
| −1 | Goes to a fast-food restaurant |
| +1 | Eats pulses |
| +1 | Eats rice and or pasta |
| +1 | Has Breakfast |
| +1 | Has a dairy product for breakfast |
| +1 | Eats bread or cereals at breakfast |
| +1 | Has at least 2 yoghurts or 40g of cheese |
| −1 | Eats pastries at breakfast |
| +1 | Eats nuts |
| +1 | Diet includes olive oil |
| −1 | Eats sweets and candy |
The socioeconomic information and family characteristics were collected from the survey distributed to the parents or educational guardians. It contained questions about gender and age of children and parents’ education, recorded in five categories of years: 0, 1–4, 5–9, 10–12, and more than 12 years of formal education. This information was further grouped for analysis into four categories: up to 5 years, between 5 and 9 years, 10–12 years and more than 12 years of education.
Estimation of diet costThe estimation of diet cost was divided in two tasks. Firstly, the collection of food prices, that took place between March and April of 2011. The source was an online supermarket, belonging to a Portuguese leader supermarket chain. Price data was obtained by gathering mean prices of correspondent food or package size, as well as the price per kilogram. Measurements were taken on regular prices, excluding discounts. In the case of composed dishes, diet costs were calculated using recipes available in Food Processor Plus® database (most of them previously adapted from traditional Portuguese recipes) and from a Portuguese website of traditional recipes.23 The price of the drinking water was estimated by the median price of the bottled natural mineral water and of the municipal water.
After this procedure, food items were assigned into different groups according to the staple food that was in its origin, and the median price per gram was computed. For example, the price of rice was obtained by calculating the median of the prices of the various brands and types available in the supermarket webpage. The choice for using the median rather than the average price was based on the fact that it better represents the central values, minimizing the effect of the very high and very low prices for each group. Finally, the cost of each meal was calculated according to the contribution of each and every food ingredient taking into account its proportion.
At dietary level, two variables were created: “Total daily cost” (TDC), representing the cost of each individual's diet and obtained by summing the cost of each meal, and “Total daily cost adjusted for energy” (TDEC) which eliminated the possible differences in costs associated with different energetic intake between individuals. TDEC was computed dividing TDC by the energy consumed (€/kcal) and expressed as €/1000kcal, in order to point differences not seen with TDC.
Statistical analysisThe statistical analyses were performed using the software Statistical Package for the Social Sciences (SPSS), version 17.0. Descriptive statistics were used to characterize the sample (mean and standard deviations). A total of 342 subjects for whom assessment of overall dietary intake was available were considered for data analysis.
Unconditional binary logistic regression models were fitted to estimate the magnitude of the association between diet cost (considering two categories, using the median value as the cut-off) and socio-demographic characteristics (sex, age and parents education) and the degree of adherence to the Mediterranean Diet (Kidmed score).5 The level of significance was set at 0.05.
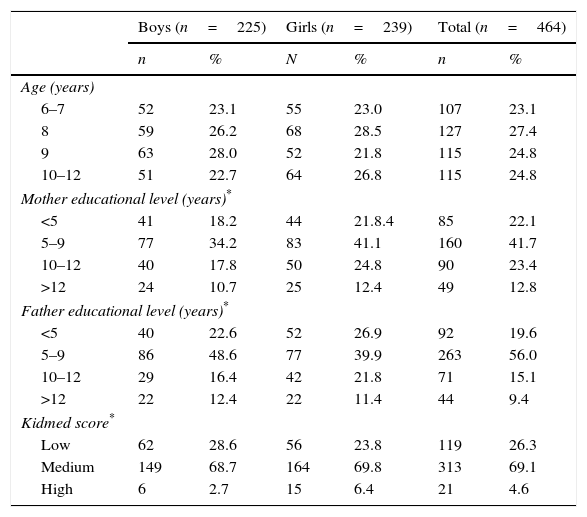
ResultsParticipant characterizationIn this sample of 464 children (51.5% girls), the prevalence of overweight and obesity were 23.3% and 7.3%, respectively. Approximately two-thirds of the study population had parents with less than 10 years of formal education. The majority of children reported a medium adherence level to Mediterranean diet (69.1%), and only 4.6% rated a higher adherence score (Table 2).
Participants’ characteristics.
| Boys (n=225) | Girls (n=239) | Total (n=464) | ||||
|---|---|---|---|---|---|---|
| n | % | N | % | n | % | |
| Age (years) | ||||||
| 6–7 | 52 | 23.1 | 55 | 23.0 | 107 | 23.1 |
| 8 | 59 | 26.2 | 68 | 28.5 | 127 | 27.4 |
| 9 | 63 | 28.0 | 52 | 21.8 | 115 | 24.8 |
| 10–12 | 51 | 22.7 | 64 | 26.8 | 115 | 24.8 |
| Mother educational level (years)* | ||||||
| <5 | 41 | 18.2 | 44 | 21.8.4 | 85 | 22.1 |
| 5–9 | 77 | 34.2 | 83 | 41.1 | 160 | 41.7 |
| 10–12 | 40 | 17.8 | 50 | 24.8 | 90 | 23.4 |
| >12 | 24 | 10.7 | 25 | 12.4 | 49 | 12.8 |
| Father educational level (years)* | ||||||
| <5 | 40 | 22.6 | 52 | 26.9 | 92 | 19.6 |
| 5–9 | 86 | 48.6 | 77 | 39.9 | 263 | 56.0 |
| 10–12 | 29 | 16.4 | 42 | 21.8 | 71 | 15.1 |
| >12 | 22 | 12.4 | 22 | 11.4 | 44 | 9.4 |
| Kidmed score* | ||||||
| Low | 62 | 28.6 | 56 | 23.8 | 119 | 26.3 |
| Medium | 149 | 68.7 | 164 | 69.8 | 313 | 69.1 |
| High | 6 | 2.7 | 15 | 6.4 | 21 | 4.6 |
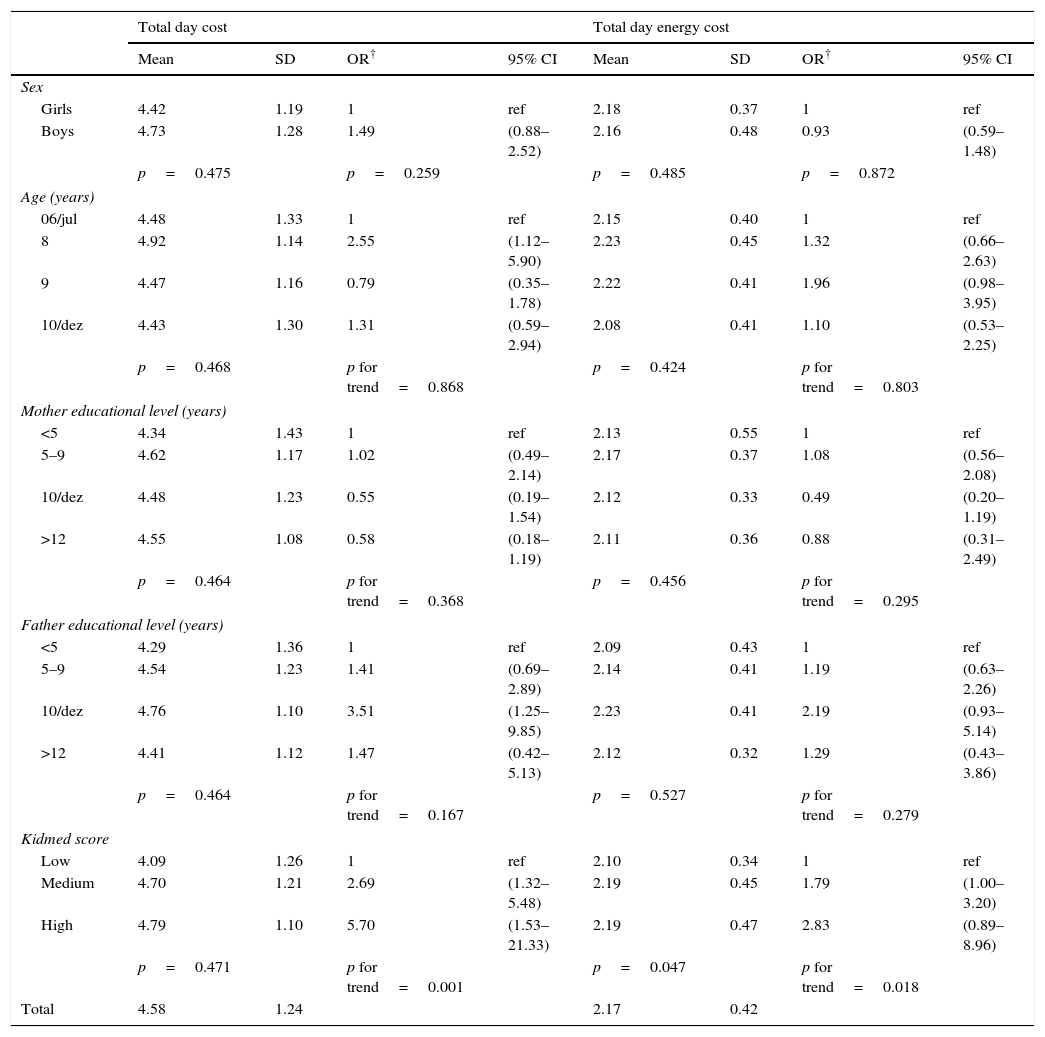
The average (±standard deviation) TDC was 4.58 (±1.24) € and the average TDEC was 2.17 (±0.42) €/1000kcal (Table 3). No meaningful differences were observed between gender, age or parental education regarding TDC and TDEC. Accordingly, no meaningful or consistent variation in the diet cost with age and parents’ education was observed (Table 3). Concerning Kidmed score, it is noticeable an increasing in the cost of the diet with increasing level of adherence to the Mediterranean Diet (TDC of 4.79€ in high adherence category vs. 4.09€ in low adherence category, p=0.471; TDEC of 2.19€/1000kcal in high adherence category vs. 2.10€/1000kcal in low adherence category, p=0.047). Considering children reporting the higher adherence to Mediterranean diet in comparison with those with the lowest adherence, the odds favoring higher diet cost was 5.70 (95% CI 1.53–21.33, p for trend=0.001) for TDC and 2.83 (95% CI 0.89–8.96, p for trend=0.018) for TDEC (Table 3).
Diet cost and odds ratio for diet cost according to sex, age, weight status, parents’ education and Kidmed score.
| Total day cost | Total day energy cost | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | OR† | 95% CI | Mean | SD | OR† | 95% CI | |
| Sex | ||||||||
| Girls | 4.42 | 1.19 | 1 | ref | 2.18 | 0.37 | 1 | ref |
| Boys | 4.73 | 1.28 | 1.49 | (0.88–2.52) | 2.16 | 0.48 | 0.93 | (0.59–1.48) |
| p=0.475 | p=0.259 | p=0.485 | p=0.872 | |||||
| Age (years) | ||||||||
| 06/jul | 4.48 | 1.33 | 1 | ref | 2.15 | 0.40 | 1 | ref |
| 8 | 4.92 | 1.14 | 2.55 | (1.12–5.90) | 2.23 | 0.45 | 1.32 | (0.66–2.63) |
| 9 | 4.47 | 1.16 | 0.79 | (0.35–1.78) | 2.22 | 0.41 | 1.96 | (0.98–3.95) |
| 10/dez | 4.43 | 1.30 | 1.31 | (0.59–2.94) | 2.08 | 0.41 | 1.10 | (0.53–2.25) |
| p=0.468 | p for trend=0.868 | p=0.424 | p for trend=0.803 | |||||
| Mother educational level (years) | ||||||||
| <5 | 4.34 | 1.43 | 1 | ref | 2.13 | 0.55 | 1 | ref |
| 5–9 | 4.62 | 1.17 | 1.02 | (0.49–2.14) | 2.17 | 0.37 | 1.08 | (0.56–2.08) |
| 10/dez | 4.48 | 1.23 | 0.55 | (0.19–1.54) | 2.12 | 0.33 | 0.49 | (0.20–1.19) |
| >12 | 4.55 | 1.08 | 0.58 | (0.18–1.19) | 2.11 | 0.36 | 0.88 | (0.31–2.49) |
| p=0.464 | p for trend=0.368 | p=0.456 | p for trend=0.295 | |||||
| Father educational level (years) | ||||||||
| <5 | 4.29 | 1.36 | 1 | ref | 2.09 | 0.43 | 1 | ref |
| 5–9 | 4.54 | 1.23 | 1.41 | (0.69–2.89) | 2.14 | 0.41 | 1.19 | (0.63–2.26) |
| 10/dez | 4.76 | 1.10 | 3.51 | (1.25–9.85) | 2.23 | 0.41 | 2.19 | (0.93–5.14) |
| >12 | 4.41 | 1.12 | 1.47 | (0.42–5.13) | 2.12 | 0.32 | 1.29 | (0.43–3.86) |
| p=0.464 | p for trend=0.167 | p=0.527 | p for trend=0.279 | |||||
| Kidmed score | ||||||||
| Low | 4.09 | 1.26 | 1 | ref | 2.10 | 0.34 | 1 | ref |
| Medium | 4.70 | 1.21 | 2.69 | (1.32–5.48) | 2.19 | 0.45 | 1.79 | (1.00–3.20) |
| High | 4.79 | 1.10 | 5.70 | (1.53–21.33) | 2.19 | 0.47 | 2.83 | (0.89–8.96) |
| p=0.471 | p for trend=0.001 | p=0.047 | p for trend=0.018 | |||||
| Total | 4.58 | 1.24 | 2.17 | 0.42 | ||||
SD: standard deviation; OR: odds ratio; 95% CI: 95% confidence interval.
The present study showed that a higher adherence to the Mediterranean diet was associated with higher diet cost. The average TDC found in this sample of school-aged children was 4.58€. As far as we know, only few studies24–26 have focused on the estimation of diet cost among children. In a study conducted within a Spanish sample aged 2–24 years old, researchers reported a mean daily diet cost of 3.16€ (data collected in the year 2000) and, more recently, two studies25,26 conducted within the DONALD cohort study, which includes German children, found daily diet costs also close to 3€. Studies among adults in Europe and US, reported average prices higher than 5€.12,14,17
One out every twenty children in this study reported high adherence level to the Mediterranean dietary pattern, results that are in line with previous studies in Mediterranean countries.27 The explored relationship between diet cost and adherence to the Mediterranean diet has brought interesting results, as it was verified an increasing cost with a higher adherence to Mediterranean diet. A similar study in Spanish youth (participants were aged between 2 and 24 years)24 has found similar results. In literature, much has already been discussed on the higher cost of healthy diets,13,14,25,29–31 of which Mediterranean diet is a good example.12,15,16,28–31 There are a few pointed aspects underlying this phenomenon, which are important to refer. The first is the content in energy dense foods that, apparently cheapen the diet,12–14,26,29 association that has already been demonstrated in the current sample of school-aged children.32 In another study, Rydén et al. verified higher cost of diet associated with its healthiness (assessed using the Healthy Eating Index), in which energy-density was low.31 Secondly, variety, a characteristic of healthy dietary patterns, is associated with a large number of food groups and foods among groups.33 Hence, and according to the literature, healthier groups are associated with higher costs, making the diet more expensive. In accordance to our results, food items that play an important role in the Mediterranean diet such as fruits and vegetables, but also fish, were associated to higher costs in different studies.12,30,31 Moreover, the contribution of healthier options within the latter group, such as lean meats and low-fat products, was further associated in the current study with an increased cost. Data in the literature relates higher costs and healthier options within the same food group.31 However, when analyzing Mediterranean diet in this perspective, Drewnowski et al.28 stated that not all nutrient-rich foods necessarily cost more and so, it should be possible to construct a Mediterranean-style diet using the lower cost options in every category.
A possible consequence of higher cost of healthy diets, such as the Mediterranean, is the higher prevalence of poor quality meals within low socioeconomic position (SEP) families, who cannot afford to spend much of the family budget on healthy foods.7,34 A study conducted in Portugal in 2006 by Moreira et al. showed that a higher education was positively linked to a better dietary quality, represented by a higher frequency of milk, vegetable soup, vegetables, fruit and fish consumption,35 all of which are commonly consumed within the Mediterranean pattern. The three most common SEP indicators are education, occupation and income. However, in the present study, only parental education was evaluated, and no significant association with diet cost was found. A subsequent study covering disposable family income could add a vital step to overtake this limitation, as it was described as a better SEP marker with regard to food budget choice by Rydén et al.31
Some methodological limitations are worth noting. First, dietary intake and cost estimates were derived from a 24h recall. The use of this instrument may have compromised the collected information, since it has been recognized that children younger than 8 years-old may not accurately recall foods and estimate portion sizes.36 Nevertheless, only approximately a quarter of our sample was younger than 8 years-old. In addition, single 24h recall may not represent the usual dietary intake and may fail to include foods and beverages that are either forgotten or consumed infrequently, influencing the KIDMED score. As most participants were not able to detail the ingredients of the recipes (and the fat used for cooking, especially concerning for the item “diet includes olive oil”) some assumptions were made, based on traditional Portuguese recipes. However, this fact may be diluted as a whole, given the sample size.
Second, the food price collection was based only in one source, which may have been minimized by the fact that the supermarket chain where the prices were collected has the largest share of food market in Portugal. Also, food prices were collected three years after the dietary survey was conducted, and some changes might have occurred in that period. However, this fact is mitigated by the expectation that prices have varied in a similar way, since the Value Added Tax has not changed during the period elapsed. In addition, the seasonal variability of fresh foods production, namely fruits and vegetables, may have compromised the accuracy of the prices collected, due to the fact that food prices were gathered in a different season of the survey. Nevertheless, it is expected that, in all seasons, the prices of fresh products whose production is seasonally variable, vary so that the rise in some prices is offset by a decline of others. In turn, energy dense foods are the most resistant to inflation.14 In some cases, a lack of details about food consumed determined the need to use average values (grouping fresh and tanned foods, for instance). The use of the average price does not capture differences between brand foods and consequently underestimate the variability of food prices and of the costs associated with individual food consumption,37 which may contribute to explain the lack of association between diet cost and parental education. Furthermore, since the current study has a cross-sectional design, we are limited to demonstrate associations and the direction of these associations.
Nevertheless, this was an original study that brought important insight into dietary costs of children and its association with socio-demographics and adherence to Mediterranean diet, a topic becoming significant in terms of Public Health nutrition worldwide, especially given the economic crisis that has settled in Europe and Mediterranean countries. As food price is becoming a primary determinant of food choice, this new information should concern and be considered by nutritional health care providers and public health authorities. Nutritional education and promotion of healthy eating should be provided in a cost effective manner.
Conflict of interestsThere were no conflicts of interest declared.
Author's contributionGA, PM and PP designed the study; GA, PM, RR, AA, VT, RB, OL, AM and PP conducted the study; RR, AA and OL collected the data; GA, PM, VT and PP analyzed the data; GA and PP wrote the manuscript. All authors read and approved the final manuscript.