



Group A streptococci (GAS) has been reported as an unusual cause of food-borne outbreaks in industrialized countries, causing pharyngitis and differing from air-borne outbreaks in that they begin abruptly and have low complications rate1.
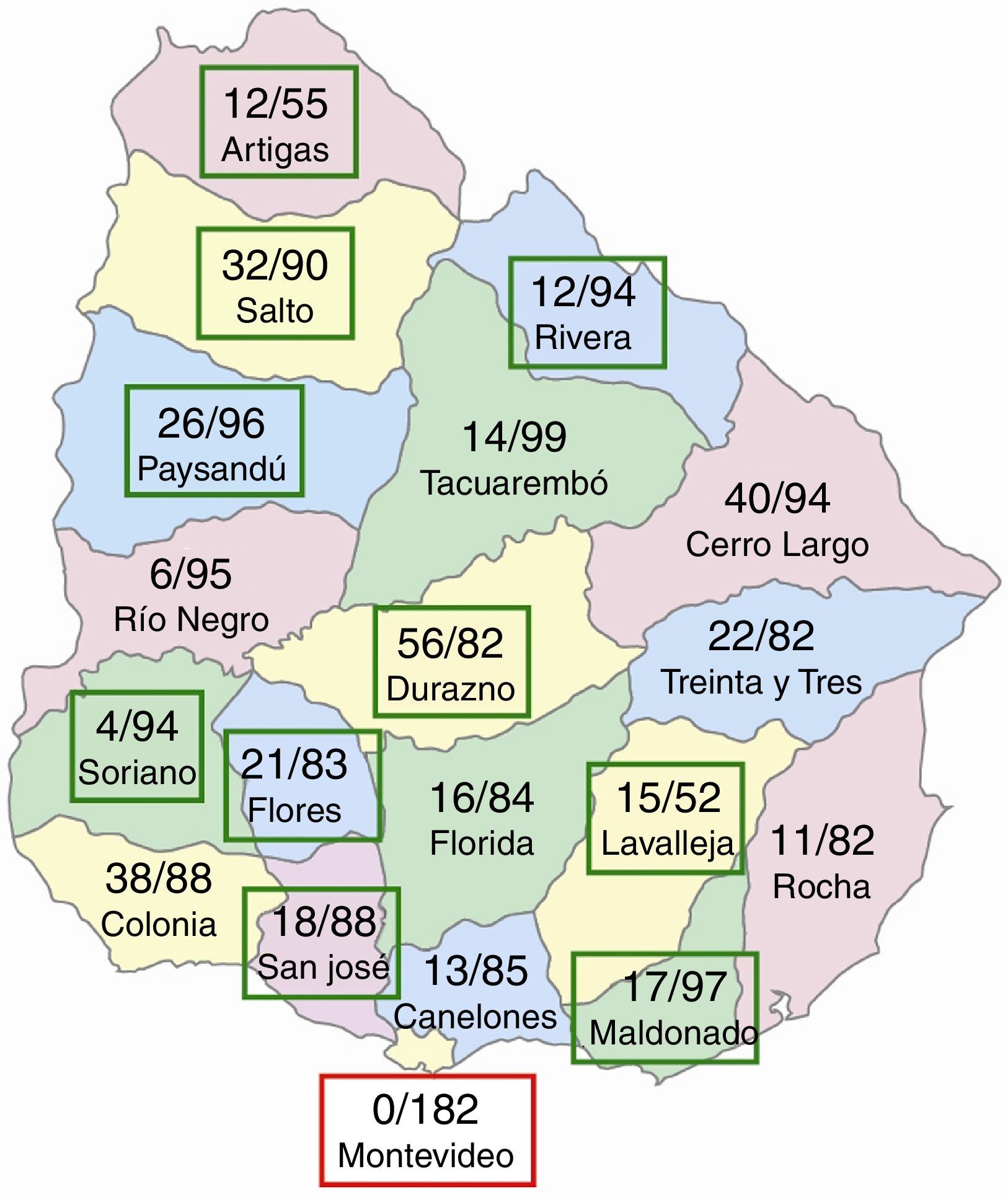
In November 2013, a large GAS outbreak was reported among 1702 young participants (15–20 years old) from all over the country who came to Montevideo, the capital city of Uruguay, for a sports competition (Fig. 1).

The competition started November 6th and 2 days later many competitors became ill and needed medical assistance. At least 374 patients with tonsillo-pharingitis were identified (attack rate 21.97%), most between November 8th and 9th. The affected competitors were staying together at the same facility but they participated in different sports, were from different geographic origins and slept in different rooms.
The epidemic curve suggested an outbreak by a common source, probably food-borne. The meal was provided by a catering service to all participants, except to those living in Montevideo. The epidemiological investigation showed that procedures for preparation, storing, transporting and handling of the dishes were not always according to regulations. One of six food handlers in place tested positive for rapid GAS antigen detection test. Unfortunately, the catering service was not investigated: no food samples were obtained and their food makers were not studied. Interestingly, none of the participants living in Montevideo became ill.
All symptomatic patients were treated with intramuscular penicillin and 2 were hospitalized for febrile seizures and bronchospasm respectively.
Most cases were only clinically diagnosed, thus only 20 GAS throat isolates from patients living in 10 different cities were available for characterization at our institution, the National Reference Laboratory (Fig. 1).
Penicillin, erythromycin, clindamycin, tetracycline, cloramphenicol and levofloxacin were tested using disk diffusion following the procedures of Clinical and Laboratory Standards Institute. The emm type was determined by sequencing the variable 5′-end of the emm gene, according to the Centers for Disease Control and Prevention.
PCR was used to detect speA, speC, speB and ssa genes as described previously4. PFGE was used to confirm the GAS similarity2 and two random selected isolates were studied by MLST5.
All GAS isolates were susceptible to the antibiotics tested. Indistinguishable PFGE profiles were obtained and only speB was identified in all isolates.
The 20 GAS isolates corresponded to emm type 68.3, a very rare serotype scarcely cited in literature. This emm type was not identified in a previous study of GAS invasive and non- invasive infections, among 135 isolates collected between 1999 and 2012 in Uruguay3. To our knowledge, emm68.3 has never been associated with food-borne streptococcal sore throat outbreaks before.
The isolates tested for MLST were ST247, which is represented by only 4 isolates in the MLST database5.
In summary, for the first time in Uruguay, a large outbreak of tonsillo-pharyngitis was recorded. This outbreak was caused by a single clone of group A streptococci emm68.3/ST247. Isolates from food were not available for comparison, but the epidemiological features suggest that food could be the source of infection.
