

The present study aimed to evaluate the effectiveness of the ACT – Raising Safe Kids Program in different socioeconomic contexts. The sample included 64 mothers of children aged 3–8 years, and 64 other caregivers, divided into three groups according to family socioeconomic level and type of school of the children (C-Public, B-Public and B-Private). The maternal parenting practices and behavior of the children were evaluated pre- and post-intervention with the ACT Program in group. Regardless of the socioeconomic level of the families and the type of school of the children, the ACT Program was effective in improving maternal parenting practices and behavior of the children, according to the perception of the mothers and other caregivers. The findings demonstrate the validity of the ACT Program in Brazilian context for socioeconomic levels B and C and public and private schools.
El objetivo del presente estudio fue evaluar la eficacia del Programa ACT Educando a Niños en Ambientes Seguros en distintos contextos socioeconómicos. En la muestra se incluyeron 64 madres de niños de entre 3 y 8 años de edad y otros 64 cuidadores, que se dividieron en 3 grupos conforme al nivel socioeconómico familiar y al tipo de colegio al que acudían los niños (C-Público; B-Público y B-Privado). Se evaluaron las prácticas educativas de las madres y el comportamiento de los hijos pre y postintervención con el Programa ACT en el grupo. Con independencia del nivel socioeconómico familiar y del tipo de colegio de los niños, el Programa ACT fue eficaz y mejoró las prácticas educativas materna y el comportamiento infantil, según la percepción de las madres y los cuidadores. Los hallazgos demuestran la validez del Programa ACT en el contexto brasileño para los niveles socioeconómicos B y C y los colegios públicos y privados.
Among all the roles played by parents, parenting is one of the most challenging tasks with important personal and social implications. Parenting is a process to educate, protect and guide the children during their developmental trajectory (Brooks, 2013; Pereira, Goes, & Barros, 2015). The strategies used by parents to guide the behavior of their children are called parenting practices (Grusec & Lytton, 1988; Mussen, Conger, Kagan, & Huston, 1990).
The maternal characteristics, family socioeconomic status and behavior of the child are variables that influence the dynamics of the mother–child interactions (Poehlmann et al., 2011; Potharst et al., 2012). The socioeconomic status is a relevant distal variable of the developmental contexts of the child, more specifically, of the exosystem (Bronfenbrenner, 1996; Linhares, 2015). Children from lower economic classes that have experienced family violence, directly as an agent or indirectly as a witness or victim, are more likely to be involved in bullying situations at school, as the target or author of the violence (Pinheiro & Williams, 2009). To grow up in violent communities and homes can cause a child to exhibit more behavioral problems, show more evidence of post-traumatic physical symptoms and experience feelings of low self-esteem (Landers, Da Silva e Paula, & Kilbane, 2013). Therefore, when using parenting practices that involve violence, the family microenvironment acts as a chaotic development context, constituting a risk factor for the child development (Bronfenbrenner & Evans, 2000).
In order to promote the development of children, preventive intervention programs for parents can act as protection mechanisms for the development. These are designed with the aim of improving the knowledge and parenting skills (Haslam, Mejia, Sanders, & Vries, 2016), and providing support for the parents, demonstrating effectiveness in the prevention of child abuse and neglect (Holzer, Higgins, Bromfield, & Higgins, 2006), in the reduction of the risk of child maltreatment (Mikton & Butchart, 2009) and in the promotion of healthy development (O’Connell, Boat, & Warner, 2009).
The preventive intervention programs are classified as universal, selective, and indicated (Essau, 2002; O’Connell et al., 2009). The universal programs attend general population, whose individuals are not identified specifically at-risk. The selective programs target individuals or groups at-risk, such as alcoholics or violent parents. Finally, the indicated programs target individuals with biological markers, psychosocial vulnerabilities, early symptoms, or problems, such as behavior problems, mental health problems. The advantages of the universal program could be implemented in large scale and protect individuals against stigmatization, and also facilitate the recruitment.
In Brazil, as far as we know, there were few universal preventive parenting programs with systematic and structured manual. Predominantly, the parenting programs are selective and indicative directing to mothers with multiple maltreatment violence (Pereira, D’Affonseca, & Williams, 2013), and mothers with marital violence history (Williams, Santini, & D’Affonseca, 2014). An example of a universal prevention program was addressed to mothers of infants focus on improving positive parenting practices (Nogueira, Rodrigues, & Altafim, 2013).
Differently, in the international context, there are effective parenting programs. According to the recent review study by Altafim and Linhares (2016), three universal preventive intervention programs to promote parenting practices are prominent, namely: Incredible Years (Webster-Stratton, 2006), Triple P – Positive Parenting Program (Sanders, 2008) and ACT– Raising Safe Kids Parenting Program (Silva, 2007, 2009). Among these, the ACT – Raising Safe Kids Parenting Program, which was developed by the American Psychological Association (APA, Washington, USA), focuses on the prevention of abusive and violent parenting. The ACT Program is based on social learning theory of Bandura and social-cognitive framework. The aim of ACT is to strengthen families and improve or change parenting skills through the dissemination of knowledge about non-violent discipline, child development, anger management, skills for conflict resolution, effects of the media on children and methods to protect them from exposure to violence, distributed in eight group sessions (Knox, Burkhart, & Hunter, 2010; Silva, 2007). The ACT have been applied in different countries, as USA, Japan, Peru, Colombia, Greece, Bosnia, Turkey, and Taiwan and recently in Brazil and Portugal.
The ACT Program can be implemented as part of public health activities in communities, showing itself to be a promising preventive intervention program due to the positive results of the studies performed with it, as well as their level of relevance and scientific evidence (CEBC, 2014). Furthermore, it should be noted that the ACT Program was nominated by the World Health Organization as one of the three effective parenting programs for use in the prevention of violence against children (NCPFCE, 2015).
The majority of the studies conducted on the ACT Program have been performed in the United States (Silva & Williams, 2015). After the participation in the ACT program by parents and caregivers, there was a reduction in both physical and psychological aggressive parenting behaviors (Knox et al., 2010; Knox, Burkhart, & Cromly, 2013; Portwood, Lamber, Abrams, & Nelson, 2011), a reduction in the child behavior problems (Knox & Burkhart, 2014; Knox, Burkhart, & Howe, 2011), including a reduction of bullying behaviors (Burkhart, Knox, & Brockmyer, 2013). In addition, there were changes indicating more effective parenting (Portwood et al., 2011), with an increase in affectionate behavior by the parents (Knox & Burkhart, 2014) and an increase in the participants knowledge about anger management, problem resolution and non-aggressive discipline (Weymouth & Howe, 2011). However, the studies performed present limitations that should be considered in order to fill gaps in the scientific literature, through the performance of new studies, these being: (i) all of the published studies were conducted in the United States, even though the ACT Program is applied in various countries; (ii) as far as is known, there are no studies evaluating the applicability of the ACT Program for different socioeconomic levels; (iii) some studies evaluated the effectiveness of the ACT Program with small samples (Porter & Howe, 2008); (iv) the use of the ACT Evaluation Questionnaire or the development of other instruments has not yet been standardized, as the main measure of the studies (Knox et al., 2010; Weymouth & Howe, 2011); (v) pre-intervention evaluation were applied at the moment after starting the intervention (Porter & Howe, 2008); (vi) absence of reporting measures with multiple informants (Burkhart et al., 2013; Knox & Burkhart, 2014; Knox et al., 2010, 2011, 2013; Porter & Howe, 2008; Portwood et al., 2011; Weymouth & Howe, 2011).
Despite the advances performed, there is still a need for new findings that enhance the applicability of the ACT Program. Accordingly, the present study aimed to fill some of the aforementioned gaps, especially in relation to evaluating the applicability of this parenting program with a Brazilian sample, including participants from different socioeconomic backgrounds and multiple informants on the child behavior. This study aimed to evaluate the effectiveness of the ACT Program in families of children enrolled in public and private schools and differentiated by socioeconomic level. The study hypothesis was that the intervention with the ACT program would be effective for improving the maternal parenting practices and the child behavior, regardless of the socioeconomic status of the families and the type of school of the children evaluated.
MethodParticipantsThe sample consisted of 64 mothers (or legal guardian who performed the maternal role) of children 3–8 years of age, of both genders, living in Ribeirão Preto/SP. Data were also collected from 64 other primary caregivers, in addition to the mother, who participated as informants to complement the evaluations of the child behavior. For the composition of the sample of mothers, the inclusion criteria were: (i) biological mothers or other legal guardian performing the maternal function (for example: grandparents with legal custody); (ii) residents of Ribeirão Preto city (southwest of Brazil); (iii) with children enrolled in a public or private school; (iv) mothers of children in the three and eight years age group; and (iv) mothers of children with capacitating mental. For the composition of the sample of other primary caregivers, the inclusion criterion established was regularly acting in the education and care of the child.
The exclusion criteria for enrollment were the following: (i) mothers with apparent cognitive impairment, which could lead to impairment in understanding instructions; (ii) mothers who were participating in some other kind of guidance related to parenting practices. In the data analysis, it was included only the data of participants who completed both pre- and post-intervention evaluations, and of mothers who completed at least seven of the eight sessions of the ACT Program.
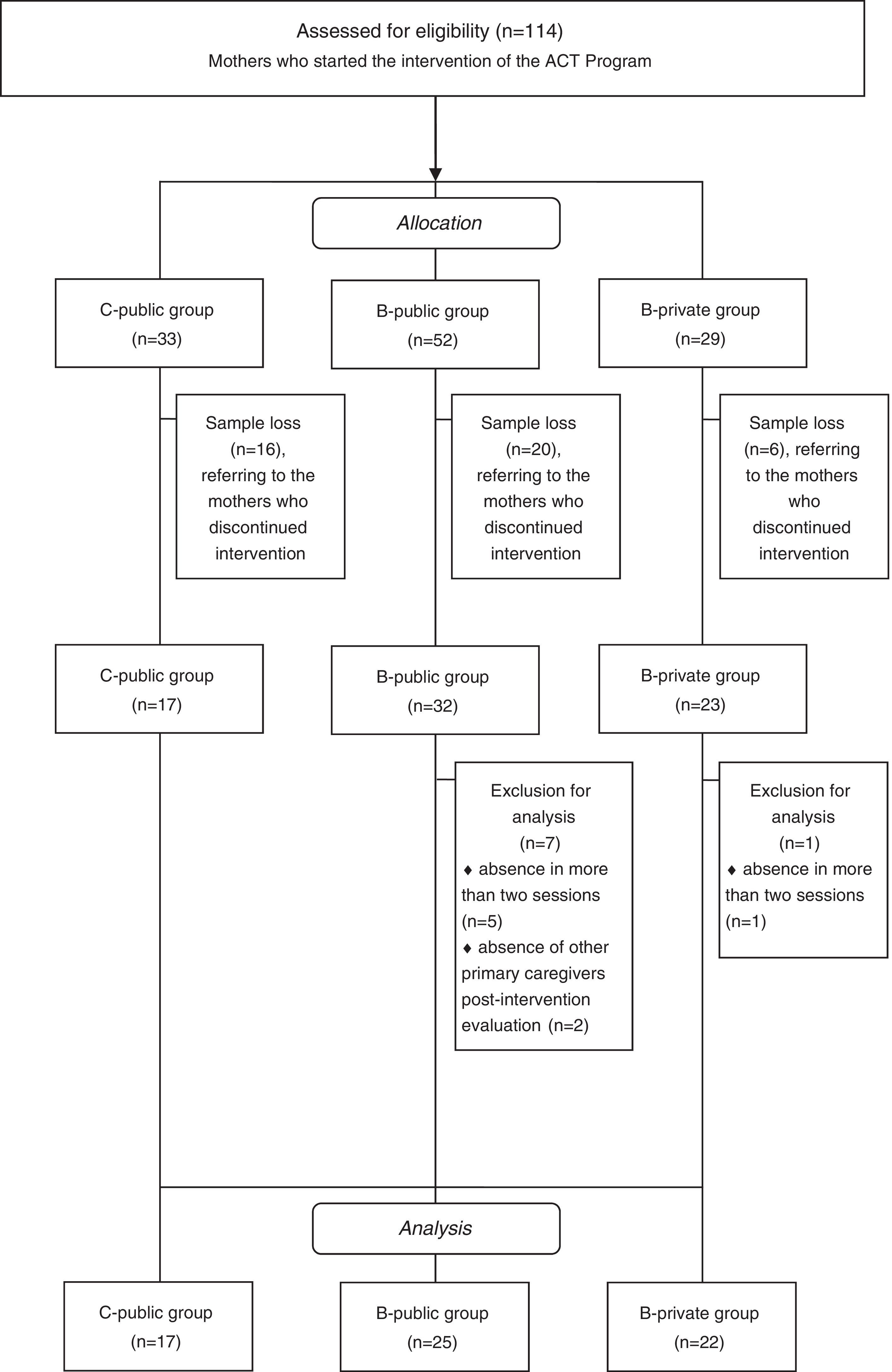
Participants included in the study were exclusively B or C socioeconomic level, as stated by Economic Classification Criterion Brazil (ABEP, 2014), whom were divided into three groups, according to the family socioeconomic level combined with the type of school of the children: C-Public, B-Public, and B-Private (Fig. 1).

A total of 114 mothers were eligible for inclusion in the study, with 33 belonging to the C-Public group, 52 to the B-Public group and 29 to the B-Private group. In relation to sample loss, considering the three groups, there was a loss of 42 mothers who stopped participating in the intervention, namely: 16 mothers of the C-Public group, 20 mothers of the B-Public group and six mothers of the B-Private group. Predominantly, the reasons for dropping out of the mothers were difficulties to participate regarding the schedule of the meetings due to work, as well as issues related to mother's health problems. The adherence of mothers to participate in the ACT program was 51% in C-Public group, 61% in B-Public group and 79% in B-Private group.
After the start of the intervention, seven mothers belonging to the B-Public group were excluded from the study sample, five for not completing the minimum number of sessions and two due to the absence of the post-intervention evaluation of the family. Regarding the B-Private group, only one mother was excluded from the study due to not attending the minimum number of sessions. Therefore, the sample consisted of 64 mothers, 17 of whom belong to the C-Public group, 25 to the B-Public group and 22 to the B-Private group.
Considering the mothers that did not participate in the study (n=50 [n=42, lost sample, and n=8, excluded from analysis]) 32% belonged to the C-Public group, 54% to the B-Public group and 14% to the B-Private group. There were no statistically significant differences between the group of mothers who did not participate in the study and the group of mothers who participated in relation to main sociodemographic characteristics, such age and gender of the children and age and education of the mothers (data not shown).
This study was approved by the Research Ethics Committee of the Clinical Hospital, Ribeirão Preto Medical School of University of São Paulo (FMRP-USP).
Instruments and measuresParenting practicesParenting practices were self-reported by mothers using the ACT Questionnaire, version in Portuguese-Brazil (Silva, 2009), which is part of the materials of the parenting program ACT Raising Safe Kids developed by the American Psychological Association (Silva, 2009). The University of São Paulo has a Memorandum signed by APA and FMRP-USP authorizing the promotion, implementation and evaluation of the ACT Program in Brazil. The present study used the following three scales of the ACT Questionnaire: (1) Parenting Style (10 items related to how parents behave with respect to inappropriate behavior of their children, such as “When my child misbehaves I do a long sermon or I talk straight to the point”); (2) Electronic Media (9 items to check the control of the parents regarding access of the child to the Electronic Media, including television, internet and video games, e.g. “How often do you switch channels from inappropriate programs”); and (3) parental behavior (10 items, related to the parents’ attitudes in different situations with the child, as well as their participation and contribution to violence prevention, e.g. “I calmed myself down when I was angry so my child could learn how to do the same”). Item responses for parental style and parental behavior sections are made on a 5-point Likert scale ranging from 1 to 5 (total score ranging from 10 to 50), and Electronic Media are made on a 4-point Likert scale (total score ranging from 5 to 36). Higher scores indicate better parenting practices, for all of the scales. Previously, the internal consistency of ACT short-form found by Knox et al. (2013) was alpha=0.77. The internal consistency obtained in the present study sample was alpha=0.78 for Parenting Style scale, alpha=0.65 for parental behavior scale, and alpha=0.68 for Electronic Media scale.
Child behaviorChild behavior was measured using the Strengths and Difficulties Questionnaire (SDQ), proposed by Goodman (1997), translated into Portuguese and adapted to the Brazilian socio-cultural characteristics by Fleitlich, Cortázar, and Goodman (2000). The SDQ is a brief behavioral screening questionnaire about 25 attributes, some positive and others negative, of children between 3 and 16 years old (versions P3-4 and P4-16). These 25 items are divided between five subscales, including behavioral problems (emotional symptoms, conduct problems, hyperactivity and relationship problems with peers) and capacities (prosocial behavior) of the children. Item responses are made on 3-point Likert scale: not true, somewhat true, and certainly true. Higher scores indicate more behavior problems, with the exception of the prosocial behavior scale, in which higher scores indicate greater capacity. The instrument presents adequate psychometric properties (Woerner et al., 2004).
Socioeconomic status (SES)The socioeconomic score was measured using the Brazil Economic Classification Criterion from Brazilian Association of Research Companies (ABEP, 2014), available at http://www.abep.org/criterio-brasil. This instrument includes questions of household characteristics, presence and quantity of household assets (e.g. radio, television, bathroom, refrigerator, car), and educational degree of the household head. The ABEP score is a point system with established weights for each item, and the sum of them can vary from 0 to 46 points. Higher score means better socio-economic status. Based on the scores, families can be categorized into Class A1, A2, B1, B2, C1, C2, D, and E; where A1 was the highest economic status and E is the lowest category. For this study, the procedure of joining B1 and B2, and C1 and C2 levels was adopted, thus yielding exclusively two levels (B and C).
Characterization of children and familyA Questionnaire for characterization of children and families was used including items such as: age, gender, level of education, religion, and marital status.
The ACT Raising Safe Kids ProgramThe ACT Program (Silva, 2009), aim to enhance the positive parenting practices and to prevent maltreatment and violence in the behavior of parents and the environmental context of development of children from birth to eight years old. The ACT program was developed by the American Psychological Association's Violence Prevention Office. It is important to note that the focus in ACT could be parents or another main caregiver who nurture the children.
The program comprises the following sessions: Session 1 – Understanding your child behavior (to support parents learn basic elements of child development and how to respond appropriately to behavior of children); Session 2 – Children and Violence (to support parents understand how children can be exposed to violence and the consequences this will have on their lives); Session 3 – How parents can understand and control anger (To support parents learn how to control and deal with anger feeling); Session 4 – How to understand and help children when they feel angry (to support parents understand the anger feeling and how to teach children to control and manage it); Session 5 – Children and Electronic Media (to support parents understand the impact of Electronic Media on child behavior and give options on how to reduce child exposure to violence); Session 6 – Discipline and Parenting Style (to support parents understand that the way to educate their children has an impact on their behavior throughout life); Session 7 – Discipline and positive behavior (to support parents how to prevent child difficult behavior and how to use positive strategies to discipline children); Session 8 – Take ACT Program to your home and your community (to support participants realize what they learn with program, and that is already helping them to realize their dreams for their children); encourage participants to use at home and their community the tools they have learned and strengthen the parents their role as teachers, protectors, and defenders of their children. The ACT comprised a Manual for facilitators; Parents Handbook; ACT Questionnaires for assessments; Control of presence sheet; CD with the content of the sessions in Power Point (for more information see http://www.apa.org/act).
ProceduresData collection was conducted by two trained and expertise psychologists (first and second authors of the study) certificated as facilitators in ACT Program and two assistants. The groups of ACT were conducted with one facilitator accompanied with an assistant. The groups were performed in two private schools, two public schools, two Family Health Program centers and one philanthropic association, with the last two attending children enrolled in community schools. The recruitment of the participants was carried out through different strategies and included meetings with staff and managers to explain the study and establish strategies of dissemination, recruitment, and implementation, brief talks during parent meetings, delivery of explanatory folders in the report books of the children and posters displayed on the premises.
Data collection was carried out from 2013 to 2015. The mothers participated in two evaluations (pre- and post-intervention) and in the intervention with the ACT Program, which took place in eight highly interactive group sessions, one per week (2h per session). In the sessions the mothers received information and developed tasks in groups using the materials, contents, and scenarios included in the material of the program. The ACT provides a set of role-playing proposal and videos to support the activities. In the study, we use the original form of ACT program only including four videos adapted to the cultural context of Brazil.
The ACT Evaluation Questionnaire and Strengths and Difficulties Questionnaire were self-administered in mothers at pre- and post-intervention. If the mothers had more than one child, the mothers were asked to choose the child aged three to eight years that caused the most worry. The other caregivers participated in specific child behavior evaluations, also at the pre- and post-intervention moments. Through the mothers, an envelope was sent containing the Terms of Consent Form and the SDQ Questionnaire.
Data analysisThe data analysis included descriptive and inferential statistical analysis. The main characteristics of groups and the outcomes in the pre-intervention moment were analyzed by between group comparisons using the t-test (continuous variables) and the chi-square or Fisher's exact test (categorical variables). The Shapiro–Wilk test was used to examine the normality of the data and the results confirm the normality of the parenting practices data. The two-way mixed design ANOVA was performed to analyze the effects of groups (C-Public, B-Public and B-Private), moments (pre- and post-intervention), and also the interactive effects of both factors (groups and moments). Also, the Bonferroni post hoc test was used. The effect size was calculated by partial square eta (n2 partial) for ANOVA, identifying the large (0.14), medium (0.06) and small (0.01) size effects. Additionally, the between-group comparison was carried out using the MANOVA to analyze the standardize z-scores of ACT scales together in pre- and post- intervention, independently. The significance level adopted for all tests was 5% (p≤0.05).
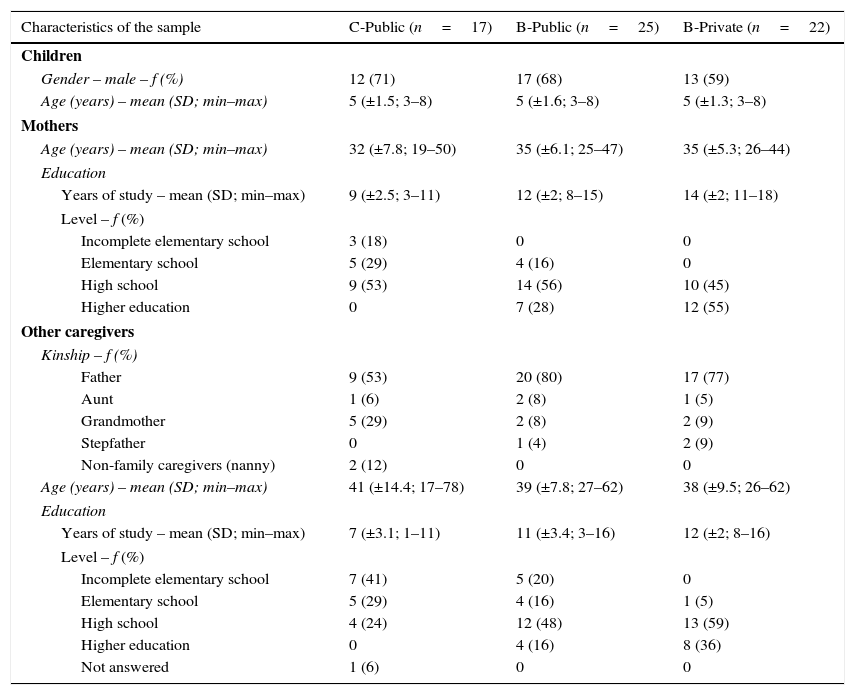
ResultsTable 1 shows that there was a predominance of boys with a mean age of 5 years old in all groups. The other main caregivers participants are predominantly fathers. As might be expected, statistically significant differences were found between the groups regarding mothers’ educational status (C-Public vs B-Public, p=0.0001; C-Public vs B-Private, p=0.0001; B-Public vs B-Private, p=0.008) and the other caregivers’ educational status (C-Public vs B-Public, p=0.003; C-Public vs B-Private, p<0.0001; B-Public vs B-Private, p=0.01). Mothers and other main caregivers of the C-Public group had fewer years of education, compared to both the B-Public and B-Private groups, and also mothers and other main caregivers of the B-Public presented fewer years of education than B-Private group. There were no statistically significant differences between the groups on the variables gender and age of the children, mothers’ age and caregivers’ age.
Characteristics of the sample of mothers, children and other caregivers, according to the groups divided by the socioeconomic level of the families and type of school of children.
| Characteristics of the sample | C-Public (n=17) | B-Public (n=25) | B-Private (n=22) |
|---|---|---|---|
| Children | |||
| Gender – male – f (%) | 12 (71) | 17 (68) | 13 (59) |
| Age (years) – mean (SD; min–max) | 5 (±1.5; 3–8) | 5 (±1.6; 3–8) | 5 (±1.3; 3–8) |
| Mothers | |||
| Age (years) – mean (SD; min–max) | 32 (±7.8; 19–50) | 35 (±6.1; 25–47) | 35 (±5.3; 26–44) |
| Education | |||
| Years of study – mean (SD; min–max) | 9 (±2.5; 3–11) | 12 (±2; 8–15) | 14 (±2; 11–18) |
| Level – f (%) | |||
| Incomplete elementary school | 3 (18) | 0 | 0 |
| Elementary school | 5 (29) | 4 (16) | 0 |
| High school | 9 (53) | 14 (56) | 10 (45) |
| Higher education | 0 | 7 (28) | 12 (55) |
| Other caregivers | |||
| Kinship – f (%) | |||
| Father | 9 (53) | 20 (80) | 17 (77) |
| Aunt | 1 (6) | 2 (8) | 1 (5) |
| Grandmother | 5 (29) | 2 (8) | 2 (9) |
| Stepfather | 0 | 1 (4) | 2 (9) |
| Non-family caregivers (nanny) | 2 (12) | 0 | 0 |
| Age (years) – mean (SD; min–max) | 41 (±14.4; 17–78) | 39 (±7.8; 27–62) | 38 (±9.5; 26–62) |
| Education | |||
| Years of study – mean (SD; min–max) | 7 (±3.1; 1–11) | 11 (±3.4; 3–16) | 12 (±2; 8–16) |
| Level – f (%) | |||
| Incomplete elementary school | 7 (41) | 5 (20) | 0 |
| Elementary school | 5 (29) | 4 (16) | 1 (5) |
| High school | 4 (24) | 12 (48) | 13 (59) |
| Higher education | 0 | 4 (16) | 8 (36) |
| Not answered | 1 (6) | 0 | 0 |
Note: f=frequency; %=percentage; SD=standard deviation; min=minimum value; max=maximum value; p≤0.05.
Additional information about monthly family income showed that in the C-Public group, 29% of the mothers had a family income below R$ 1000.00, 59% from R$ 1000.00 to R$ 3000.00 and only 6% had a family income from R$ 3100.00 to R$ 5000.00. No mother belonging to this group had a monthly family income over R$ 5000.00. The minimum salary in Brazil during the period of data collection was R$ 880.00
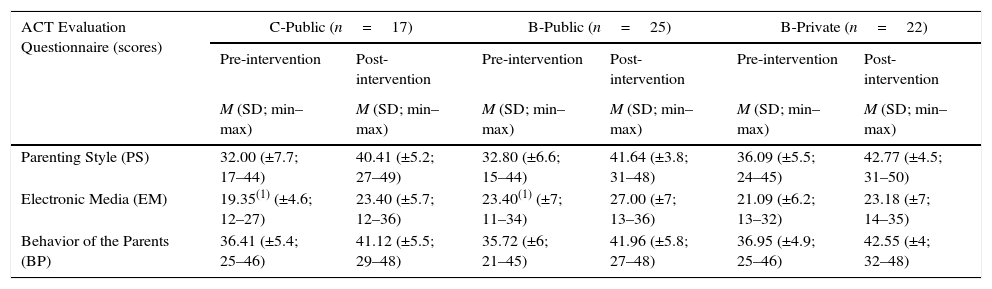
In Table 2, in the pre-intervention moment, the Parenting Style and Behavior of the Parents scales there were no statistically significant differences between the groups. In the Electronic Media scale, some items were not applicable for some mothers and then the total scores were not comparable. For this reason, the between groups comparison was not performed in the pre-intervention.
Scores in the ACT Evaluation Questionnaire (Parenting Style, Electronic Media and Behavior of the Parents) at the moments of pre- and post-intervention of the ACT Program, according to the groups divided by the socioeconomic status of the families and type of school of the children.
| ACT Evaluation Questionnaire (scores) | C-Public (n=17) | B-Public (n=25) | B-Private (n=22) | |||
|---|---|---|---|---|---|---|
| Pre-intervention | Post-intervention | Pre-intervention | Post-intervention | Pre-intervention | Post-intervention | |
| M (SD; min–max) | M (SD; min–max) | M (SD; min–max) | M (SD; min–max) | M (SD; min–max) | M (SD; min–max) | |
| Parenting Style (PS) | 32.00 (±7.7; 17–44) | 40.41 (±5.2; 27–49) | 32.80 (±6.6; 15–44) | 41.64 (±3.8; 31–48) | 36.09 (±5.5; 24–45) | 42.77 (±4.5; 31–50) |
| Electronic Media (EM) | 19.35(1) (±4.6; 12–27) | 23.40 (±5.7; 12–36) | 23.40(1) (±7; 11–34) | 27.00 (±7; 13–36) | 21.09 (±6.2; 13–32) | 23.18 (±7; 14–35) |
| Behavior of the Parents (BP) | 36.41 (±5.4; 25–46) | 41.12 (±5.5; 29–48) | 35.72 (±6; 21–45) | 41.96 (±5.8; 27–48) | 36.95 (±4.9; 25–46) | 42.55 (±4; 32–48) |
Note: M=mean; SD=standard deviation; min=minimum value; max=maximum value; score PS and BP (range from 10 to 50) and EM score (range from 9 to 36). In each scale, the higher the score, the better the behavior of the participant in relation to these aspects.
There were statistically significant differences within moments, considering pre- and post-intervention moments, in all scales of ACT Evaluation, as: Parenting Style (F[1; 61]=104.83; p<0.0001; n2=0.63, large effect size), Electronic Media (F[1; 61]=39.13; p<0.0001; n2=0.39, large effect size), and Parents Behavior (F[1; 61]=52.57; p<0.0001; n2=0.46, large effect size). There were no significant effects of group factor or interaction between groups and moments. Regardless of the socioeconomic level and type of school of the children, the scores were higher, in the three groups, in the scales of the ACT Evaluation, at the post-intervention moment, compared to the pre-intervention moment, according to maternal perception.
The MANOVA results showed that there were no differences between the three groups in the ACT scales together (Parenting Style, Electronic Media, and Parents Behavior), both pre- and post- intervention (pre-intervention: Pillai's Trace=0.17, F(6; 120)=1.84; p=0.10 and post-intervention: Pillai's Trace=0.13, F(6; 120)=1.38; p=0.23).
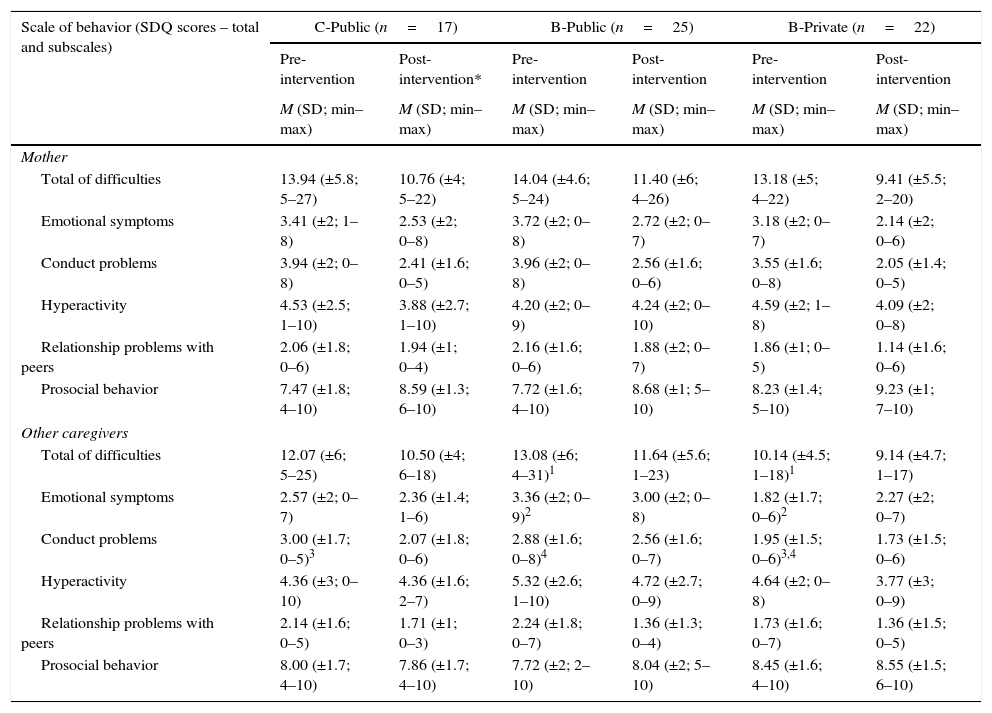
Table 3 shows that, at the pre-intervention moment, with respect to the behavior of the children evaluated by the mothers, there was no statistically significant difference between the groups. In the pre-intervention moment of the ACT Program, with respect to the behavior of the children evaluated by the other caregivers, there was statistically significant difference between the C-Public and B-private groups in the conduct problems subscale and between the B-Public and B-Private groups in the total of behavioral difficulties, in emotional symptoms and in conduct problems. This means that the children of the B-private group presented fewer behavioral problems and less emotional symptoms than the children of the B-Public group. In addition, the children of the B-Private group presented fewer behavioral problems compared to the children of the other two groups.
Indicators of behavioral difficulties and capabilities (SDQ score) of the children at the moments of pre- and post-intervention of the ACT Program, according to the perception of the mothers and the other primary caregivers, in groups divided by the socioeconomic status of the families and type of school of the children.
| Scale of behavior (SDQ scores – total and subscales) | C-Public (n=17) | B-Public (n=25) | B-Private (n=22) | |||
|---|---|---|---|---|---|---|
| Pre-intervention | Post-intervention* | Pre-intervention | Post-intervention | Pre-intervention | Post-intervention | |
| M (SD; min–max) | M (SD; min–max) | M (SD; min–max) | M (SD; min–max) | M (SD; min–max) | M (SD; min–max) | |
| Mother | ||||||
| Total of difficulties | 13.94 (±5.8; 5–27) | 10.76 (±4; 5–22) | 14.04 (±4.6; 5–24) | 11.40 (±6; 4–26) | 13.18 (±5; 4–22) | 9.41 (±5.5; 2–20) |
| Emotional symptoms | 3.41 (±2; 1–8) | 2.53 (±2; 0–8) | 3.72 (±2; 0–8) | 2.72 (±2; 0–7) | 3.18 (±2; 0–7) | 2.14 (±2; 0–6) |
| Conduct problems | 3.94 (±2; 0–8) | 2.41 (±1.6; 0–5) | 3.96 (±2; 0–8) | 2.56 (±1.6; 0–6) | 3.55 (±1.6; 0–8) | 2.05 (±1.4; 0–5) |
| Hyperactivity | 4.53 (±2.5; 1–10) | 3.88 (±2.7; 1–10) | 4.20 (±2; 0–9) | 4.24 (±2; 0–10) | 4.59 (±2; 1–8) | 4.09 (±2; 0–8) |
| Relationship problems with peers | 2.06 (±1.8; 0–6) | 1.94 (±1; 0–4) | 2.16 (±1.6; 0–6) | 1.88 (±2; 0–7) | 1.86 (±1; 0–5) | 1.14 (±1.6; 0–6) |
| Prosocial behavior | 7.47 (±1.8; 4–10) | 8.59 (±1.3; 6–10) | 7.72 (±1.6; 4–10) | 8.68 (±1; 5–10) | 8.23 (±1.4; 5–10) | 9.23 (±1; 7–10) |
| Other caregivers | ||||||
| Total of difficulties | 12.07 (±6; 5–25) | 10.50 (±4; 6–18) | 13.08 (±6; 4–31)1 | 11.64 (±5.6; 1–23) | 10.14 (±4.5; 1–18)1 | 9.14 (±4.7; 1–17) |
| Emotional symptoms | 2.57 (±2; 0–7) | 2.36 (±1.4; 1–6) | 3.36 (±2; 0–9)2 | 3.00 (±2; 0–8) | 1.82 (±1.7; 0–6)2 | 2.27 (±2; 0–7) |
| Conduct problems | 3.00 (±1.7; 0–5)3 | 2.07 (±1.8; 0–6) | 2.88 (±1.6; 0–8)4 | 2.56 (±1.6; 0–7) | 1.95 (±1.5; 0–6)3,4 | 1.73 (±1.5; 0–6) |
| Hyperactivity | 4.36 (±3; 0–10) | 4.36 (±1.6; 2–7) | 5.32 (±2.6; 1–10) | 4.72 (±2.7; 0–9) | 4.64 (±2; 0–8) | 3.77 (±3; 0–9) |
| Relationship problems with peers | 2.14 (±1.6; 0–5) | 1.71 (±1; 0–3) | 2.24 (±1.8; 0–7) | 1.36 (±1.3; 0–4) | 1.73 (±1.6; 0–7) | 1.36 (±1.5; 0–5) |
| Prosocial behavior | 8.00 (±1.7; 4–10) | 7.86 (±1.7; 4–10) | 7.72 (±2; 2–10) | 8.04 (±2; 5–10) | 8.45 (±1.6; 4–10) | 8.55 (±1.5; 6–10) |
Note: M=mean; SD=standard deviation; min=minimum value; max=maximum value; *at the post-intervention moment, in the C-Public group, 14 families answered; score in the SDQ subscales (range from 0 to 10); SDQ total score (range from 0 to 40). For the total difficulties and emotional symptoms, conduct problems, hyperactivity and relationship problems with peers subscales the higher the score, the worse the behavior of the child. In the prosocial behavior subscale the higher the score, the better the behavior of the child. In each scale, the score can range from 0 to 10 and the total difficulties (the sum of the first four scales) can vary from 0 to 40.
Between groups comparison at the pre-intervention moment; p-value:
There were statistically significant differences within pre- and post-intervention moments, in the child behavior assessed by the mothers, in the following scales: total of difficulties (F[1; 61]=21.90; p<0.0001; n2=0.26, large effect size), emotional symptoms (F[1; 61]=18.06; p<0.0001; n2=0.23, large effect size), conduct problems (F[1; 61]=37.75; p<0.0001; n2=0.38, large effect size), relationship with peers (F[1; 61]=4.0; p=0.05; n2=0.06, medium effect size), and prosocial behavior (F[1; 61]=25.23; p<0.0001; n2=0.29, large effect size). According to the mothers’ perception, all groups reduced the total behavioral problems, emotional symptoms, conduct behavior, and relationship problems with peers and increased the prosocial behavior. Finally, there was no significant difference between groups on hyperactivity scale. Also, there were no significant effects of group factor or interaction between groups and moments.
There were statistically significant differences within pre- and post-intervention moments, in the child behavior assessed by the other caregivers, in the following scales: total of difficulties (F[1; 58]=5.66; p=0.02; n2=0.09, medium effect size), conduct problems (F[1; 58]=4.73; p=0.03; n2=0.08, medium effect size), and relationship with peers (F[1; 58]=5.83; p=0.02; n2=0.09, medium effect size). Concerning the other caregivers’ perception, all groups reduced the total behavioral problems, conduct behavior, and relationship problems with peers. Finally, there were no statistically significant differences on emotional symptoms, hyperactivity, and prosocial scales. Also, there were no significant effects of group factor or interaction between groups and moments.
DiscussionIn the present preliminary study, the results confirmed the initial hypothesis that the intervention with the universal prevention ACT Program is effective for improving maternal parenting practices and the child behavior, regardless of the socioeconomic level of the families (level B or C) and type school of the children (public or private). The adherence rates in the program were 51% in mothers C-Public, 61% in mothers B-Public, and 79% in the mothers B-Particular. These findings showed a higher adherence rate in the higher socioeconomic level, specifically in the group of mothers whose children are in private school. The adherence rates in the current study were similar to the rate of 68% found by Alvarez, Rodrigo, and Byrne (2016).
Although, prior to the intervention, the mothers already presented positive indicators regarding parenting practices, the ACT Program demonstrated its effectiveness to modify the type of discipline used to provide consequences for the behavior of the child, monitoring the access of the children to Electronic Media and maternal attitudes in different situations experienced with the child, as well as the participation and contribution of the mothers in the prevention of violence, according to maternal perception. The findings of this study in Brazil were similar to previous studies with the ACT Program, in the North American context, that aimed to evaluate its effectiveness with respect to the modification of parenting practices (Knox et al., 2010, 2013; Porter & Howe, 2008; Portwood et al., 2011; Weymouth & Howe, 2011) and of the behavior of the child (Burkhart et al., 2013; Knox & Burkhart, 2014; Knox et al., 2011; Porter & Howe, 2008).
Some differences can be observed between studies previously conducted with the ACT Program and the present study. Differently from the present study, the study of Porter and Howe (2008) did not find statistical significant improvement, post- intervention, with respect to the parental monitoring of the access of the children to Electronic Media; however, there was only a marginal difference from pretest to follow-up. Because of that, the authors hypothesized that the awareness of the impact of Electronic Media on childhood development was characterized as being a gradual process and therefore could take longer to identify. In the study of Knox et al. (2010), both in the intervention group, submitted to the ACT Program, as well as in the control group, a statistically significant difference was found, with respect to monitoring Electronic Media, between the pre- and post-intervention moments; however, there was no interactive effect between the moment and the intervention condition. Thus, it was hypothesized that the ACT Evaluation Questionnaire might not be sensitive to small changes or the parents, because they were already undergoing clinical monitoring, may have had access to this type of information. In the studies of Portwood et al. (2011), Knox et al. (2013) and Knox and Burkhart (2014), the ACT Evaluation Questionnaire was not used, and therefore it was not possible to assess whether there was a significant improvement with regard to knowledge about the impact of Electronic Media on the lives of the children. Only one of these studies found that, from the reports of the parents, there was increased awareness of the issue after the intervention (Portwood et al., 2011). Despite the positive effects achieved with the ACT Program, the sample of the study conducted by Porter and Howe (2008) was of low income and had been exposed to multiple stressors, such as homelessness. Thus, the characteristics of the sample studied by the authors make it difficult to generalize the results to people without identification of this degree of risk exposure. The sample of the present study was drawn from the community without identified risk, thus demonstrating the universal character of prevention of the ACT Program.
The results obtained in this study show that the ACT Program intervention was effective, according to the perception of the mothers, in helping them in the important task of monitoring the access of the children to Electronic Media, regardless of the socioeconomic status of the families and the type of school of the children. This finding is consistent with one of the aims of the ACT Program, which is to make parents and caregivers more conscious of the effects of Electronic Media on the behavior of their children, teaching the children to be critical consumers of Electronic Media (Porter & Howe, 2008). Studies show that the improper use of Electronic Media may cause impairments in the development of the child, such as reducing prosocial behavior and increasing aggressive thoughts (Anderson, 2000), reducing school performance (Munni & Malhi, 2006), increasing the likelihood of developing obesity (Stettler, Signer, & Suter, 2004) and increasing negative stress (Munni & Malhi, 2005).
Similarly, in the present study the ACT Program contributed to the mothers of different socioeconomic levels, improving their attitudes, behavior and ways of disciplining their children in different situations experienced, according to maternal perception. By promoting education of the parents and positive parenting practices through strengthening their knowledge and skills, the program improves the positive parenting practices and, thus, increases the guarantee that the child will develop and be raised in a violence-free environment (Landers et al., 2013; Linhares, 2015). Therefore, it is important to invest actions to support and guide parents in the task of raising their children, helping to reduce the level of parental stress and promoting coping strategies for the adverse situations experienced with the child (Minetto, Crepaldi, Bigras, & Moreira, 2012).
With regard to the child behavior, after the intervention with the ACT Program there was an improvement of the indicators of behavioral difficulties and capacities of the children, based on the mothers’ and other caregivers’ perceptions. According to the literature, the importance of the participation of multiple informants regarding child behavior problems is consensual (Kraemer et al., 2003). The possibility of obtaining the perception of more than one informant provides the study with greater accuracy, as it diminishes the chances of bias related to the perception and comprehension of the child behavior.
Regardless of the families’ socioeconomic status and the type of school of the child, there was an improvement in conduct problems and prosocial behavior, according to maternal perception. The mothers of the B-Public and B-Private groups reported improvements in their children with regard to emotional symptoms and, specifically in the B-private group, the children also presented improvements in relationship problems with peers. Previous studies show that the ACT Program was effective in reducing aggressive behavior (Porter & Howe, 2008), bullying behavior (Burkhart et al., 2013) and externalizing behavior problems (Knox et al., 2011; Knox & Burkhart, 2014). Furthermore, in the study by Knox et al. (2011) there was also a reduction in conduct problems after the intervention of the ACT Program, evaluated by the Strengths and Difficulties Questionnaire (SDQ). Importantly, all the studies conducted to evaluate the effectiveness of the ACT Program on the change in behavior of the child used the report of only one informant regarding the behavior of the child, that is, they were not conducted with multiple informants. The studies by Knox et al. (2011) and Knox and Burkhart (2014) did not use the SDQ instrument in its entirety, only the conduct problems subscale.
According to the results of the present study, collected from the perception of the mothers regarding the behavior of the children, it should be noted that after the ACT Program intervention the mothers learned to see the behavior of the children positively and to feel less negative regarding their inappropriate behavior. The Convention on the Rights of the Child, decreed by the United Nations (UN), recognizes the importance of knowledge about childhood development and reiterates the duty of countries to disseminate the basic principles of this theme throughout all sectors of society (Silva, Vieira, de Moura, & Ribas, 2005). Thus, it is essential for public policies directed toward parents to be implemented in order to disseminate basic knowledge of childhood development, thus minimizing possible negative effects on the parenting practices and, consequently, on the development of the child and interaction between parents and children. After the participation of mothers in the ACT Program, according to the perception of the other informant caregiver, the children of the C-Public group presented improvements with respect to conduct problems and the children of the B-Public group improvements with regard to relationship problems with peers.
The results of the present study, as well as the results of previous studies, demonstrate the positive impact of the ACT Program on the mothers’ parenting practices and on the child behavior, contributing to the prevention of child behavior problems or the maintenance of appropriate behavior. The ACT Program is a parental intervention with strategies based on scientific evidence for the prevention of violence, founded on the principles that in the early years of childhood children learn the basic foundations for life. In addition, the ACT Program presents specific aspects in the prevention of violence, including the impact of violence and various methods to protect children from violence in the family, community and media, thus avoiding emotional, cognitive and behavioral consequences (Knox et al., 2011). The ACT Program has as strong characteristic of reaching parents of different socioeconomic levels, since the language used in the concepts and knowledge was translated from the scientific field of Psychology to an accessible language and format.
This study offers support for the development of public policies that aim to include the family as a fundamental part in the adequate development of the child. Parental programs can contribute to modifying the view and the routine of parents, positively influencing the behavior of the child and consequently the family environment.
Human development can be enhanced through public policies that focus on the most important and sensitive periods of childhood. In particular, early childhood is characterized as being one of the periods in which there is a requirement for increased investment in the implementation of rapid actions with coordinated practice together with sectors such as health and education, valuing the contexts that affect children, such as the family, community and school (Macana & Comim, 2015). The influences coming from the macro context, such as the culture in which the child and family are inserted, the government organization and the political and social actions, can affect childhood development and, therefore, should be the focus in the elaboration of public policies directed toward early childhood (Linhares, 2015). Through this study, it is hoped to contribute to ensuring children receive a healthy, happy, dignified and protected childhood, both from the adults accompanying their development and from the government sectors.
It should be noted that the present study has some limitations. The results regarding the socioeconomic level of the families were obtained from the classification of ABEP and did not include families of socioeconomic status of A, D and E, which represent, respectively, the highest and lowest levels according to the instrument; furthermore, the ABEP focuses more on the power to purchase consumer goods. The sample for the intervention was composed only of mothers and there was no control group. Futhermore, the ACT Evaluation Questionnaire is a measure that has still not been psychometrically evaluated completely, needing further studies. The measures regarding the child behavior and the use of other standardized and extensively validated instruments strengthen the results on the effectiveness of the intervention program, the object of this study. However, the ACT Evaluation Questionnaire was designed to evaluate the content covered during the sessions of the ACT Program and, according to the results of previous studies and those of the present study, it has been shown to be a sensitive tool to capture changes related to parenting practices. There was no further analysis of the quality of implementation of the intervention.
Despite the limitations, this study presents relevant aspects and allows the conclusion that the ACT Program has applicability in the Brazilian context with families of socioeconomic level B and C and children from public and private schools. The findings indicate that the ACT Program can be an effective strategy for the acquisition or improvement of parenting practices and the prevention and reduction of child behavior problems. This study advances on feasibility of the ACT Program, characterized as being of universal prevention, in different socioeconomic contexts. Then, the importance is corroborated of universal preventive interventions for improving maternal parenting practices with an impact on the adaptive behavior of the children. Thus, parenting practices start to act as a protective factor for the development of the children.
Although there is increasing scientific evidence regarding the ACT Program, gaps can still be observed that could be filled by further studies, such as paternal involvement in the interventions, conducting randomized controlled trials to evaluate the efficacy of the program including control group and follow-up measures to ensure the maintenance of the learning over time. Additionally, future studies could advance in the psychometric analysis of the ACT instrument. Such gaps may generate questions for further studies on the ACT Program, as well as other universal prevention programs directed toward parenting practices.
ConclusionThe present Brazilian preliminary study of the ACT universal preventive program showed effectiveness to improve parenting practices, improving positive educational strategies and decreasing or eliminating violence and maltreatment in the home. Then, this is a relevant intervention with tested ecological validity that could be subsequently implemented in public policies for communities, used in a large-scale dimension. Additionally, we detected positive impact on the child behavior outcomes improving the psychological adaptive resources. Considering the relevance of the early childhood, the ACT could be a valuable tool to protect child development against stressful and adversity context.
Conflict of interestThe authors have no conflict of interest to declare.
The Foundation for Support of Research in the State of São Paulo, Brazil (FAPESP), for Master's scholarship (MEA Pedro; grant #2013/24655-6) and Doctorate's scholarship (ERP Altafim; grant #2012/25293-8); The National Council of Science and Technology Development (CNPq) for MBM Linhares; Maria Cecília Souto Vidigal Foundation (FMCSV) and The American Psychological Association for the support with the ACT Raising Safe Kids Program. We also thank to Francine Belotti da Silva and Rebeca Cristina de Oliveira for their participation in the data collection as research assistants.
