








Pregnancy loss is a common medical problem in reproductive-age as more than fifty percent of human pregnancies are aborted before term. The majority are unrecognized occurring before or with the expected next menses. About 10–12 percent of all clinically diagnosed pregnancies are lost as first-trimester or early second trimester. The rate of fetal death after 14 weeks’ gestation is much lower than the rate of pre-embryonic and embryonic loss. CA125 is a member of the mucin family glycoproteins. CA125 has found application as a tumor marker or biomarker that its level may be increased in the serum of some patients with specific types of cancers. Some studies detected that the abortion risk is increased in pregnant women with higher CA125 levels. Progesterone belongs to the C21 group of progestogen. Its main source in humans is the corpus luteum.
Human chorionic gonadotropin (HCG) is a glycoprotein produced by syncytiotrophoblast.
Aim of the workThe aim of this study was to determine the effectiveness of measuring maternal serum β-HCG, progesterone, CA125 in prediction of first trimester abortion.
PatientsThe study included 90 pregnant women attending the ANC clinic in El-Shatby Maternity University Hospital. Patients were divided equally into two groups: Group I: 45 women with threatened abortion, subdivided into 2 subgroups: Subgroup A – Cases ended in abortion; Subgroup B – Cases continued as normal pregnancies. Group II: 45 pregnant women with normal pregnancy and were further subdivided into two subgroups: Subgroup C – Cases ended in abortion; Subgroup D – Cases continued as normal pregnancies.
Exclusion criteria(1) Multiple pregnancies; (2) Anembryonic pregnancy; (3) Pregnant women with prior treatment with progesterone; (4) History of endometriosis; (5) Fibromyoma with pregnancy.
MethodsAfter clinical and sonographic examination, 3mL venous blood have been taken once for estimation of serum level of β-hCG, progesterone and CA125 by quantitative ELISA.
ResultsThis is a case–control study. Out of the 90 pregnancies, 15 cases (16.6%) had aborted during follow-up, 9 cases (60%) of them had history of threatened abortion while 6 cases (40%) had no history of threatened abortion. Regarding Serum Progesterone level between studied groups, the calculated p value was <0.001. For Serum β HCG, the calculated p value was <0.001. In Serum CA125 the calculated p value was <0.001.
A perda da gravidez é problema clínico comum em mulheres em idade fértil, pois em mais de 50% das gestações humanas ocorre aborto antes do termo. Em sua maioria, tais abortos passam despercebidos; ocorrem antes da próxima menstruação ou juntamente com a próxima menstruação. Cerca de 10-12% de todos os abortos clinicamente diagnosticados ocorrem no primeiro trimestre ou no início do segundo trimestre. O percentual de mortes fetais após 14 semanas de gestação é muito mais baixo do que o percentual de abortos pré-embrionários ou embrionários. Foi constatado que CA125 tem aplicação como marcador tumoral ou como biomarcador, pois seu nível pode aumentar no soro de alguns pacientes portadores de tipos específicos de neoplasias. CA125 é um membro da família das glicoproteínas mucinas. Alguns estudos observaram que o risco de aborto aumenta em gestantes com níveis mais elevados de CA125. Progesterona pertence ao grupo C21 dos progestágenos. Em seres humanos, sua principal fonte é o corpo lúteo. Gonadotrofina coriônica humana (HCG) é uma glicoproteína produzida pelo sinciciotrofoblasto.
ObjetivoDeterminar a eficácia da determinação, no soro materno, de β-HCG, progesterona e CA125 na previsão do aborto no primeiro trimestre.
PacientesO estudo abrangeu 90 gestantes atendidas na clínica ANC na Maternidade do Hospital Universitário El-Shatby. As pacientes foram divididas equitativamente em dois grupos. Grupo I: 45 gestantes com ameaça de aborto, subdivididas em dois subgrupos: Subgrupo A – Casos que terminaram em aborto; Subgrupo B – Casos que tiveram continuidade como gestações normais. Grupo II: 45 gestantes com gestação normal, subdivididas em dois subgrupos: Subgrupo C – Casos que terminaram em aborto; Subgrupo D – Casos que tiveram continuidade como gestações normais.
Critérios de exclusão1. Gestações múltiplas; 2. Gestação anembriônica; 3. Gestantes previamente tratadas com progesterona; 4. História de endometriose; 5. Fibromioma com gestação.
MétodosApós exame clínico e ultrassonográfico, 3mL de sangue venoso foram coletados uma vez para estimar o nível sérico de β-hCG, progesterona e CA125 por Elisa quantitativo.
ResultadosEste é um estudo de casos-controle. Das 90 gestações, durante o seguimento ocorreram 15 (16,6%) casos de aborto; nove (60%) tinham história de ameaça de aborto, seis (40%) não tinham história de ameaça de aborto. Com relação ao nível sérico de progesterona entre os grupos estudados, calculamos p<0,001. Para o nível sérico de CA125, calculamos p<0,001.
Pregnancy loss is a common medical problem in reproductive-aged females, with around 25 percent of all women attempting pregnancy experiencing at least one spontaneous abortion. Medically, all pregnancy losses before 20 weeks’ gestation termed as abortion.1,2
More than fifty percent of human pregnancies are aborted before term. The majority are unrecognized occurring before or with the expected next menses. About 10–12 percent of all clinically diagnosed pregnancies are lost as first-trimester or early second trimester. The rate of fetal death after 14 weeks’ gestation is much lower than the rate of pre-embryonic and embryonic loss.3
Sporadic abortion is the commonest adverse outcome in human reproduction. In the majority of sporadic spontaneous abortions, an etiology is unknown. A spontaneous abortion or miscarriage are expected to occur in 15–25 percent of all pregnancies.4
CA125 (cancer antigen 125 or carbohydrate antigen 125) also known as mucin 16 or MUC16. MUC16 is a member of the mucin family glycoproteins. CA125 has found application as a tumor marker or biomarker that its level may be increased in the serum of some patients with specific types of cancers, or other benign conditions.5
There are two theories explaining the rise of maternal serum CA125 in the first trimester. The most accepted one is the tubal reflux theory of Quirk et al. According to this theory, CA125 with decidual origin passes to maternal compartment via tubal reflux and rises in the circulation after the absorption by peritoneal lymphatics. As the pregnancy proceeds, a functional obstruction occurs due to the fusion of deciduas capsularis and deciduas parietalis in tuba uterine, and serum CA125 levels decrease.6
The second theory is explained as the crossing of CA125 to the maternal blood circulation due to damage in decidual cells occurred by chorionic villus invasion in early pregnancy and by placental separation at birth.7
Some studies detected that the abortion risk is increased in pregnant women with higher CA125 levels.
Progesterone belongs to the C21 group of progestagen. Its main source in humans is the corpus luteum. After conception, corpus luteum is supported by secretion of human chorionic gonadotropin (HCG), and produces progesterone until the 10th gestational week. After a transition period by 7–10 gestational weeks the placenta becomes the major source of progesterone.8
Human chorionic gonadotropin (HCG) is a glycoprotein produced by syncytiotrophoblast. It has a molecular weight of 36–40kDa and is biologically and immunologically similar to LH but with a longer half-life.9
Although its main function is to maintain the corpus luteum, the fetal testis is a target organ for hCG. It is largely responsible for the early development of the fetal testis and for testosterone production prior to fetal LH control.9
Aim of the workThe aim of this study was to determine the effectiveness of measuring maternal serum β-HCG, progesterone, CA125 in prediction of first trimester abortion.
PatientsThe study included 90 pregnant women attending the antenatal care clinic of El-Shatby Maternity University Hospital.
All cases signed a well informed written consent to declare their agreement to be enrolled in this study, as agreed upon by the ethical committee.
The patients were divided equally into two groups:
45 pregnant women with threatened abortion those were further subdivided into 2 subgroups:
Subgroup ACases ended in abortion including missed abortion, complete abortion and inevitable abortion.
Subgroup BCases continued as normal pregnancies where pregnancies did not end in abortion.
N.B.All cases of group I who presented by threatened abortion were advised to physical and mental rest and prescribed natural progesterone 400μg in the form of vaginal pessaries once daily for 5 days.
Group II45 pregnant women with normal pregnancy and were further subdivided into two subgroups:
Subgroup CCases ended in abortion including missed abortion, complete abortion and inevitable abortion.
Subgroup DCases continued as normal pregnancies where pregnancies did not end in abortion.
Inclusion criteria- (1)
Any gravidity and parity.
- (2)
Maternal age between 20 and 35 years.
- (3)
Gestational age between 5 and 13 weeks.
- (4)
Singleton pregnancy.
- (1)
Multiple pregnancies.
- (2)
Anembryonic pregnancy.
- (3)
Pregnant women with prior treatment with progesterone.
- (4)
Heavy smokers.
- (5)
Diabetes mellitus.
- (6)
Renal, trophoblastic and thrombophilic diseases.
- (7)
History of endometriosis.
- (8)
Fibromyoma with pregnancy.
All cases have been subjected to the following:
HistoryPersonal, Obstetric history, Medical and Surgical history: to exclude general and systemic diseases.
Examination and investigationsTransvaginal ultrasonographic scanning to:
- o
Assess fetal measurements, and exclude multiple pregnancies, vesicular mole and ectopic pregnancy.
- o
Assess placental site and to exclude retroplacental hemorrhage and collection.
3mL venous blood have been taken once and sent to the laboratory for estimation of serum level of β-hCG, progesterone and CA125 by quantitative enzyme linked immunoassay.10
Group IAt time of first admission.
Group IIBetween 5 and 13 weeks of gestation.
ResultsThis is a case–control study that was conducted on ninety pregnant women between 5 and 13 weeks of gestation.
Out of the 90 pregnancies, 15 cases (16.6%) had aborted during follow-up, 9 cases (60%) of them had history of threatened abortion while 6 cases (40%) had no history of threatened abortion.
Serum progesteroneIt might be seen from Table 1 that comparing the study groups regarding serum progesterone, the calculated means were 9.9 with standard deviation of 0.7 in group A, 28.3 with standard deviation of 4.5 in group B, 13.2 with standard deviation of 0.9 in group C 27.3 with standard deviation of 4.1 in group C, the calculated p value was <0.001, so there is a statistical significance.
Serum β HCGIt might be seen from Table 2 that comparing the study groups regarding serum β HCG, the calculated means were 10,450.6 with standard deviation of 1710.5 in group A, 27,375.9 with standard deviation of 5987.0 in group B, 16,456.3 with standard deviation of 2451.6 in group C and 41,876.1 with standard deviation of 4231.7 in group C, the calculated p value was <0.001, so there is a statistical significance.
Serum beta hCG in Group I, II and subgroups.
| S. beta HCG mIU/ml | Group I | Group II | F (P) | ||
|---|---|---|---|---|---|
| Aborted (A) | Completed (B) | Aborted (C) | Completed (D) | ||
| Range | 9120.0–1311.5 | 21,900.0–34,760.0 | 12,120.4–19,769.0 | 35,980.0–98,710.0 | 95.2 (0.001) |
| Mean±SD | 10,450.6±1710.5 | 27,375.9±5987.0 | 16,456.3±2451.6 | 41,876.1±4231.7 | |
It might be seen from Table 3 that comparing the study groups regarding serum CA125, the calculated means were 20.9 with standard deviation of 0.6 in group A, 42.3 with standard deviation of 4.8 in group B, 32.7 with standard deviation of 1.2 in group C and 60.8 with standard deviation of 3.1 in group C, the calculated p value was <0.001, so there is a statistical significance.
Specificity and sensitivity of serum progesterone, β-hCG and CA 125 in prediction of first trimester abortionRegarding serum progesterone in prediction of first trimester abortion the calculated sensitivity and specificity at a cut-off value of 23ng/ml were 90.14 and 88.76 respectively, as shown in Table 4.
As shown in Table 5, the calculated sensitivity and specificity of β-hCG at a cut-off value of 20,555mlIU/ml were 79 and 85.17, respectively.
On the other hand the calculated sensitivity and specificity of CA125 at a cut-off value of 51.68U/ml were 88.11 and 79.31 respectively, this was shown in Table 6.
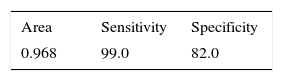
As shown in Table 7, the combined sensitivity and specificity of the three biomarkers for prediction of first trimester abortion were 99.00 and 82.00 respectively.
DiscussionHCG has been used alone or in combination with progesterone, oestradiol, testosterone, CA125, Human Placental Lactogen (HPL) and ultrasonography in other studies in the determination of the prognosis of threatened abortion.11
As in the study of Mehmet et al.12 the relationship between abortion and lower β-HCG levels were shown in many studies. In agreement with the previous studies, we also found β-HCG levels significantly lower in the group with abortion than that of the group where no abortion was detected. When it is considered that β-HCG is released from trophoblasts, it is easier to explain the low β-HCG levels in the cases of in the cases of inevitable, complete and incomplete abortion.12
Darwish et al.13 in a prospective controlled study of using bio-chemical marker in the prediction of pregnancy outcome in cases with recurrent pregnancy loss, they found that progesterone is not significant in the prediction of pregnancy outcome at 6–7th week in a study of pregnant women from 6–11th week of gestation with a sensitivity and specificity of 43%, 50% respectively. PPV and NPV are of 38%, 56% respectively.13
Altay et al.14 in a prospective study of 99 pregnant women at the 10th week of pregnancy with the use of Crown Rump Length (CRL), Fetal heart rate and progesterone as a predictor of spontaneous abortion risk found that Crown Rump Length (CRL) and serum progesterone could predict patients with low abortion risk.14
Moreover, we found that progesterone is also an independent factor on abortion as β-HCG in our analysis. In addition, since we have detected a correlation between β-HCG and progesterone in detecting abortion.
Hanita et al. (2012) in their study a 95 pregnant women of 13 weeks or less period of amenorrhea were recruited. Fourteen normal pregnant women were controls. Progesterone levels were significantly lower in threatened abortion patients with outcomes of nonviable pregnancy compared with pregnancies that progressed on to the viability period 23.3±12.0 vs. 89.7±33.2 respectively, p<0.001. At cut-off value of 32.7ng/mL, progesterone had 90% sensitivity with 75% negative predictive value and 92% specificity with 97% positive predictive value.15
The high cutoff level value in comparison to our study may be due to therapeutic usage of progesterone.
Duan et al.16 in their study including 245 women from which 175 were threatened abortion and 70 were control. They concluded that progesterone combined with Beta hCG measurement may be useful for predicting outcome of threatened abortion.16
Contrary to the studies indicated previously, other studies found the sensitivity of using β-HCG and progesterone together as 81% and the specificity of both as 99% in detecting abortions. As a result, it was detected that the use of the both β-HCG and progesterone together, instead of β-HCG or progesterone singly, does not provide additional benefit in terms of increasing the sensitivity value.17
In our study, we have found a positive correlation between β-HCG or progesterone in cases who have aborted, whereas, in cases who have completed their pregnancy there were no significant correlation.
For that reason, even although β-HCG is an independent factor, since β-HCG is used more frequently in determining the prognosis of trophoblast, ectopic pregnancy and threatened abortion, and is used more common in laboratories than progesterone, and since the kit of β-HCG is more expensive than either that of progesterone, it has been suggested that the use of progesterone alone in the detection of abortions in asymptomatic pregnancies will be more eligible.
Mahdi et al.18 in his study for estimation of CA-125 Level In first trimester threatened abortion. He concluded that CA-125 cannot be used as a predictor of outcome of early pregnancy complicated by vaginal bleeding. This study not supporting the results of our study but it is noted the small number of patients in the study and that may be a cause of different result from our study.18
On the other hand, we found a statistical difference, were the sensitivity was 88.11%, specificity was 79.31% and positive predictive value was. 73.05% at 51.68IU/mL.
Ayaty et al.19 in their study compared 50 women with healthy pregnancy and 50 women with threatened abortion of the level of CA 125 and followed up the outcome. The mean level of CA-125 in finally aborted patients was 58.17±7.25IU/mL and in normal pregnant women, who continue to term, was 26.61±1.76IU/mL. The CA-125 level in threatened women, whose pregnancy continued and did not abort, was 30.89IU/mL. They concluded that measurement of serum CA-125 may be an inexpensive, easily available, sensitive and specific predictor of outcome in threatened abortion, which results the loss of pregnancy. This study supports our study results.19
Maged and Al-Mostafa20 in their study. CA125, Beta hCG and progesterone are good biochemical markers and fetal heart rate (FHR) and Crown Rump Length (CRL) are good ultrasonographic markers for the prediction of outcome in women with threatened abortion. This study involving 250 women in their 1st trimester was divided into three groups: group I (65 women) in whom threatened abortion ended in abortion, group II (85 women) with threatened abortion who completed their pregnancy and group III (100 women) with normal pregnancy.20
There was a statistically significant difference between group 1 and the other two groups regarding CA 125, Beta hCG, progesterone, fetal heart rate (FHR) and Crown Rump Length (CRL). The sensitivity, specificity of CA 125 at 80IU/mL were 80.2% and 78.3%, respectively, for Beta hCG at 19,887mIU/mL were 88.6% and 81.1, respectively, for progesterone at 25ng/mL were 90.1% and 87.2%, respectively, for fetal heart rate (FHR) at 110bpm were 98.1%, and 99.1% respectively and for Crown Rump Length (CRL) at 21mm were 46.4%, and 40.1%, respectively. This study correlates our study results.
Based on the findings that free β-HCG and progesterone as independent variables demonstrated a similar statistically significant prediction on abortion, the single measurement of free β-HCG or progesterone levels can be useful in the prediction of first trimester spontaneous abortions according to clinician's choice. The use of progesterone may be recommended, since it has high availability and lower cost than free β-HCG.21
Finally our study found that Beta hCG, progesterone and CA 125 are significant in predicting pregnancy out come with a cutoff value of CA125U/mL, β HCG mIU/mL, Progesterone ng/ml which was (51.68, 20,555 and 23) respectively.
Conclusion- 1.
Reliable prediction of abortion in the first trimester could potentially improve pregnancy outcomes because it would allow closer prenatal monitoring, earlier diagnosis, and expeditious interventions.
- 2.
Measuring serum progesterone, Beta hCG and CA 125 in first trimester will give a good idea about the integrity of the pregnancy, a patient with higher Level of Beta hCG than 20,555mIU/mL and progesterone 23ng/mL and a lower level of CA125 than 51.68U/mL identifies patients at a very high risk for abortion, with a sensitivity of about 99% and a specificity of 82%.
- 1.
Potential benefits of any screening test are highest in populations at greatest baseline risk of disease; hence, women in the high-risk group for abortion would be ideal candidates for routine screening.
- 2.
Women at high risk for abortion should increase the frequency of their antenatal visits, to increase their surveillance and timely intervention, thus potentially improving both maternal and fetal outcome.
- 3.
Using the possibility of identification of risk of abortion prior to the onset of vaginal bleeding or any other signs, targeted studies of existing, controversial or novel treatment and preventive strategies should be undertaken.
- 4.
Further studies should be inducted including combinations of progesterone, CA125 or β HCG with other predictors of abortion to test the sensitivity and specificity of such combinations.
The authors declare no conflicts of interest.