



To present the clinical experience with a new extended (for 15 days), wireless, and satellite cardiac monitoring system in a group of patients with suspicion of cardiac arrhythmia.
MethodThe study included a cohort of 100 patients seen in the Cardiovascular Electrophysiology Unit of a reference hospital. They were suspected of having a cardiac arrhythmia, with no electrocardiographic diagnosis of the cause, despite previous examinations. They were subjected to SEEQ-type (Medtronic) external cardiac monitoring for 15 days, with the outcomes recorded.
ResultsOf the total of 100 subjects studied, 51% were male, and the median age was 60 years (range: 5 - 91 years). The main symptoms were palpitation, and the most prevalent comorbidity was arterial hypertension (47%). Almost all (98%) of them had a previous Holter study, and 46% had two studies, which were inconclusive in explaining the symptoms. The SEEQ monitoring recorded a significant electrocardiographic abnormality in 22% of the patients. A pacemaker implant was the treatment most applied and atrial fibrillation was the most frequent arrhythmia in 50% of the positive findings. There was a higher and significant percentage of positive diagnoses in males.
ConclusionsExternal, satellite, wireless cardiac monitoring extended for 15 days, is a novel tool that can increase the probability of documenting a clinically significant electrocardiographic abnormality in those patients who suffer recurrent cardiovascular symptoms.
Dar a conocer la experiencia clínica con un nuevo sistema de monitorización cardiaca extendida (por 15 días), inalámbrica y satelital en un grupo de pacientes con sospecha de arritmias cardíacas.
MetodologíaCohorte de 100 pacientes atendidos en la unidad de Electrofisiología cardiovascular de un centro de referencia, con sospecha de arritmia cardíaca, sin diagnóstico electrocardiográfico causal, a pesar de exámenes previos. Se les aplicó una monitorización cardiaca externa tipo SEEQ (Medtronic) por 15 días y se registró el desenlace.
ResultadosDe un total de 100 sujetos estudiados, 51% eran hombres, con mediana de edad de 60 años (rango: 5 - 91 años). El principal síntoma fueron las palpitaciones (42%) y la comorbilidad más prevalente la hipertensión arterial (47%); 98% tenían estudio de Holter previo y 46% dos estudios sin resultado conclusivo que explicara los síntomas. La monitorización tipo SEEQ documentó anormalidad electrocardiográfica significativa en 22% de los pacientes. El implante de marcapaso fue el tratamiento más aplicado y la fibrilación auricular fue la arritmia más frecuente en el 50% de los hallazgos positivos. Hubo una proporción mayor y significativa de diagnósticos positivos en el sexo masculino.
ConclusionesLa monitorización cardiaca externa inalámbrica, satelital, extendida por 15 días es una herramienta novedosa que incrementa la probabilidad de documentar una anormalidad electrocardiográfica clínicamente significativa en quienes padecen síntomas cardiovasculares recurrentes.
Cardiac arrhythmias are highly prevalent; it has been reported that atrial fibrillation alone affects one to four percent of the general population, and increases with age to 10% in octogenarians. It is also the cause of other conditions such as cerebrovascular accidents, and may appear as a result of arterial hypertension, obstructive sleep apnea, obesity or ischemic heart disease.1–3
This condition worsens or fosters structural and electrophysiological heart changes, and, in its persistent or chronic form, produces atrial and/or ventricular dilation. Such dilation leads to heart failure and increases the risk of hospitalization, cerebral embolism or sudden death, especially in those with ischemic cardiomyopathy.1,3–8
Heart rhythm alterations may be asymptomatic or may manifest themselves through various signs and symptoms, including palpitations, a sensation of tachycardia or rapid heart rate, presyncope or syncope, and sudden adynamia.1,2 These symptoms, which are chiefly paroxysmal in the beginning stages, may later become persistent or chronic. Their early identification can facilitate timely diagnosis and treatment, but they are often difficult to document.
Traditionally, an electrocardiogram has been considered to be the ¿gold standard¿ for diagnosing cardiac arrhythmias, although obtaining one at the precise moment in which symptoms present is unlikely. In order to increase this possibility, Holter electrocardiographic monitoring was invented, which, by extending the recording period to 24 or 48hours, enhances the observation time, with a greater probability of capturing the arrhythmia.
However, this method is useful when the symptoms and arrhythmia occur at least every other day, since significant findings are less likely when the anomalies occur only once every few days or weeks.
This study intends to show the primary experience in Colombia with continuous, wireless, satellite cardiac monitoring for 15 days, using a Medtronic SEEQ electronic patch system, applied in patients who consulted due to recurrent cardiovascular symptoms possibly related to cardiac arrhythmias.
Materials and methodsType of study and populationThis was a retrospective study carried out in the Cardiovascular Electrophysiology unit of a reference center in Bogotá, which included a cohort of patients with suspected cardiac arrhythmia (with or without a history of ablation) who underwent extended satellite cardiac monitoring, using the SEEQ system, for 15 days between April 1, 2015 and December 31, 2016. Those who did not complete the monitoring, or had not been seen by a specialist to determine treatment by the end of the study, were excluded.
Cardiac monitorThe SEEQ extended cardiac monitoring system is a wireless, electronic adhesive patch device with single channel electrocardiographic monitoring ability (equivalent to a DII electrocardiographic lead), recently introduced to clinical practice. This device is waterproof, a characteristic which allows its continuous use for 7.5 days per patch. To increase the probability of finding a diagnostic tracing, and in accordance with previous studies,9 monitoring is performed for 15 days using two sequential patches, each patch for 7.5 days. The patch placed on the patient¿s chest uses a wireless mobile modem for satellite transmission, similar to a cellular telephone (fig. 1). Patients who received this monitoring had been evaluated by an electrophysiologist due to recurrent episodes of palpitations and/or cardiovascular symptoms (presyncope, syncope) without electrocardiographic correlation despite previous Holter monitoring, or due to non-conclusive alterations on electrocardiogram tracings.

Data collection was done retrospectively using information from the Electrophysiology Unit charts, from which sociodemographic (age and sex), clinical (symptoms, history, chief complaint, reason for test), 24 hour Holter electrocardiogram results and management variables were taken. The SEEQ monitoring results, recorded automatically or activated by the patient, were validated by an electrophysiologist, who was responsible for the final report. A significant diagnostic event was defined as a conclusive electrocardiographic anomaly such as: symptomatic sinus bradycardia (in the daytime or while awake) lower than 40 bpm, bradycardia lower than 40 bpm associated with a slow escape rhythm for more than 10seconds, atrial fibrillation lasting at least five minutes, atrial flutter for more than five minutes, sustained ventricular tachycardia (greater than 30seconds), de novo or paroxysmal trifascicular block (or any of these associated with symptoms), first degree AV block with a PR greater than 320ms, or a T on P phenomenon and de novo WPW, which required management other than clinical follow-up (pharmacological treatment, implantation of a cardiac stimulation device or mapping and ablation of the arrhythmia).
Analysis planAll the information obtained from the medical records was collected in an instrument designed for this purpose. Descriptive statistics, frequencies and proportions were calculated for categorical variables, and measures of dispersion and central tendency for numeric variables. The Chi square or Fisher¿s test was used to evaluate the association between categorical variables.
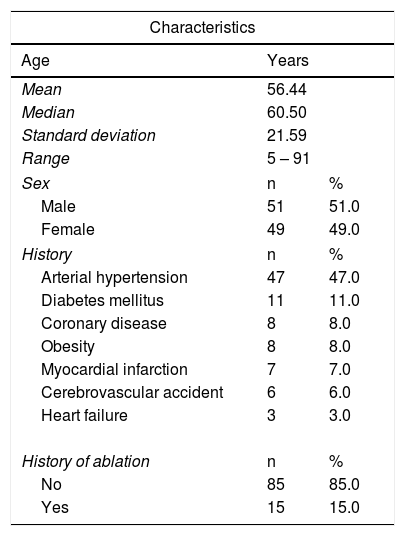
ResultsOne hundred subjects who underwent SEEQ extended satellite monitoring for 15 days were included. The median age was 60 years, with a range of five to 91 years; 51% were male. The indications for SEEQ monitoring were: recurrent palpitations without an evident cause (27%), bradycardia (20%), suspected paroxysmal atrial fibrillation (21%), post-ablation palpitations (15%), syncope (6%), suspected atrioventricular blocks (5%), and other arrhythmias (6%). With regard to history, arterial hypertension was the most common, present in about half of the patients. Approximately 15% of the study population had a history of ablation, and they were monitored to follow-up on palpitations (Table 1).
Demographic and clinical information of the patients included in the study.
| Characteristics | ||
|---|---|---|
| Age | Years | |
| Mean | 56.44 | |
| Median | 60.50 | |
| Standard deviation | 21.59 | |
| Range | 5 – 91 | |
| Sex | n | % |
| Male | 51 | 51.0 |
| Female | 49 | 49.0 |
| History | n | % |
| Arterial hypertension | 47 | 47.0 |
| Diabetes mellitus | 11 | 11.0 |
| Coronary disease | 8 | 8.0 |
| Obesity | 8 | 8.0 |
| Myocardial infarction | 7 | 7.0 |
| Cerebrovascular accident | 6 | 6.0 |
| Heart failure | 3 | 3.0 |
| History of ablation | n | % |
| No | 85 | 85.0 |
| Yes | 15 | 15.0 |
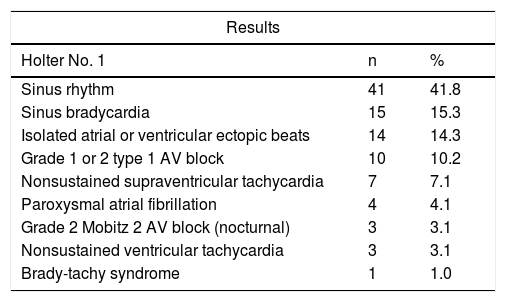
Ninety-eight percent of patients had had at least one prior 24 hour Holter electrocardiographic test. In two percent of cases it was not ordered, since the patients reported sporadic symptoms, rather than every other day. A total of 58.2% of studies showed inconclusive abnormal tracings; among these, the most frequent were non-extreme sinus bradycardia and isolated atrial or ventricular ectopic beats. Forty-six percent of the patients had a second 24 hour Holter electrocardiographic study, 41.3% of which were normal. The most frequent results in this second test were isolated atrial or ventricular ectopic beats, and first degree and second degree type 1 atrioventricular blocks (Table 2).
Results of electrocardiographic Holter performed prior to SEEQ.
| Results | ||
|---|---|---|
| Holter No. 1 | n | % |
| Sinus rhythm | 41 | 41.8 |
| Sinus bradycardia | 15 | 15.3 |
| Isolated atrial or ventricular ectopic beats | 14 | 14.3 |
| Grade 1 or 2 type 1 AV block | 10 | 10.2 |
| Nonsustained supraventricular tachycardia | 7 | 7.1 |
| Paroxysmal atrial fibrillation | 4 | 4.1 |
| Grade 2 Mobitz 2 AV block (nocturnal) | 3 | 3.1 |
| Nonsustained ventricular tachycardia | 3 | 3.1 |
| Brady-tachy syndrome | 1 | 1.0 |
| Holter No. 2 | n | % |
|---|---|---|
| Sinus rhythm | 19 | 41.3 |
| Isolated atrial or ventricular ectopic beats | 9 | 19.6 |
| Grade 1 or 2 type 1 AV block | 6 | 13.0 |
| Sinus bradycardia | 4 | 8.7 |
| Paroxysmal atrial fibrillation | 4 | 8.7 |
| Nonsustained ventricular tachycardia | 3 | 6.5 |
| Nonsustained supraventricular tachycardia | 1 | 2.2 |
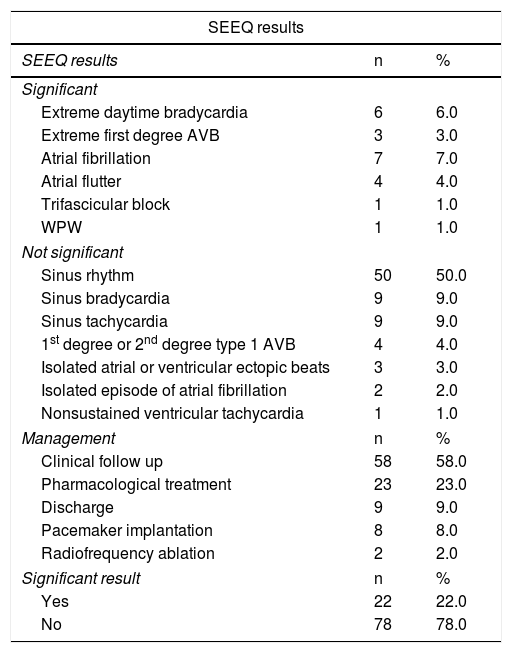
The monitoring results are described in Table 3. As shown, 22 results were considered to be clinically significant (diagnostic electrocardiographic tracings of a specific arrhythmia, leading to treatment). The most common arrhythmias were atrial flutter and atrial fibrillation in 11 patients, equal to 50% of the cases. Those who received this diagnosis had comorbidities such as arterial hypertension (64%), obesity (36%), a history of acute myocardial infarction (27.3%), heart failure (9.1%) and cerebrovascular accidents (9.1%).
SEEQ monitoring results and management chosen.
| SEEQ results | ||
|---|---|---|
| SEEQ results | n | % |
| Significant | ||
| Extreme daytime bradycardia | 6 | 6.0 |
| Extreme first degree AVB | 3 | 3.0 |
| Atrial fibrillation | 7 | 7.0 |
| Atrial flutter | 4 | 4.0 |
| Trifascicular block | 1 | 1.0 |
| WPW | 1 | 1.0 |
| Not significant | ||
| Sinus rhythm | 50 | 50.0 |
| Sinus bradycardia | 9 | 9.0 |
| Sinus tachycardia | 9 | 9.0 |
| 1st degree or 2nd degree type 1 AVB | 4 | 4.0 |
| Isolated atrial or ventricular ectopic beats | 3 | 3.0 |
| Isolated episode of atrial fibrillation | 2 | 2.0 |
| Nonsustained ventricular tachycardia | 1 | 1.0 |
| Management | n | % |
| Clinical follow up | 58 | 58.0 |
| Pharmacological treatment | 23 | 23.0 |
| Discharge | 9 | 9.0 |
| Pacemaker implantation | 8 | 8.0 |
| Radiofrequency ablation | 2 | 2.0 |
| Significant result | n | % |
| Yes | 22 | 22.0 |
| No | 78 | 78.0 |
AVB=atrioventricular block WPW=Wolff-Parkinson-White syndrome.
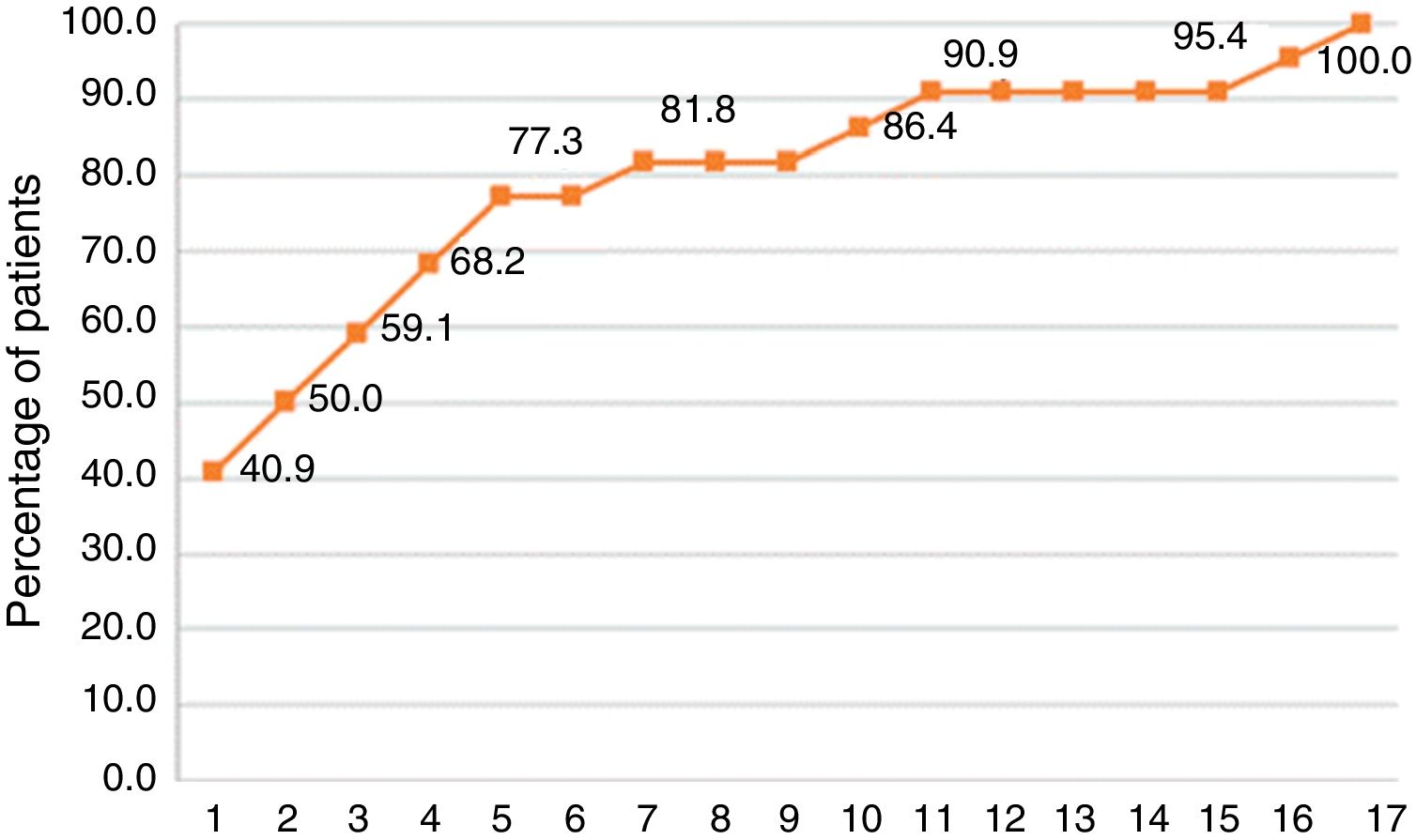
As shown in figure 2, the identification of the first arrhythmic episode occurred after the first monitoring day in 60% of the patients, and reached 90% on day 11. Based on the monitoring results, eight patients required pacemaker implantation, two required radiofrequency ablation, and the remaining 12 were treated pharmacologically.

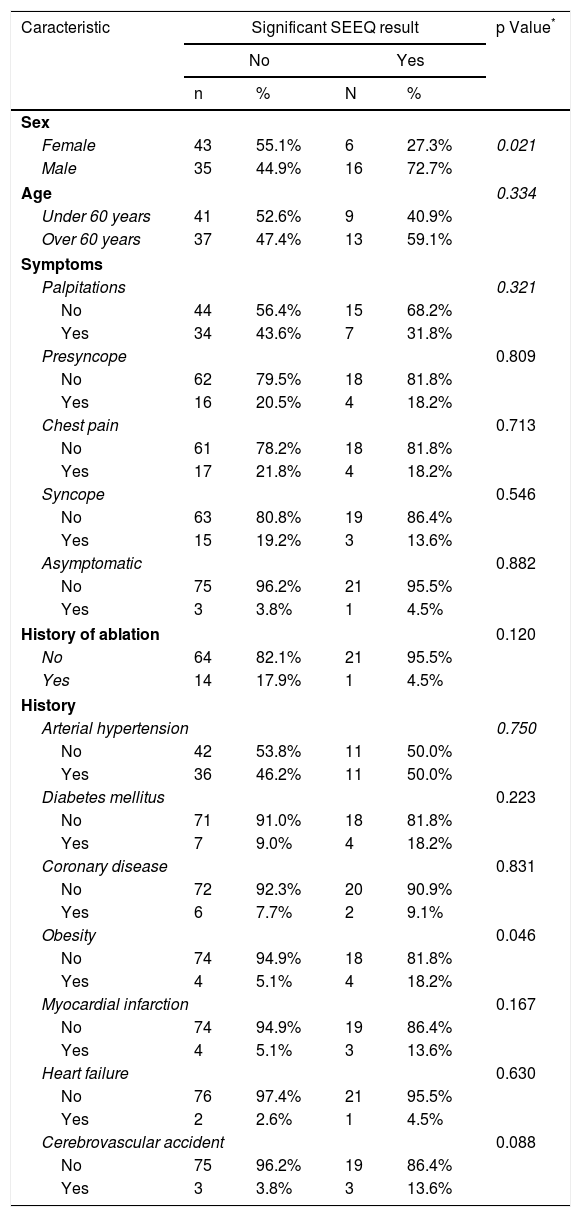
The evaluation of which variables could be related to a clinically significant SEEQ monitoring result showed a significant association with the male sex, since a greater proportion of significant diagnoses was found in men (p=0.021). There were no differences with regard to age, symptoms and history (Table 4).
SEEQ monitoring results according to demographic and clinical characteristics.
| Caracteristic | Significant SEEQ result | p Value* | |||
|---|---|---|---|---|---|
| No | Yes | ||||
| n | % | N | % | ||
| Sex | |||||
| Female | 43 | 55.1% | 6 | 27.3% | 0.021 |
| Male | 35 | 44.9% | 16 | 72.7% | |
| Age | 0.334 | ||||
| Under 60 years | 41 | 52.6% | 9 | 40.9% | |
| Over 60 years | 37 | 47.4% | 13 | 59.1% | |
| Symptoms | |||||
| Palpitations | 0.321 | ||||
| No | 44 | 56.4% | 15 | 68.2% | |
| Yes | 34 | 43.6% | 7 | 31.8% | |
| Presyncope | 0.809 | ||||
| No | 62 | 79.5% | 18 | 81.8% | |
| Yes | 16 | 20.5% | 4 | 18.2% | |
| Chest pain | 0.713 | ||||
| No | 61 | 78.2% | 18 | 81.8% | |
| Yes | 17 | 21.8% | 4 | 18.2% | |
| Syncope | 0.546 | ||||
| No | 63 | 80.8% | 19 | 86.4% | |
| Yes | 15 | 19.2% | 3 | 13.6% | |
| Asymptomatic | 0.882 | ||||
| No | 75 | 96.2% | 21 | 95.5% | |
| Yes | 3 | 3.8% | 1 | 4.5% | |
| History of ablation | 0.120 | ||||
| No | 64 | 82.1% | 21 | 95.5% | |
| Yes | 14 | 17.9% | 1 | 4.5% | |
| History | |||||
| Arterial hypertension | 0.750 | ||||
| No | 42 | 53.8% | 11 | 50.0% | |
| Yes | 36 | 46.2% | 11 | 50.0% | |
| Diabetes mellitus | 0.223 | ||||
| No | 71 | 91.0% | 18 | 81.8% | |
| Yes | 7 | 9.0% | 4 | 18.2% | |
| Coronary disease | 0.831 | ||||
| No | 72 | 92.3% | 20 | 90.9% | |
| Yes | 6 | 7.7% | 2 | 9.1% | |
| Obesity | 0.046 | ||||
| No | 74 | 94.9% | 18 | 81.8% | |
| Yes | 4 | 5.1% | 4 | 18.2% | |
| Myocardial infarction | 0.167 | ||||
| No | 74 | 94.9% | 19 | 86.4% | |
| Yes | 4 | 5.1% | 3 | 13.6% | |
| Heart failure | 0.630 | ||||
| No | 76 | 97.4% | 21 | 95.5% | |
| Yes | 2 | 2.6% | 1 | 4.5% | |
| Cerebrovascular accident | 0.088 | ||||
| No | 75 | 96.2% | 19 | 86.4% | |
| Yes | 3 | 3.8% | 3 | 13.6% | |
There were significant differences (p=0.0356) between men and women with regard to the indication for monitoring. In a sizeable proportion of men (31%), the indication for monitoring was bradycardia, compared with 8.2% in women.
An analysis by indication showed that the majority of significant results were from patients who had undergone monitoring due to bradycardia.
A total of three satellite alerts were received; however, after being evaluated by the specialist, all three cases were determined to be false positives due to artifacts.
DiscussionThe two most relevant points of the study were: 1) the use of a new, wireless satellite extended cardiac monitoring system for 15 days for the diagnosis of electrocardiographic alterations which could be correlated with cardiovascular symptoms; and 2) the documentation, using this new system, of a significant electrocardiographic anomaly, leading to the adoption of a new treatment strategy, in 22% of the patients who did not have an established diagnosis despite multiple prior studies and consults. This diagnostic yield (22%) was greater than that of a study carried out on a cohort of 3,209 children with suspected clinically significant arrhythmias, where a patch with similar technology to that of SEEQ achieved 12.2% in 14 days of monitoring.10
Palpitations, presyncope or syncope of unknown origin are among the most frequent symptoms prompting internal medicine and cardiology consults.11 Traditionally, 24 hour Holter cardiac monitoring is the most frequently used method to attempt to capture a cardiac arrhythmia which would explain these symptoms. However, the erratic and sporadic nature of these symptoms leads to a low diagnostic yield.12–14 Extended cardiac monitoring using the SEEQ system is a new tool which has the principal advantages of being easily portable, having a wireless system, being water resistant and having the capacity for external activation by the patient as well as automatic activation, transmitting via satellite the electrocardiographic tracings which can be correlated with symptoms.
The device is considered to be a highly important technological advance, as it has a lower complexity than the other systems or devices that are usually used for cardiac monitoring (e.g. 24 hour, 48 hour, or seven day Holter; external cardiac event monitors). That is, it eliminates surface cables and electrodes which reduces electrical interference caused by vibration, avoids recording interruptions caused by the detachment of a cable or electrode, increases the number of monitoring days, does not require daily change, and tolerates exposure to water; characteristics which redound to patient comfort. The main disadvantages of this novel monitoring, compared with the traditional 24 hour Holter electrocardiographic monitoring, are the impossibility of taking precise measurements with electronic calipers; the dependence on a remote reception and reading center; the unavailability of several electrocardiographic channels or minimum, maximum, and daily and hourly average values; and limited recordingof the arrhythmia, among others.
Zimetbaum et al. studied the optimal length of cardiac monitoring with relation to its diagnostic potential, and affirmed that 90% of cardiac arrhythmias could be captured in the first two weeks; monitoring beyond this period resulted in increased costs.9 However, besides the observation time, there are other factors that should be considered in order to increase the percentage of positive capture of a significant arrhythmia: the type and frequency of symptoms, the timing of monitoring related to the symptoms, and the type of population studied, among others.
The length of monitoring could be irrelevant if the symptom frequency is very high; that variable becomes important when the symptom is sporadic, erratic, or infrequent. Twenty-four or 48 hour Holter monitoring has a 15 to 28% diagnostic yield for daily or every-other-day symptoms,12–14 but its yield is very low when the symptom is more infrequent, when it presents erratically (as happens in atrial fibrillation) or when the study is used for diagnosing syncope, where its diagnostic yield has been reported to be only four percent15 (fig. 3). External loop recorders were designed to extend monitoring and activate it specifically during events or symptoms. This system increased the diagnostic yield of correlating the symptom (intermittent palpitations) with a documented arrhythmia in up to 67% after a three month extended monitoring.16 However, the device does not monitor continuously and requires patient activation during the clinical event, a process which may fail due to the symptom, as the patient may be incapable of activating it or may not activate it correctly; this phenomenon was reported in up to 23% of a case series.17 In addition, the surface electrodes and monitor cables are uncomfortable after a certain number of days of use, which limits patient satisfaction; and, finally, some of these devices do not record asymptomatic events, which is of paramount importance in cardiac arrhythmias such as atrial fibrillation (30% of the events in hypertensive patients, and up to 50% in other series) .1,18 According to Balmelli et al., a cardiac event monitor should have automatic activation, since a percentage of significant electrocardiographic findings are captured using this algorithm, rather than patient activation.18 Furthermore, implantable cardiac monitoring has shown that, for sporadic, erratic or isolated symptoms (periodicity of at least one month), a longer monitoring period is required to capture an anomaly: usually more than one year.19
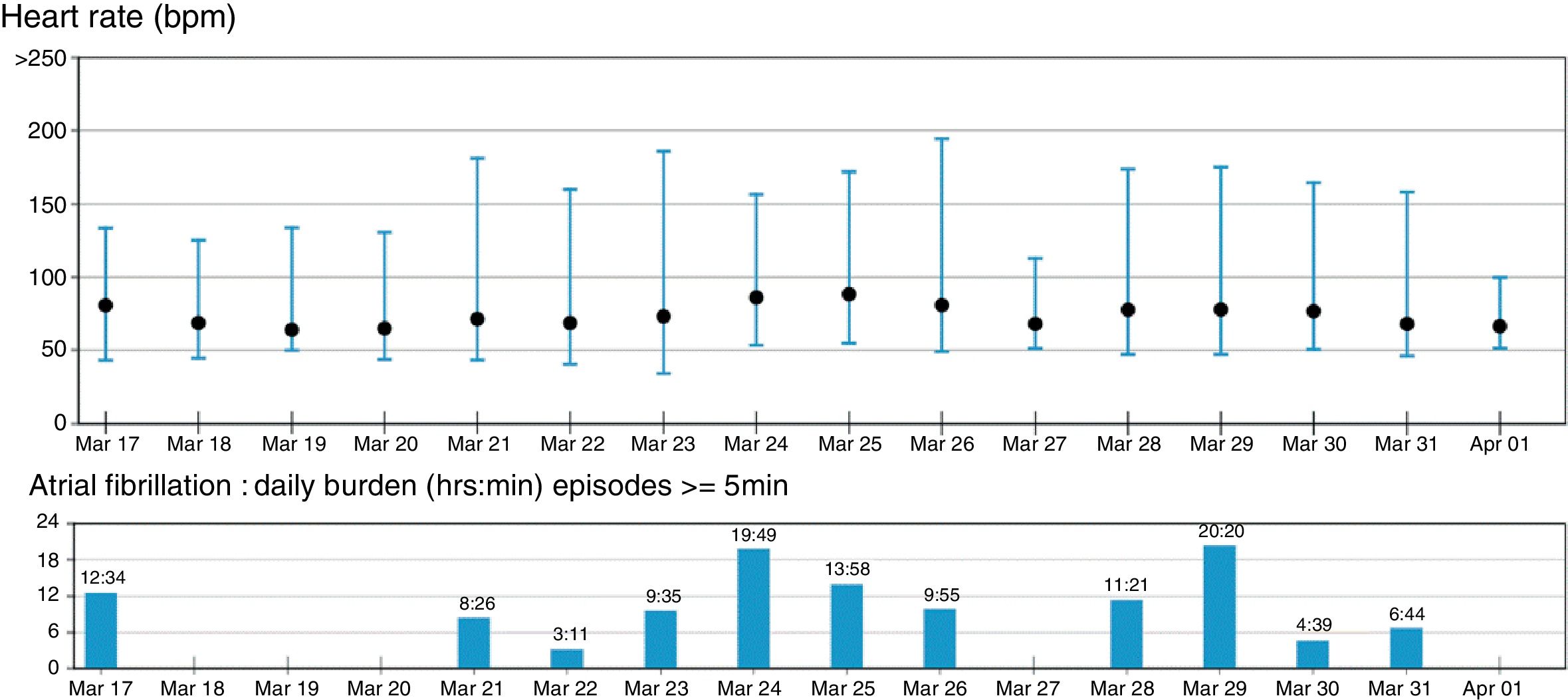
 that on March 18, 19, 20 and 27 and April 1, no atrial fibrillation was recorded. A 24 hour electrocardiographic Holter performed on those days would not have produced a diagnosis.")
Summary of the 15 day SEEQ recording of a patient with a history of palpitations without documented arrhythmia, in spite of a prior 24 hour Holter electrocardiographic test. Notice in the bar graph showing the burden of atrial fibrillation (episodes>5minutes, cumulative frequency) that on March 18, 19, 20 and 27 and April 1, no atrial fibrillation was recorded. A 24 hour electrocardiographic Holter performed on those days would not have produced a diagnosis.
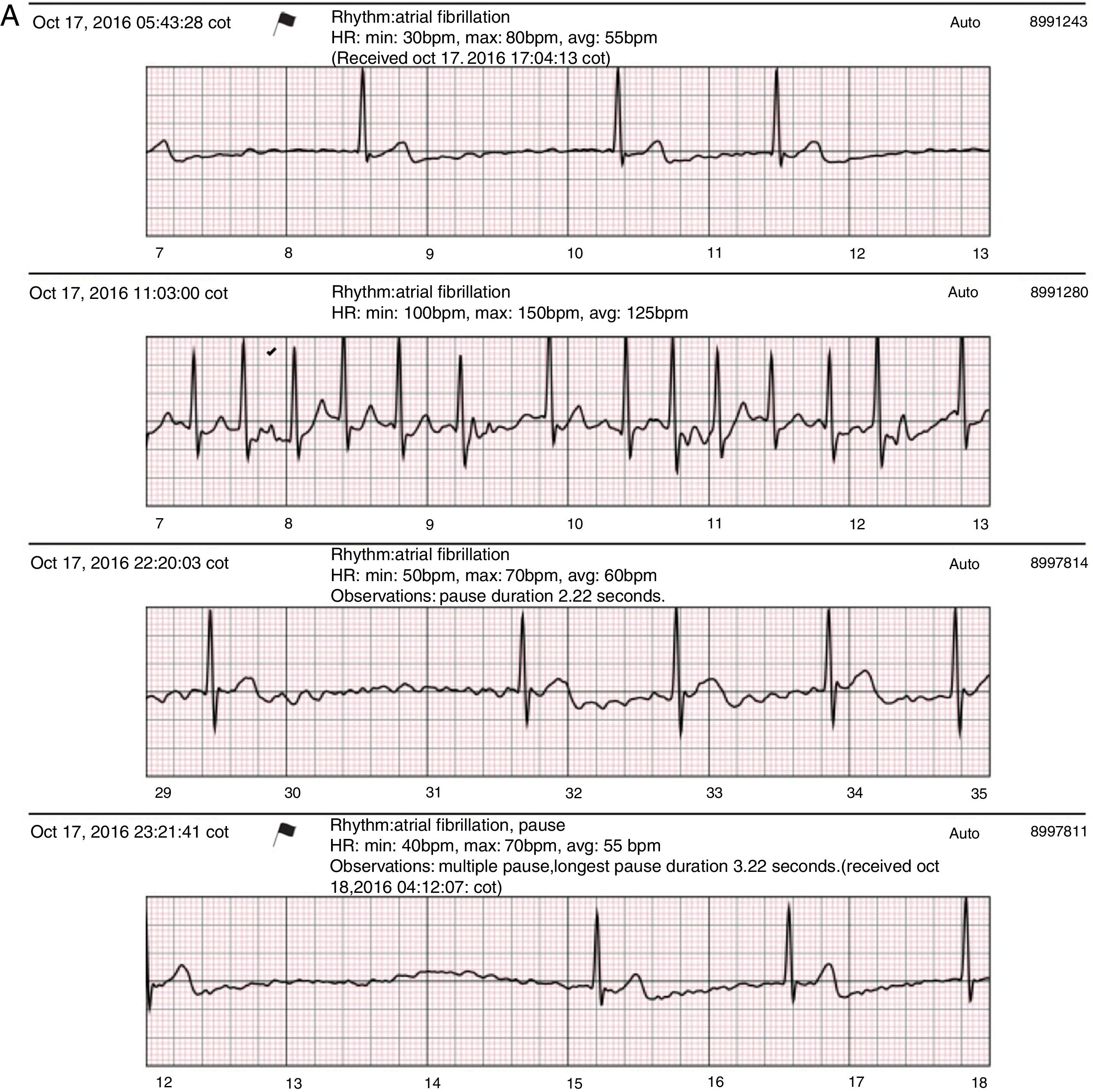
Recent studies using extended cardiac monitoring in patient populations with similar symptoms to those presented in this series have produced conclusive results which are correlatable with clinically significant arrhythmias in up to 41%.20 Nevertheless, the population in these studies presented a greater frequency of symptoms and a higher incidence of cardiovascular disease, with 21% coronary disease, contrasting with the 15% in the current study. Also, cardiac monitoring was extended for 30 days. The diagnostic yield in Rothman et al.¿s 20 study was even higher when the investigated symptom was recurrent presyncope or syncope (89%), in spite of the extremely high preceding symptom frequency in this subgroup of patients (1-99 presyncopal events and/or 1-10 syncopal events prior to monitoring). Arterial hypertension was the most common comorbidity in both studies, with a similar percentage: 47% in the current series versus 52% in the study being discussed. Arterial hypertension is the disease most related to atrial fibrillation; it increases the risk of this arrhythmia by 70-80%, and is the cause of approximately 20% of atrial fibrillation cases in the Western world.1 This relationship may explain the presence of this arrhythmia or its substitutes (atrial flutter) in 11 of the 22 positive results found in the current study (fig. 4A) as well as in Rothman et al.¿s study, in which it was also the most common arrhythmia (23%). Patients with positive atrial fibrillation and/or flutter findings on SEEQ monitoring in the current study had a high rate of comorbidities besides hypertension, obesity and coronary disease.


A: Sample SEEQ tracings. Patient with atrial fibrillation not previously diagnosed by Holter monitoring, with multiple tracings at different hours of the same day; the flag sign in the first tracing corresponds to an automatic system report sent as an alert due to the low heart rate and arrhythmia. B: Extreme symptomatic daytime sinus bradycardia. C. 2:1 AV block in an awake patient with a history of syncope of unknown origin.
The inconclusive findings of the first Holter and the conclusive final results of SEEQ suggest that patients with cardiovascular symptoms of a suspected arrhythmic origin could benefit in a greater proportion from extended monitoring rather than a repeated Holter monitoring.21 Prolonged observation of symptoms with concomitant monitoring increases the possibility of establishing a significant clinical correlation. In this study, three days were required to record 50% of the positive findings, five to six days to obtain 70% of the findings, and 10 to 11 days to obtain 90% of the positive findings (fig. 2).
Likewise, the 22% of positive findings obtained through SEEQ monitoring in the present case series could be increased if other candidates were considered for this monitoring: individuals with recurrent palpitations, those who describe their symptomatology in a more consistent way, with regard to event duration (for example, lasting at least one minute), those with more frequent events (at least weekly), and those with a high total of accumulated events, as in the Rothman20 study. The mere description of the symptom is not enough; its semiological characteristics must be considered in order to increase the possibility of documenting its electrocardiographic correlation.
The finding of significant bradycardia during the daytime or while awake (<40 bpm) (more frequent in men) and the possibility of it explaining the symptoms leading to pacemaker implantation, has been recognized by other implantable cardiac monitor studies.19 As many as 70% of patients who show non-significant or initially isolated bradycardia on Holter monitoring, which persists with progression to daytime events in longer-lasting studies (SEEQ monitoring or implantable monitor), may require device implantation (figs. 4B and C).19
Among the study limitations are those inherent to the design itself. As an observational study, the results reflect what happens in the real world. The study population is heterogenous in age as well as in clinical characteristics, which affects the results since the probability of this population¿s having an arrhythmia is different from that of experimental study populations with stricter inclusion criteria. However, it is an approximation of what occurs in daily practice, and therefore can provide substantial information regarding the usefulness of this diagnostic method, as well as criteria for choosing the population that will most benefit from its use.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FinancingThis study was sponsored by Fundarritmia - Fundación Cardiovascular.
Conflict of interestsNone.