



To determine the degree of autonomy of patients treated with mechanical thrombectomy; to assess the degree of neurological deficit on admission and 24 h, and the degree of dependency at 3 months after performing the mechanical thrombectomy.
MethodQuantitative, observational, and descriptive study, with a sample of 57 patients treated with mechanical thrombectomy in the Autonomous City of Buenos Aires. Neurological deficit was measured with the National Institute of Health Stroke Score upon admission and 24 h after treatment with mechanical thrombectomy, and functional outcome with the modified Rankin scale at three months.
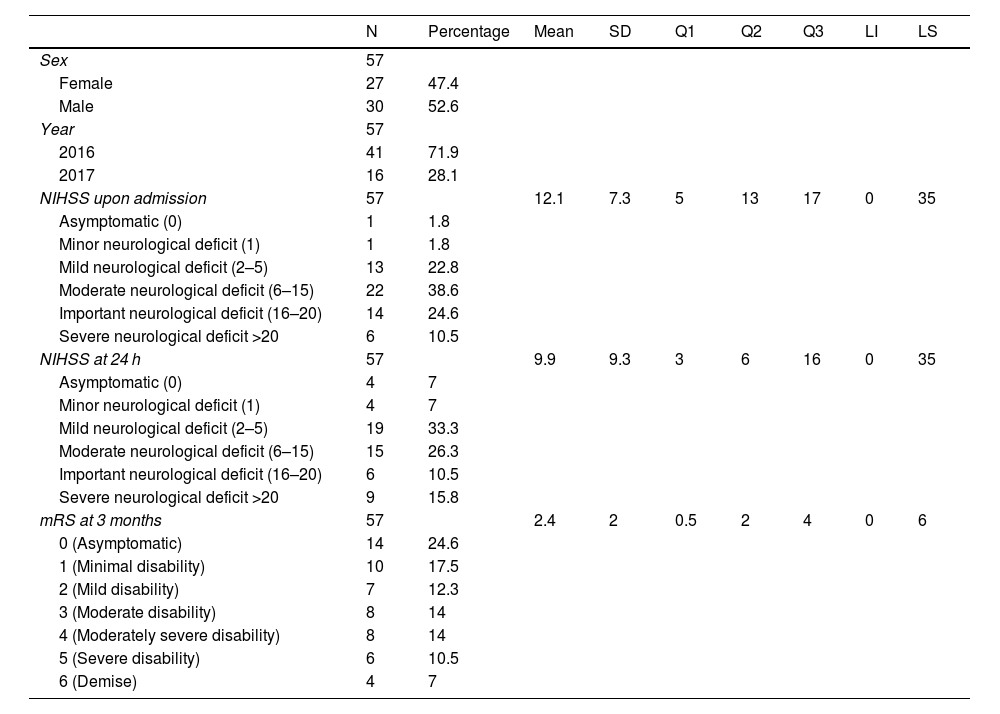
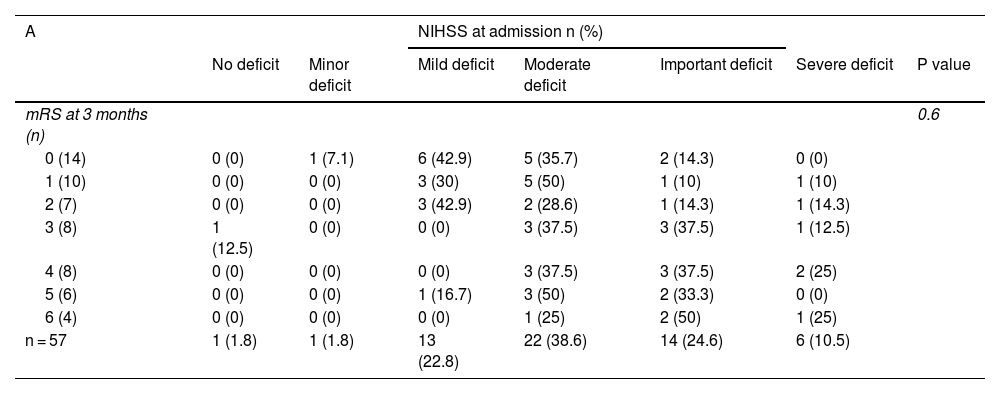
ResultsThe degree of dependency at three months was 2,4 points. The mean neurological deficit score on admission was 12,1 points, and 9,3 points after 24 h. Neurological deficit at 24 h has been found to be predictive of functionality at three months.
ConclusionThe mean of the neurological deficit at admission was situated in a moderate neurological deficit. The mean of the neurological deficit at 24 h has been placed in a moderate neurological deficit. The score for the degree of dependency at three months was placed in the mild disability category. A significant correlation has been obtained between the neurological deficit at 24 h and the functional result at three months.
Determinar el grado de autonomía de los pacientes tratados con trombectomía mecánica; evaluar el grado de déficit neurológico al ingreso y a las 24 horas y el grado de dependencia a los tres meses tras la realización de la trombectomía mecánica.
MétodoEstudio cuantitativo, observacional y descriptivo, con una muestra de 57 pacientes tratados con trombectomía mecánica en la Ciudad Autónoma de Buenos Aires. El déficit neurológico ha sido medido con la National Institute of Health Stroke Score al ingreso y tras las 24 horas del tratamiento con trombectomía mecánica y el resultado funcional con la escala de Rankin modificada a los tres meses.
ResultadosEl grado de dependencia a los tres meses se ha situado en 2,4 puntos. La puntuación media del déficit neurológico al ingreso ha sido de 12,1 puntos, a las 24 horas de 9,3 puntos. El déficit neurológico a las 24 horas ha resultado ser predictivo de la funcionalidad a los tres meses.
ConclusiónLa puntuación media del déficit neurológico al ingreso se ha situado en un déficit neurológico moderado. La puntuación del déficit neurológico a las 24 h se ha situado en un déficit neurológico moderado. La puntuación del grado de dependencia a los tres meses se ha situado en la categoría discapacidad leve. Se ha obtenido correlación significativa entre el déficit neurológico y el resultado funcional.
Artículo
Diríjase al área privada de socios de la web de la SEDENE, (https://sedene.com/revista-de-sedene/ ) y autentifíquese.
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora