


Despite the development of anaesthesia worldwide, not all operating rooms follow minimum stringent safety standards. One of the violations of patient safety standards is simultaneous anaesthesia, which threatens the life of the patient and compromises medical ethics and professionalism.
ObjectiveTo describes the frequency of the practice of simultaneous anaesthesia among a group of anaesthetists and anaesthesia residents who attended a Latin-American Anaesthesiology Congress.
Materials and methodsCross-sectional study of a universe of 954 participants who registered to the XXXII Congress of CLASA, held in Asunción, Paraguay (September 30th to October 3rd, 2013). Participation in the study was voluntary after verbal informed consent on the part of the respondents, and the questionnaire was answered anonymously. This study was approved by the Research Committee of the Colombian Society of Anaesthesiology and Resuscitation (Sociedad Colombiana de Anestesiología y Reanimación – S.C.A.R.E).
ResultsOf the 112 anaesthetists and 29 anaesthesia residents surveyed, 30% recognized that simultaneous anaesthesia is given habitually at their place of work; 26% do not apply the checklist; 24% consider that the practice is justified; and 84% are in favour of penalizing this behaviour.
ConclusionThere are places where simultaneous anaesthesia is still practiced and where the checklist is not used. A vast majority of the respondents agree that this breach must be penalized in order to improve patient safety.
A pesar del desarrollo que ha tenido la anestesiología a nivel mundial, no en todos los quirófanos se cumple con un riguroso estándar la aplicación de las normas mínimas de seguridad. Una de las violaciones a la seguridad de los pacientes es la anestesia simultánea, que atenta contra la vida de los pacientes y compromete la ética y el profesionalismo médico.
ObjetivoDescribir la frecuencia de uso de la anestesia simultánea en un grupo de anestesiólogos y estudiantes de posgrado de anestesiología asistentes a un Congreso Latinoamericano de Anestesiología.
Métodos y materialesEstudio de corte transversal en un universo de 954 inscritos al XXXII Congreso de la CLASA en Asunción, Paraguay (30 de septiembre a 3 de octubre de 2013). La participación fue voluntaria, previo consentimiento informado verbal por parte de los encuestados, y el formulario de respuesta fue anónimo. Este estudio fue aprobado por el Comité de Investigaciones de la Sociedad Colombiana de Anestesiología y Reanimación (SCARE).
ResultadosDe los 112 anestesiólogos y 29 estudiantes de posgrado en anestesiología encuestados, el 30% reconocieron que en los sitios donde trabajan se da anestesia simultánea de manera habitual; el 26% no aplican la lista de chequeo; el 24% consideran que se justifica esta práctica, y el 84% están a favor de sancionar esta conducta.
ConclusiónTodavía hay lugares en donde se practica la anestesia simultánea y no se utiliza la lista de chequeo. Una gran mayoría de los encuestados están de acuerdo en que se debe sancionar esta infracción en procura de la seguridad de los pacientes.
In the past, given little availability of medical professionals trained in the practice of anaesthesia, it was commonplace to see the risky practice of providing simultaneous anaesthesia where the patient was abandoned not only in rooms within the same institution but also between separate hospitals.1
At the present time, this practice is considered illegal by the specialty2 and considering the fact that the patient is defenceless when under anaesthesia, this practice also constitutes betrayal of the trust placed in the anaesthetist and, consequently, the surgical teams and the institutions that lend themselves to this practice are also guilty. Simultaneous anaesthesia, unlike medical error, is considered malpractice and, as such, is inexcusable.3
The current practice of simultaneous anaesthesia is unknown. In some places it is tolerated because of the little availability of specialized teams and because of the economic interests of the practitioners who want to increase their income.4
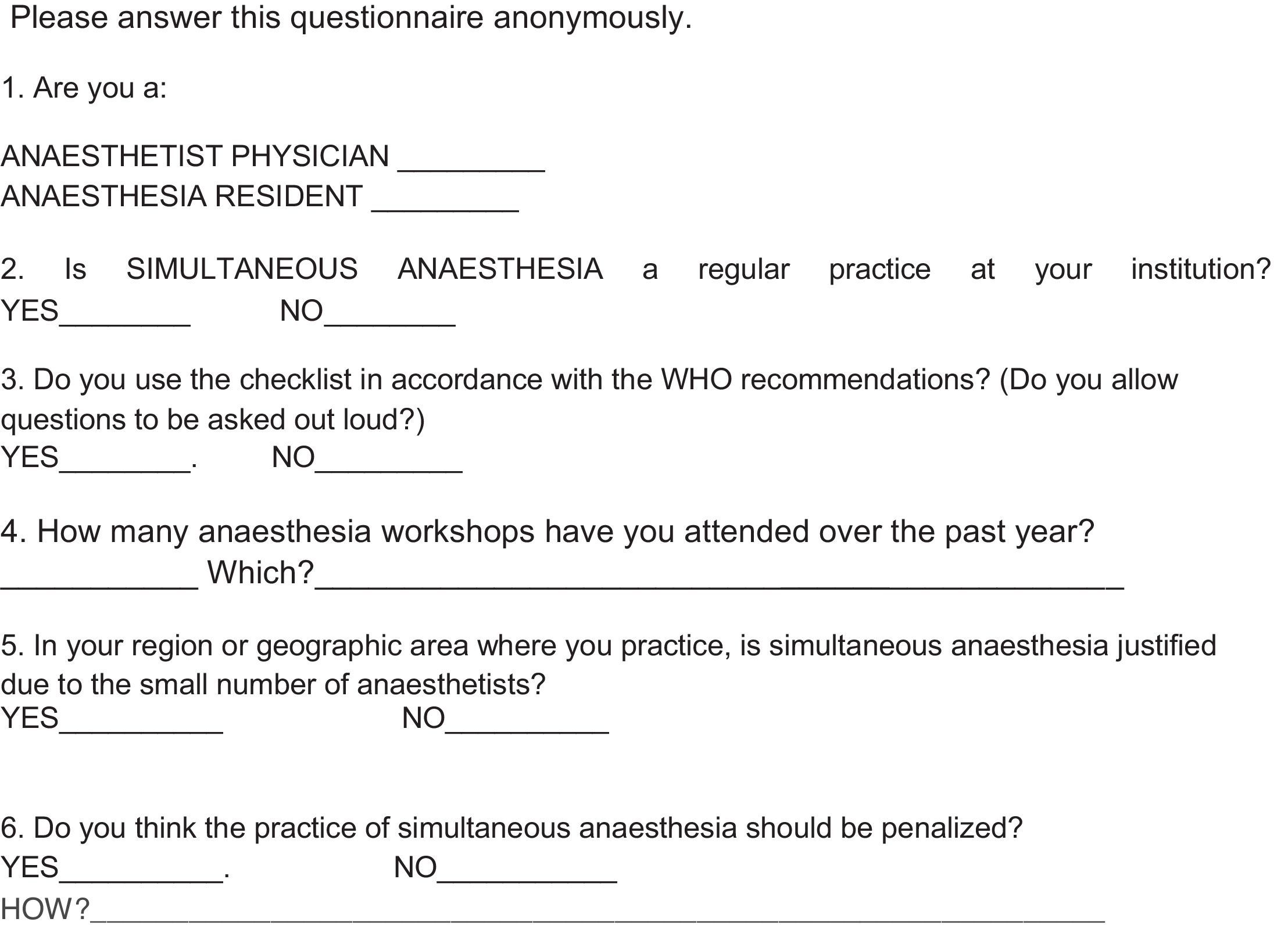
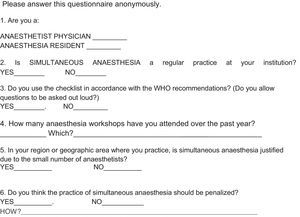
Considering that the rejection of the practice of simultaneous anaesthesia varies in different countries, and in order to determine what is the reality of this ethical and legal problem in Latin-America, a survey was conducted among anaesthetists of various LatinAmerican countries who attended the XXXII Congress of the Latin-American Confederation of Anaesthesia Societies (CLASA), held between September 30th and October 3rd, 2013, in Asunción, Paraguay (Annex 1 for the form).
MethodologyCross-sectional study of a universe of 954 participants (more than 150 anaesthesia professors of Latin-America, Europe and North America) registered at the XXXII Congress of CLASA from September 30th to October 3rd, 2013. Participation in the survey was voluntary after giving verbal informed consent, and the answers to the questionnaire were anonymous. This study was approved by the Research Committee of Sociedad Colombiana de Anestesiología y Reanimación (S.C.A.R.E).
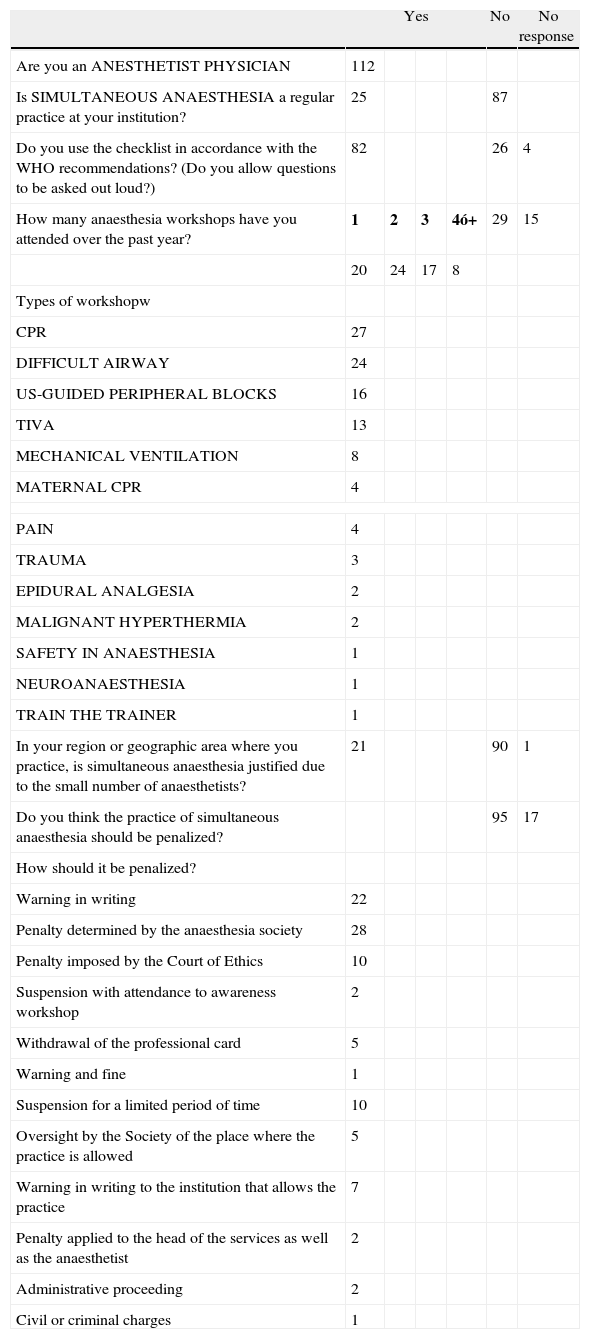
ResultsOverall, 141 participants responded: 112 anaesthetists working in hospitals and clinics in Latin-America, and 29 anaesthesia residents (14% of the attendees).
Of the respondents, 30% recognize that in the region of Latin-America where they work, simultaneous anaesthesia is given; 26% do not apply the checklist proposed by the World Health Organization (WHO) (which requires the presence of the anaesthetist throughout the entire anaesthetic procedure).5 Half of the anaesthetists have attended at least one anaesthesia workshop with simulators in the past year, an activity where, in order to succeed, teamwork and accountability are a pre-requisite. However, of the 19 residents surveyed, only 58% had attended one simulation workshop over the preceding year. The most frequent workshops offered are for cerebro-cardio-pulmonary resuscitation, difficult airway, ultrasound-guided regional blocks, and total intravenous anaesthesia (TIVA). Only one anaesthetist reported attendance to a workshop on safety in anaesthesia. An important percentage of the anaesthetists (24%) believe that simultaneous anaesthesia is justified in their regions, while 84% agree that the “malpractice” of simultaneous anaesthesia should be penalized, and some are of the opinion that the penalty should be suspension from professional practice, and even submission of the case to civil or criminal courts (Annexes 2 and 3).
DiscussionAlthough systematic errors have diminished worldwide,6 and anaesthesia is considered to have minimum procedural failings,7–9 the results of this study point to the fact that the practice of simultaneous anaesthesia in developing countries (for example, in Latin-America) is a threat to patient safety.
It is noteworthy that almost 30% of the respondents acknowledged the existence of simultaneous anaesthesia practice in their region. Given the anonymous nature of this type of questionnaire, it was not possible to determine the region from which these responses came. However, this finding suggests a very frequent practice, at least among the group of respondents, when the result should have been naught.
The checklist is a very useful tool in the surgical setting, considering that its has been shown to contribute to the early identification of adverse events,10 and to reduce complications from 11% to 7% (p<0.001).11 Added to this is the fact that only one of the respondents had attended a workshop on patient safety.
In Colombia, Medical Ethics Standards are regulated by Law 23 of 1981, which states the following under Article 15: “Physicians shall not expose their patients to unwarranted risks (those unrelated to the patient's clinical and pathological conditions)”.
Institutions must not allow this type of illegal action, regardless of the motivation (lack of anaesthetists, profit, etc.), because, after all, they are accountable for all risks: administrative, criminal, civil and ethical, not to mention the moral risks, the loss of reputation and credibility, and discredit.
In its 2009 Manual on the application of the surgical safety checklist, the WHO requires the presence of the anaesthetist at the beginning of the procedure, during the procedure and at the end of the procedure.5
Sociedad Colombiana de Anestesiología (S.C.A.R.E.), after due process and after determining that the anaesthetist is guilty of the serious fault of “providing simultaneous anaesthesia”, proceeds immediately to suspend the coverage to which the associate is entitled as an active partner of FEPASDE (special support fund for lawsuits) and to expel him or her from the Society. It is necessary that the other members of the Latin-American Confederation of Anaesthesia Societies (CLASA) implement similar procedures. “It is not only a matter of complying with the licensure requirements and preventing very serious legal jeopardy, but of protecting the patient's life and integrity”.12
In England, the Royal College of Anaesthetists, which is the body in charge of maintaining the standards of quality care and safety applied to all patients undergoing surgery, emphasizes the following 3 components in relation to the provision of anaesthesia care:
- 1.
A well-trained, experienced anaesthetist must be present throughout all general and regional anaesthetic procedures, including procedures requiring sedation.
- 2.
An anaesthetist needs to be physically at the patient's side during the administration of general anaesthesia.
- 3.
Care in anaesthesia services during emergencies, including surgery, must be provided by competent anaesthetists.13,14
In Colombia, Resolution 2003 of 2014 (page 132) issued by the Ministry of Health and Social Protection defines the licensure procedures and conditions that healthcare providers are required to comply with, and states the following: “Operative services offering low (medium and high) complexity surgical procedures must have an anaesthetist on site to carry out only one procedure at a time and who must be present throughout the surgical procedure and be accountable for it”.15
The CLASA promotional poster on the safety of anaesthesia (Fig. 1) reflects an irrefutable slogan: simultaneous anaesthesia must not be allowed; it is not justified under any circumstance and it is a source of adverse events and a breach to the safe practice of anaesthesiology.

In Colombia there are 2324 anaesthetists, almost 1000 of them practicing in Bogotá, the capital city with a population of more than 7.5 million (1 anaesthetist for every 7500 inhabitants). In Cuba, according to Sainz H & Cordero I, delegates from the Cuban Society of Anaesthesiology to CLASA (personal communication) there are close to 1400 anaesthetists and 11.14 million inhabitants (1 anaesthetist for every 8000 people), and in Havanah, the capital city, there are 420 anaesthetists to serve 2 million inhabitants (1 for every 4761 inhabitants). In Argentina, according to Weissbrod EP, member and secretary of the Argentinian Society of Anaesthesia, Analgesia and Resuscitation of Buenos Aires (AAARBA) (personal communication) there are 12.8 million inhabitants and 2018 anaesthetists (1 for every 6343 inhabitants). In Managua, capital city of Nicaragua, according to Arguello B, member of the Anaesthesia Society of Nicaragua (personal communication), the situation is complex given that there are approximately 1.6 million inhabitants and only 100 anaesthetists (1 for every 16,000 inhabitants). The thinking, therefore, may be that the number of anaesthetists is insufficient, creating the need to practice simultaneous anaesthesia in certain places. However, according to some experts, the reality does not always coincide with the figures,16 and when the operating rooms are licensed in a coherent way, it is possible to achieve a balanced distribution between the number of anaesthetists and the population requiring anaesthesia care.16 Life prevails above any dilemma, so there is no excuse or justification for any of the members of the surgical team to abandon a patient in the middle of major surgery.
Since the 1980s, doctor Alberto Scafati, anaesthesia specialist, has pioneered the “National Campaign for the Eradication of Simultaneous Anaesthesia and Patient Abandonment” in Argentina. This printed campaign has added to its reference logo (Fig. 2) the slogan “One anaesthetist for every patient=SAFETY”. Although it was publicized nationwide, there is still a need for strong awareness action in order to eradicate simultaneous anaesthesia from that part of the continent.
Conclusion.")
Important work is still required in the form of education campaigns to raise awareness not only among anaesthetists but also among patients; safety in medicine must be institutionalized3 the different scientific anaesthesia societies must come forward with strong statements against these criminal acts that endanger the health and lives of the patients and jeopardize the prestige of our specialty.
Ethical disclosuresProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work centre on the publication of patient data.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
FundingThe authors’ own resources.
Conflicts of interestThe principal author is the President of Sociedad Colombiana de Anestesiología y Reanimación (S.C.A.R.E.)
| Yes | No | No response | ||||
| Are you an ANESTHETIST PHYSICIAN | 112 | |||||
| Is SIMULTANEOUS ANAESTHESIA a regular practice at your institution? | 25 | 87 | ||||
| Do you use the checklist in accordance with the WHO recommendations? (Do you allow questions to be asked out loud?) | 82 | 26 | 4 | |||
| How many anaesthesia workshops have you attended over the past year? | 1 | 2 | 3 | 4ó+ | 29 | 15 |
| 20 | 24 | 17 | 8 | |||
| Types of workshopw | ||||||
| CPR | 27 | |||||
| DIFFICULT AIRWAY | 24 | |||||
| US-GUIDED PERIPHERAL BLOCKS | 16 | |||||
| TIVA | 13 | |||||
| MECHANICAL VENTILATION | 8 | |||||
| MATERNAL CPR | 4 | |||||
| PAIN | 4 | |||||
| TRAUMA | 3 | |||||
| EPIDURAL ANALGESIA | 2 | |||||
| MALIGNANT HYPERTHERMIA | 2 | |||||
| SAFETY IN ANAESTHESIA | 1 | |||||
| NEUROANAESTHESIA | 1 | |||||
| TRAIN THE TRAINER | 1 | |||||
| In your region or geographic area where you practice, is simultaneous anaesthesia justified due to the small number of anaesthetists? | 21 | 90 | 1 | |||
| Do you think the practice of simultaneous anaesthesia should be penalized? | 95 | 17 | ||||
| How should it be penalized? | ||||||
| Warning in writing | 22 | |||||
| Penalty determined by the anaesthesia society | 28 | |||||
| Penalty imposed by the Court of Ethics | 10 | |||||
| Suspension with attendance to awareness workshop | 2 | |||||
| Withdrawal of the professional card | 5 | |||||
| Warning and fine | 1 | |||||
| Suspension for a limited period of time | 10 | |||||
| Oversight by the Society of the place where the practice is allowed | 5 | |||||
| Warning in writing to the institution that allows the practice | 7 | |||||
| Penalty applied to the head of the services as well as the anaesthetist | 2 | |||||
| Administrative proceeding | 2 | |||||
| Civil or criminal charges | 1 | |||||
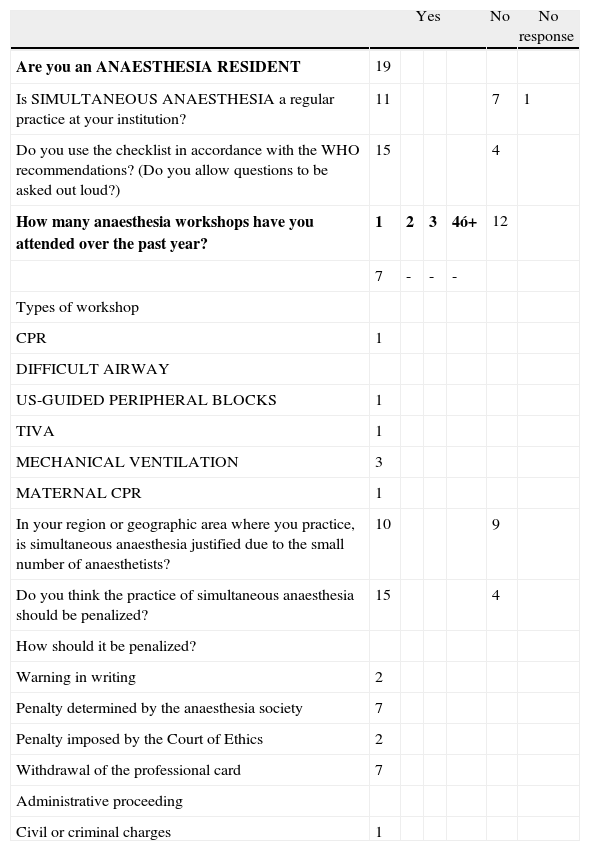
| Yes | No | No response | ||||
| Are you an ANAESTHESIA RESIDENT | 19 | |||||
| Is SIMULTANEOUS ANAESTHESIA a regular practice at your institution? | 11 | 7 | 1 | |||
| Do you use the checklist in accordance with the WHO recommendations? (Do you allow questions to be asked out loud?) | 15 | 4 | ||||
| How many anaesthesia workshops have you attended over the past year? | 1 | 2 | 3 | 4ó+ | 12 | |
| 7 | - | - | - | |||
| Types of workshop | ||||||
| CPR | 1 | |||||
| DIFFICULT AIRWAY | ||||||
| US-GUIDED PERIPHERAL BLOCKS | 1 | |||||
| TIVA | 1 | |||||
| MECHANICAL VENTILATION | 3 | |||||
| MATERNAL CPR | 1 | |||||
| In your region or geographic area where you practice, is simultaneous anaesthesia justified due to the small number of anaesthetists? | 10 | 9 | ||||
| Do you think the practice of simultaneous anaesthesia should be penalized? | 15 | 4 | ||||
| How should it be penalized? | ||||||
| Warning in writing | 2 | |||||
| Penalty determined by the anaesthesia society | 7 | |||||
| Penalty imposed by the Court of Ethics | 2 | |||||
| Withdrawal of the professional card | 7 | |||||
| Administrative proceeding | ||||||
| Civil or criminal charges | 1 | |||||
Please cite this article as: Navarro-Vargas JR, Arguello B, Scafati A. A propósito de una encuesta sobre la Práctica Habitual de Anestesia Simultánea en Latinoamérica. Rev Colomb Anestesiol. 2014;42:265–271.