

A singular parent-support program is limited in its ability to address multiple child and family needs. One innovative solution is braiding, a process in which two evidence-based programs are systematically combined as a newly tailored, cohesive curriculum. In this paper we describe the systematic braiding of two parent-support curricula, Parents as Teachers® and SafeCare®. We highlight implementation challenges to inform future planning and braiding efforts. Based on qualitative data (n=13), we discuss five lessons learned, including identifying a pedagogical approach and sustainability at the model- and site-level. Implications and future directions for braiding and implementation are also discussed.
El programa de apoyo parental en solitario se ve limitado por su capacidad para abordar las múltiples necesidades de niños y familias. Una solución innovadora es el braiding (enlazado), un proceso en el que se combinan sistemáticamente dos programas basados en evidencia, como currículo cohesivo y de nuevo diseño. En este documento describimos el braiding sistemático de dos currículos de apoyo parental, «Parents as Teachers®»y «SafeCare®». Hacemos hincapié en las dificultades de su introducción para informar sobre la planificación futura y los resultados del braiding. Basándonos en los datos cualitativos (n=13), comentamos cinco lecciones aprendidas, incluyendo la identificación de un enfoque pedagógico y la sostenibilidad en relación con el modelo y la localización. También abordamos las direcciones futuras en cuanto a braiding y su introducción.
Unlike child mental health services, there is not a central diagnosis schema guiding child welfare service provision and, as such, there is a lack of consensus of the best intervention practices (Barth & Lee, 2014). Despite the existence of many evidence-informed parent support models, no single model or program comprehensively addresses the complex needs of all children and families (Powell, Bosk, et al., 2015) and, further, not all children and families have the same needs. In some cases, parents have co-occurring issues such as substance use or mental health that need to be addressed (Barth, 2009) prior to modifying parenting skills. In other cases, children's trauma symptoms (Cohen & Mannarino, 2017) may first require attention. In addition to variation in needs, there are variations among the extant parent-support models related to the mechanisms for referral (e.g., mandated or voluntary), prevention needs and targets (e.g., primary or secondary prevention and broader risk factors), and infrastructure capabilities and capacity (e.g., educational background of providers) (Guastaferro & Lutzker, 2017; Sweet & Appelbaum, 2004). Variation is a functional necessity. Any given model is unlikely to address all of a family's needs, and even if such a model existed, it would be cumbersome to implement and unlikely easily disseminated. Further, it is unclear whether all intervention components are necessary to produce behavior change or lower risk for any given family receiving a comprehensive program. There is a fine balance in meeting the needs of children and families and adhering to the guiding principle of parsimony (Berliner et al., 2015).
In practice, agencies are often limited to implementing one model due to funder requirements or as a function of available resources. Thus, agencies must ascertain which model is most in line with the needs of the majority of families served. Providers must also contend with family circumstances that challenge program engagement and thereby success (DuMont et al., 2008; Torres, Fitzgerald, & Shipman, 2014). Therefore, innovative implementation strategies and multicomponent intervention strategies are needed to maximize resources and the impact of behavioral interventions related to improving the well-being of children and families (Aarons, Hurlburt, & Horwitz, 2011). Systematic braiding, a burgeoning practice in which complementary models are combined while maintaining fidelity to the curriculum of each individual model (Guastaferro et al., 2017), is one approach. The braided approach is guided by model purveyors and delivered to all families with fidelity monitored throughout the implementation process.
In response to the need for innovative and multicomponent intervention strategies, we implemented systematic braiding of two parent-support curricula in an effectiveness trial focused on improving the well-being of children and families. We examined whether the systematic braiding approach could comprehensively address the multiple needs of families. Though providers commonly deliver different parent-support models to different families, or multiple models to the same family sequentially (Aarons & Palinkas, 2007), to our knowledge this was the first effort to systematically braid two evidence-based home-based parent support models. Given that fit between the program and the setting is an important determinant of implementation (Aarons et al., 2011), it is key to examine challenges to implementation when braiding two evidence-based models, each of which may differ with respect to demands from the system. The aim of this paper is to reflect upon implementation-specific lessons learned from the preparation for and implementation of the effectiveness trial to inform others who are interested in similar braided work. Thus, the focus of this paper is not on the outcomes of the effectiveness trial, though we recognize the importance of considering outcomes with these implementation lessons. Outcomes will be presented in future publications.
MethodParents as Teachers and SafeCare at Home (PATSCH) is the product of the coordinated effort of the Parents as Teachers (PAT) and National Center National SafeCare Training and Research Center. PAT® is focused on parent–child interaction, development-centered parenting, and family well-being (Albritton, Klotz, & Roberson, 2003). Families who are typically voluntary are enrolled between birth and kindergarten and receive services for at least two years. The families receive home visits, developmental/health screenings, participate in group meetings, and are referred to community resources as needed. The program has demonstrated a positive effect on child and parent outcomes related to school readiness (Zigler, Pfannenstiel, & Seitz, 2008). The providers, referred to as parent educators, serve multiple children within a family's home and, thus, may provide services to a family for multiple years.
SafeCare® is an in-home parent support model designed for families at-risk or reported for maltreatment with children aged birth to five (Guastaferro & Lutzker, 2017; Rostad, Lutzker, & Guastaferro, 2016). Over the course of 18 weekly sessions, parents are trained in parent-infant/child interaction, home safety, and child health. SafeCare has demonstrated effectiveness in improving parenting behaviors and reducing recidivism rates, specifically neglect, in child welfare populations (Chaffin, Hecht, Bard, Silovsky, & Beasley, 2012).
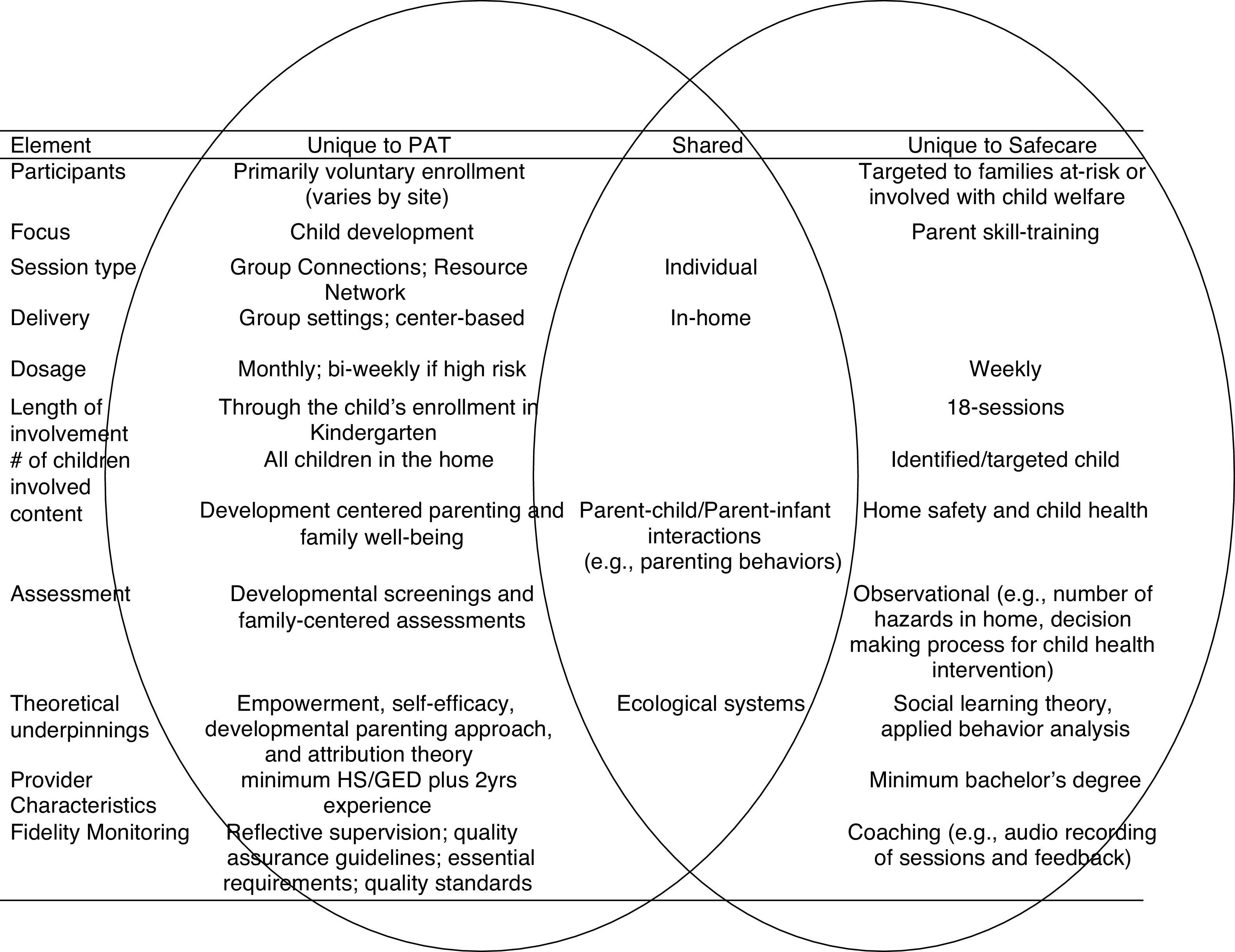
The term ‘braid’ was selected to reflect the manner in which the unique elements of the individual models are still apparent, but also overlap. Fig. 1 depicts elements unique to the PAT and SafeCare models, respectively, as well as highlights shared elements. Aspects in the shared column are found in both models and not listed additionally under each model. For example, both models are provided in-home, but the PAT model also includes group settings and the option for center-based delivery. Details of curriculum development were described elsewhere (Guastaferro et al., 2017).

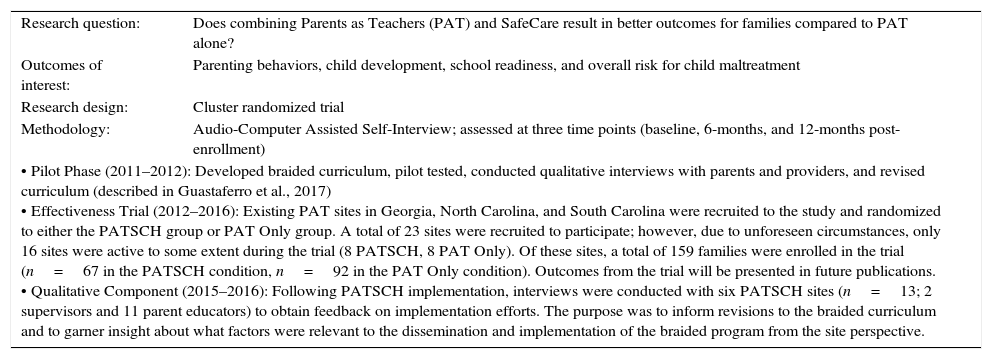
Research design: The project was funded by the Annie E. Casey Foundation {excluded for blind review} and administered by a research team at Georgia State University {excluded for blind review}. All research was approved by the University Institutional Review Board. An overview of the research design and methodology for the effectiveness trial is described in Table 1 for the context of the lessons learned.
Overview of research question, design, and methodology.
| Research question: | Does combining Parents as Teachers (PAT) and SafeCare result in better outcomes for families compared to PAT alone? |
| Outcomes of interest: | Parenting behaviors, child development, school readiness, and overall risk for child maltreatment |
| Research design: | Cluster randomized trial |
| Methodology: | Audio-Computer Assisted Self-Interview; assessed at three time points (baseline, 6-months, and 12-months post-enrollment) |
| • Pilot Phase (2011–2012): Developed braided curriculum, pilot tested, conducted qualitative interviews with parents and providers, and revised curriculum (described in Guastaferro et al., 2017) • Effectiveness Trial (2012–2016): Existing PAT sites in Georgia, North Carolina, and South Carolina were recruited to the study and randomized to either the PATSCH group or PAT Only group. A total of 23 sites were recruited to participate; however, due to unforeseen circumstances, only 16 sites were active to some extent during the trial (8 PATSCH, 8 PAT Only). Of these sites, a total of 159 families were enrolled in the trial (n=67 in the PATSCH condition, n=92 in the PAT Only condition). Outcomes from the trial will be presented in future publications. • Qualitative Component (2015–2016): Following PATSCH implementation, interviews were conducted with six PATSCH sites (n=13; 2 supervisors and 11 parent educators) to obtain feedback on implementation efforts. The purpose was to inform revisions to the braided curriculum and to garner insight about what factors were relevant to the dissemination and implementation of the braided program from the site perspective. | |
The braided curriculum was developed, tested, and revised in the Pilot Phase. The braided curriculum had four sessions per module, two of which were braided. Braided sessions included three areas of emphasis from the PAT model (i.e., developmental parenting, family well-being, and parent–child interactions) such that sessions met the essential requirements specified by PAT. Following the Pilot Phase, the Effectiveness Trial began at existing PAT sites. The study was implemented in three states and examined the effect of PATSCH compared to PAT alone with regard to parenting behaviors and overall risk for child maltreatment. Randomization occurred at the site level to avoid contamination within sites. Parent educators at all sites were asked to approach families who met at least two of the inclusion criteria (e.g., low income, low educational attainment, teen parent, single parent, or non-native English speaking) with the opportunity to participate in the research project. Families who did not participate continued their involvement with PAT. Families who decided to participate were consented by local data collectors and completed research assessments at 3 time points: baseline, 6-months post-enrollment, and 12-months post-enrollment. After PATSCH sites finished delivering the PATSCH curriculum, two members of the research team interviewed parent educators and supervisors at six sites who actively implemented PATSCH during the Effectiveness Trial. Though there were eight PATSCH sites active during the trial, only six had staff and funding at the end of the Effectiveness Trial (e.g., it was not possible to contact the parent educators and supervisors at two of the PATSCH sites). All parent educators and supervisors at the 6 PATSCH sites (n=13) were invited and agreed to participate in the interviews. Complete demographic information was not collected as part of the interview; the rationale being that demographic information on the parent educators was collected as part of the effectiveness trial. Because demographic information was not collected for the supervisors, and, as such, demographic characteristics would be incomplete, the demographic characteristics of interviewees is not presented here. However, as part of an introduction to the interviewers, and to contextualize comments, participants shared their years of experience as a provider/supervisor; the average number of years of experience was 11 years (range: 3–17 years). All interviewees were female.
The purpose of the interviews was to discuss PATSCH specific implementation successes and challenges. The interviews were conducted soon after the parent educators completed implementing the curriculum, prior to completing the outcome assessments, so as to capitalize on their experience. The semi-structured interviews were conducted in groups at each site, lasted approximately one hour, were audio recorded, and transcribed verbatim. Using a combination of the grounded theory (Corbin & Strauss, 2008) and phenomenological (Larkin, Watts, & Clifton, 2006) approaches, the interviews were coded thematically by the interviewers resulting in the organization of the lessons learned described below.
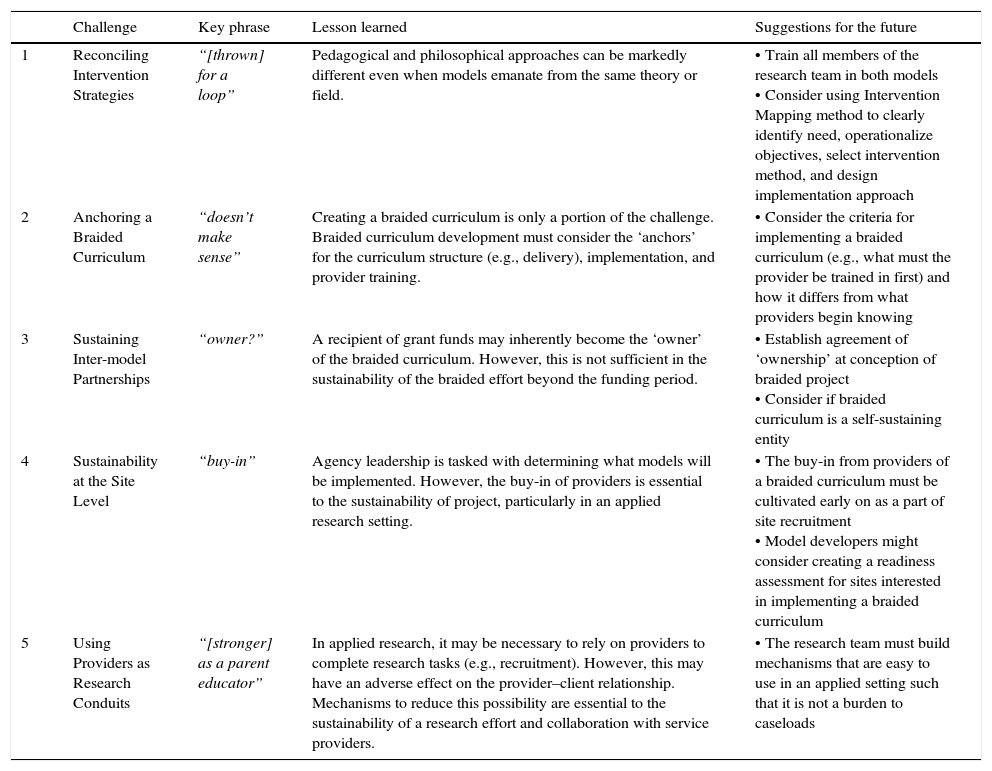
Discussion: lessons learnedWe identified five key lessons learned from this novel implementation endeavor. In this section we discuss the context of these implementation lessons learned and suggest future solutions to these challenges. These lessons learned span multiple implementation levels (e.g., provider, site, model); as such, though Lessons 3 and 4 do not have direct quotes from the interviewees as the other 3 lessons do, all lessons described here are directly informed by the interviews. A comprehensive list of lessons learned and offered solutions are presented in Table 2.
List of challenges, lessons learned, and suggestions.
| Challenge | Key phrase | Lesson learned | Suggestions for the future | |
|---|---|---|---|---|
| 1 | Reconciling Intervention Strategies | “[thrown] for a loop” | Pedagogical and philosophical approaches can be markedly different even when models emanate from the same theory or field. | • Train all members of the research team in both models • Consider using Intervention Mapping method to clearly identify need, operationalize objectives, select intervention method, and design implementation approach |
| 2 | Anchoring a Braided Curriculum | “doesn’t make sense” | Creating a braided curriculum is only a portion of the challenge. Braided curriculum development must consider the ‘anchors’ for the curriculum structure (e.g., delivery), implementation, and provider training. | • Consider the criteria for implementing a braided curriculum (e.g., what must the provider be trained in first) and how it differs from what providers begin knowing |
| 3 | Sustaining Inter-model Partnerships | “owner?” | A recipient of grant funds may inherently become the ‘owner’ of the braided curriculum. However, this is not sufficient in the sustainability of the braided effort beyond the funding period. | • Establish agreement of ‘ownership’ at conception of braided project • Consider if braided curriculum is a self-sustaining entity |
| 4 | Sustainability at the Site Level | “buy-in” | Agency leadership is tasked with determining what models will be implemented. However, the buy-in of providers is essential to the sustainability of project, particularly in an applied research setting. | • The buy-in from providers of a braided curriculum must be cultivated early on as a part of site recruitment • Model developers might consider creating a readiness assessment for sites interested in implementing a braided curriculum |
| 5 | Using Providers as Research Conduits | “[stronger] as a parent educator” | In applied research, it may be necessary to rely on providers to complete research tasks (e.g., recruitment). However, this may have an adverse effect on the provider–client relationship. Mechanisms to reduce this possibility are essential to the sustainability of a research effort and collaboration with service providers. | • The research team must build mechanisms that are easy to use in an applied setting such that it is not a burden to caseloads |
Lesson 1: Reconciling intervention approaches: Even when evidence-based programs have overlapping program goals and similar theoretical foundations, the introduction of additional constructs may create a marked difference in the implementation of the intervention (e.g., Empowerment or Attribution Theory specific to PAT and Social Learning Theory/Applied Behavior Analysis specific to SafeCare). In proposing this braided curriculum, we assumed the common program delivery mode and goals would facilitate the integration of the curricula; the PAT providers would simply deliver new content, not necessarily change the manner in which they interacted with families. This was true to some extent, however, the way in which content was taught was also different and required consideration.
The SafeCare behavioral intervention involves skill training with ongoing behavioral assessments that inform providers about parents’ mastery of the skills. For example, in the Safety module, the provider uses a structured checklist to count the number of accessible hazards in homes. It became clear that the differences in approaches were greater than anticipated. PAT does not typically conduct formal assessments of parenting behaviors via a standardized assessment form. Instead, the pedagogical approach is didactic and modeling oriented. The utilization of new intervention approaches in the braided curriculum made PATSCH providers uneasy in training because it was a shift in the manner they interacted with their families, though this unease diminished with time.
Maintaining intervention fidelity and ensuring the intervention is delivered as designed is key to maximizing potential benefits (Aarons et al., 2011; Metz & Bartley, 2012; Schoenwald et al., 2011). Fidelity is especially important when combining two interventions that conceptualize fidelity differently. For SafeCare, fidelity is assessed by observing (or listening via audio recording) how a given module is delivered during sessions. For PAT, fidelity is not assessed through direct observation, but through broader fidelity measures, referred to as Essential Requirements that target leadership/staffing, service provision (e.g., reflective supervision in which parent educators process the manner in which their emotional responses affect the services being delivered; Parlakian, 2002), and evaluation as well as Quality Standards (e.g., implementation standards). The audio recording and coaching sessions used in SafeCare standard delivery were directly applied to PATSCH. The introduction of the audio recordings of home sessions for fidelity monitoring was a challenge, and as one parent educator put it, “threw [parent educators and families] for a loop.”
The lesson learned is that in developing a braided curriculum, more than the content and theoretical orientation must be considered. The objectives of a braided curriculum must be operationalized and aligned with intervention and implementation strategies representative of the two models being braided, but specific to the braided curriculum. This balance requires structured compromise. Powell and colleagues (2015) offer suggestions as to how disparate implementation strategies between two curricula could be selected and tailored. The Intervention Mapping approach balances theory, evidence, and stakeholder perspectives. It involves a needs assessment, operationalization of program objectives, matching of intervention methods to those objectives, and the design of an implementation strategy (Bartholomew, Markham, Mullen, & Frenandez, 2015; Powell, Beidas, et al., 2015). Though we did not use this approach in our braided approach, it is likely that it may be useful in future efforts to braid existing curricula.
Lesson 2: anchoring a braided curriculum: The development of a braided curriculum requires the actual braiding of models, but also must consider the foundation, or the ‘anchor’, for the new product. This differs from the intervention style because anchoring focuses on how the provider might use the braided curriculum. PAT functioned as the ‘delivery anchor’, or the common starting point, for all PATSCH providers because the parent educators were already trained in and implementing PAT, and SafeCare was implemented within the context of a PAT service. The PATSCH curriculum utilized the SafeCare manualized session structure as the ‘implementation anchor’ (see Guastaferro et al., 2017 for an example of session outlines). The implementation of PATSCH required some parent educators to alter considerably their interactions and involvement with the families they served. This may have included a combination of one or more of the following factors: an increase in the frequency with which they visited families (e.g., transitioning from visiting once-a-month to bi-weekly); audio recording sessions for fidelity; and, introducing a session structure focused on training behaviors, thus differing from parent-directed conversation (e.g., pedagogical approach of applied behavior analysis compared to Empowerment Theory).
The function of PAT as the delivery anchor and SafeCare as the implementation anchor was discussed by parent educators in our qualitative interviews as what we have called an “anchoring mismatch.” There was an apparent disconnect for the providers between how and what they were trained to do in PAT and what they learned to do in PATSCH. One parent educator with particularly strong feelings of disconnect even stated: “The braid doesn’t work. There are similar goals, but different approaches.” Planned anchoring and implementation support built around the anchor may reduce this friction in future braided efforts.
Lesson 3: sustainability of a braided curriculum: Braiding inherently requires the cooperation and collaboration of two models beyond the provider level. The comments of the parent educators, as evident in excerpts shared in Lessons 1 and 2, emphasized the importance of determining ‘ownership’ of the braided curriculum. This is related to the delivery anchor: a PAT site could adopt PATSCH, whereas a SafeCare site could not. In our case, funding support necessitated that staff at National SafeCare Training and Research Center take the lead on much of the work utilizing input and resources provided by the PAT National Center. PATSCH is conceptually a coordinated effort by SafeCare and PAT, but the sustainability of the model requires consideration of which model takes leadership in pursuing further funding to improve the evidence-base. Cooperative agreements and memoranda of understanding are practical solutions, but sustainability in this context extends to intellectual property where the boundaries become blurred. In the context of PATSCH specifically, our team considered the following questions: does PATSCH exist as a self-sustaining entity? Or, because it relies on provider experience in PAT does it exist as a component of PAT? Or, because some of the added content is specific to SafeCare, is PATSCH an adaptation of SafeCare? Though our models have not yet collectively reached a solution to this important lesson at the time of writing, we suggest that future braided efforts establish this agreement at inception of such an effort.
Lesson 4: building sustainability at the site level: Successful implementation of any curriculum is dependent on buy-in by providers (Metz & Bartley, 2012). During the Pilot Phase, the initial conversations about the braided curriculum at some sites were with site supervisors and with supervisors and providers at others (Guastaferro et al., 2017). Of the two pilot sites trained in PATSCH, the one site that was recruited through conversation with only site supervisors discontinued participation following the Pilot Phase because of the perceived added time commitment to their already high caseloads. In contrast, the pilot site that was recruited through conversations with both the supervisor and parent educators remained active in the Effectiveness Trial. This provided us with a valuable lesson that we carried forward in the process of recruiting other sites, being sure to discuss the requirement with supervisors and staff. Providers are most familiar with their caseloads, potential participants, and whether their families would benefit from the braided curriculum. In typical SafeCare implementation a readiness assessment, a tool commonly used in implementation science, is conducted with interested sites. Future braided efforts may benefit from developing a readiness assessment specific to the implementation of a braided curriculum.
Lesson 5: impact of research on provider–client relationship: Our trial was not possible without the assistance of the parent educators at control and PATSCH sites. They became the conduits of the family enrollment aspect of the research project, a task they were not necessarily familiar with and which they were not necessarily comfortable. Third party data collectors administered the research assessments which included a computer questionnaire, a video recorded parent–child interaction, and environmental scan of two rooms. At least some parent educators believed use of video for the research negatively affected their relationships with families, some of whom they had been serving for some years. One parent educator shared the effect of PATSCH, specifically the research assessments, on her relationship with a family: “When I started talking about filming, um for the safety part… it scared her. As a matter of fact, ever since then we have met here at the school. She has not even wanted [me] in her home ever since then.” Other parent educators described the positive effect on families: “I see families all the time that, I just feel like I can use that Safety and Health piece all the time.” Parent educators also shared how parents positively responded to aspects of the braided curriculum, such as Safety: “I was walking around the house and showing them… a little detail that they never thought about before. They were really more careful about things around their house.”
The lesson is the introduction of research into the dynamic between service provider and family may be positive or negative and it is the responsibility of the researchers to reduce negative impacts as much as possible. Overall, parent educators had a positive take on their involvement:
“PATSCH has helped me learn how to approach them about safety concerns in the home, how to talk about the importance of a medical provider, how to support them through noticing and observing health crises, and trying to identify health concerns earlier...it's strengthened me as a parent educator...”
ConclusionThe objective of this paper was to describe the lessons learned from the implementation of a braided curriculum with the goal of informing future braiding efforts. Braiding offers one potential solution to better meet the comprehensive needs and improve the well-being of children and families. Of course, neither PATSCH nor any other program will meet the needs of all families. There has been very little systematic work to understand which programs are most effective for particular kinds of families based on risk factors, needs, or even expressed desires.
Although the results of the Effectiveness Trial described here are forthcoming, there is a burgeoning interest in the concept of braided efforts and the braided approach is increasingly supported by researchers, model developers, and funders (Guastaferro et al., 2017). However, an alternative perspective on combining curricula is worth noting. This perspective may be called the “less is more” approach. Some have argued that programs with a few specific intervention targets will ultimately be more effective and successful than broader programs (Berliner et al., 2015). It may not be possible to address every need a family may have, especially for very high risk families such as those in the child welfare system. There are obvious resource issues: more intervention costs more money and families may only tolerate a degree of intervention before they burn out and/or drop out. It could be that the development of new skills in a few key areas fosters families’ ability to learn other skills on their own. There is a body of data, at least related to parenting, that indicates more intervention detracts from program effectiveness (Bakermans-Kranenburg, van IJzendoorn, & Juffer, 2003; Kaminski, Valle, Filene, & Boyle, 2008). Further research to this end is warranted.
The research on braided programs is nascent. In the development of PATSCH we relied to some degree on intuition. A more effectively braided curriculum might be developed with more empirical data. We do not know which, if any, of the components that comprise PATSCH directly affect outcomes. An emerging framework to provide that empirical evidence is the multiphase optimization strategy (MOST). The goal is to engineer an optimized behavioral intervention that meets predetermined standards (expressed as an optimization criterion), is efficient (i.e., makes good use of resources), and is scalable with impact on outcomes of interest (Collins, Kugler, & Gwadz, 2016; Collins, Nahum-Shani, & Almirall, 2014). Examples of fields in which MOST has been applied include smoking cessation (Baker et al., 2015), substance use and sexual risk prevention (Caldwell et al., 2012), weight loss (Pellegrini, Hoffman, Collins, & Spring, 2014, 2016), and regulation of gestational weight gain (Dong et al., 2013). MOST is directly applicable to the objectives of PATSCH: to develop a parent-support intervention that brings together components from two evidence-based programs to better address multiple risk factors. Future research might apply the MOST framework to the concept of braiding.
Ultimately, the goal is to provide the most effective intervention to each family (Gardner, 2016). Ideally, we would have research and assessments to determine which interventions would do that based on family profiles, risk, demographics, or preferences. However, the field of maltreatment prevention has not yet reached that level of sophistication and it is clear that no single program is a best fit for every family. Strategies such as braiding, the “less is more” approach, and MOST provide frameworks for determining next steps in intervention development and evaluation as we seek to provide better services for families.
FundingThe research was supported by the Annie E. Casey Foundation. During the preparation of the manuscript for publication, K. Guastaferro was supported by award T32 DA 017629 and P50 DA 039838 from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of The National Institute on Drug Abuse.
Conflicts of interestThe authors have no conflicts of interest to declare.
We would like to thank Maithili Bhat and Ambra Noble for their help transcribing the interviews, and Jon Reader for reviewing an early draft of the manuscript.
