




In Latin America is not known for certain the quantity or quality of therapeutic communities (TCs) available in the region. The objective of this study is to describe and quantify the quantity and quality of the existing TCs in 5 different countries.
DesignA multicenter quantitative description of the TCs was conducted in Argentina, Brazil, Colombia, Mexico and Peru.
MethodsA survey was realized through the TCs regulatory entities of each country that accepted to participate in the study.
ResultsOf the 285 TCs identified in the 5 countries, 176 (62%) accepted to participate in this study. The TCs quality vas evaluated according to the scoring system stablished by De Leon, finding that 70% of the facilities have scores of 11/12 or 12/12 using these criteria. We also found that the majority of the De Leon criteria are known by more than 90% of the institutions, however, the dimensions of “separation of the community” and “encounter groups between residents” were the least known with 63 and 85% respectively. The main reasons for abandonment of TCs were “not accepting the rules of the institution”, “lack of money” and “not feeling comfortable with the facilities”. 98% of the TCs provided services to other substance abuse problems, 94% for alcohol and 40% for other types of substances.
ConclusionsThe majority of the TCs identified in our sample meet the quality criteria stablished by De Leon, mostly providing services for substance abuse. However, they should put in place additional policies to improve the unfulfilled conditions and investigate the reasons for the dissatisfaction and abandonment of these institutions.
En Latinoamérica no se conoce a ciencia cierta la cantidad o la calidad de las comunidades terapéuticas disponibles en los distintos países de la región. El objetivo de este estudio es identificar y describir la cantidad y la calidad de las comunidades terapéuticas existentes en 5 países de la región.
DiseñoSe realizó un estudio multicéntrico descriptivo cuantitativo de las comunidades terapéuticas en Argentina, Brasil, Colombia, México y Perú.
MétodosMediante las entidades reguladoras de las comunidades terapéuticas de cada país, se realizó una encuesta a las que aceptaran participar en el estudio.
ResultadosDe las 285 comunidades terapéuticas identificadas en los 5 países, 176 (62%) aceptaron participar en el estudio. La calidad de las comunidades terapéuticas se evaluó por las puntuaciones establecidas con los criterios de De León; se encontró que el 70% de las instituciones tienen puntuaciones de 11/12 o 12/12 según estos criterios. También se encontró que cumplen la mayoría de lo criterios de De León más del 90% de las instituciones; sin embargo, las dimensiones «separación de la comunidad» y «grupos de encuentro entre residentes» fueron los menos cumplidos (el 63 y el 85% de las comunidades respectivamente). Las principales razones de abandono de las comunidades terapéuticas fueron no aceptar las normas de la institución, falta de recursos económicos y no sentirse a gusto con ella. El 98% de las comunidades terapéuticas prestaban servicios para problemas de abuso de otras sustancias, el 94% para abuso de alcohol y el 40% para otros tipos de abusos.
ConclusionesLa mayoría de las comunidades terapéuticas identificadas en nuestra muestra cumplen los criterios de calidad establecidos por De León, y en su gran mayoría prestan servicios para abuso de sustancias, pero deben instaurarse políticas para mejorar las condiciones no cumplidas e indagar los motivos de las disconformidades y el abandono de estas instituciones.
The substance use disorders are among the most complex mental diseases due to disturbances generated in the homeostasis of the body, in addition to compromising the different dimensions of the subject: labor, social, cognitive, emotional, among others;1 abuse or dependence of these substances generates disabilities in patients and attendants, which can deteriorate the patients quality of life and even lead to death,2,3 Despite the many teaching and education campaigns, consumption of both legal and illegal substances has been maintained, and even has become a documented comorbidity in other mental illnesses, often in patients infected with HIV virus and teens.3-5
In a study conducted in Latin America in 2011 by the United Nations Office on Drugs and Crime, which included the collaboration of 7 countries, the prevalence of psychoactive substances in patients attending emergency rooms at the institutions included in the study were evaluated. Among the results obtained it was found that the most consumed substance was tobacco, followed by alcohol and marijuana, which were common findings in all the countries participating.6-8
The management of patients with substance abuse or dependence is aimed at helping the patient to abandon the drugs seeking and compulsive use; however, the treatment of these diseases tend to be long and includes bad adhesions, partly because patients who choose to undergo treatment are chronic users and in many cases have experienced failures in previous treatments. The duration of treatment in patients with such diseases reported relapse rates of up to 40 or 50%, so the treatment must be made on more than one occasion.9
There are different ways to handle substance abuse, among which are the use of therapeutic communities (TCs), which are defined as self-help programs for abandonment of harmful substance use behaviors and health recovery the patient via an individual personal growth, which is performed based on separating the subject from society submitting it to a residential program in a specific community with a qualified professional staff and other patients suffering from the same diseases or substance abuse problems.10,11
Trying to establish the standards by which must abide the TCs, authors such as De Leon established a number of criteria that must be present in each of these institutions, in order to ensure better quality in the services provided to patients. These criteria include a therapeutic plan, activities undertaken and even the communities’ staff organization.
Due to the worldwide TCs boom, there have been various models of these; however, not all have all the quality standards suggested by the World Federation of Therapeutic Communities, which could result in that not all programs have the same success and relapses rates.12 These has questioned the effectiveness of the TCs, however, via systematic reviews and meta analyzes, it was found that more studies are needed, however there is evidence to conclude that there is benefit on this therapy for the treatment of persons addicted to psychoactive substances. At the same time they emphasize that it is not possible to tell whether there is a better model, due to the paucity of studies used to compare them.12-14So, it is necessary to evaluate the presence and availability of TCs worldwide, in order to assess the quality of them, and design policies and recommendations improving existing TCs, besides presenting this treatment method in a more uniform and organized way to patients and their families. First, a multicenter study that allows to describe quantitatively and qualitatively TCs available in 5 Latin American countries is made, and for which we had the support of the Latin American Federation of Therapeutic Communities (FLACT), TCs regulator in the region.
MethodsA multicenter descriptive study of quantitative characteristics, including 5 countries in Latin American, was performed. These countries were Brazil (Provincia de Sao Pablo), Mexico (Provincia de Jalisco), Argentina, Peru and Colombia. Through the FLACT or the competent entity in each country, we contacted the respective national organizations responsible for the TCs regulation in order to identify the TCs registered for 2012. Once identified, we tried to contact them through different media for inviting them to participate in the study, with a timeout response of 7-8 weeks.
If we had success, an email or an envelope containing the questionnaire (adapted to each country), cover letters from the main investigator, the FLCAT president, the TCs president at a national associated level was sent; or a phone call from the local study coordinators of each country was made.
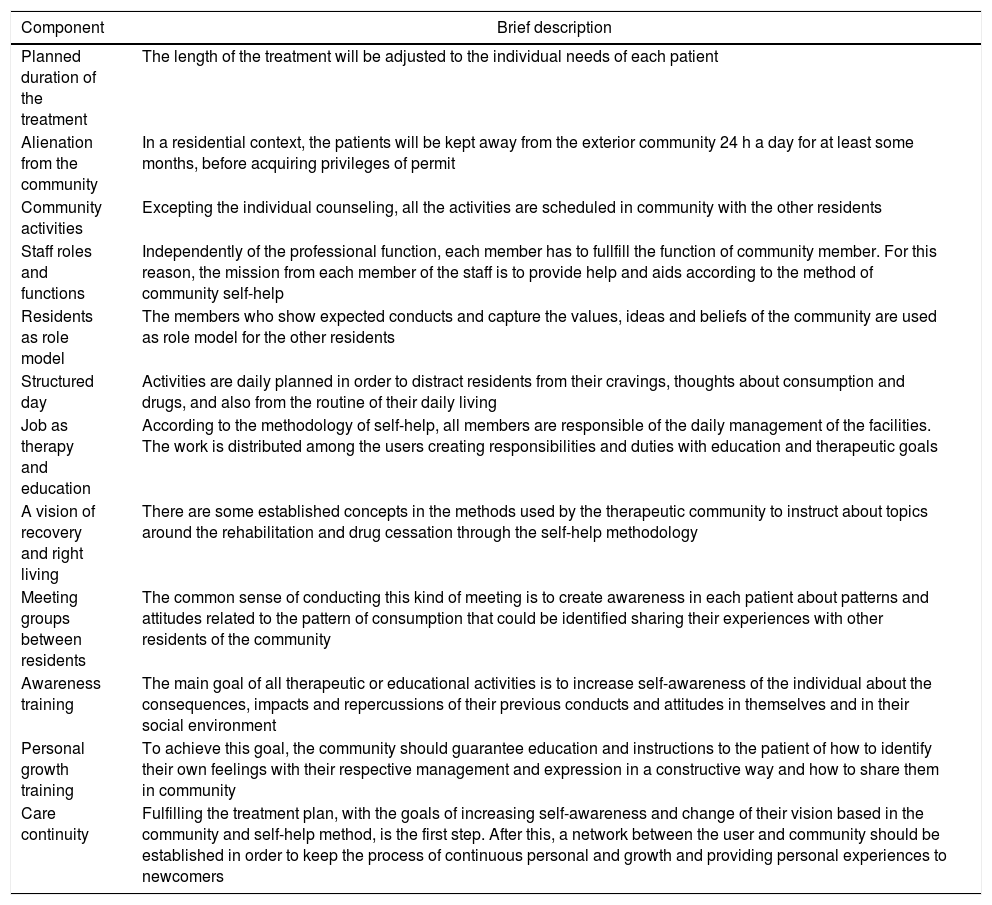
The questionnaire sent to each of TCs included a module evaluating compliance with the criteria established by De Leon 10 (Table 1), reviewing the quality of the institution and assigning a score of 1 if the community fulfilled the criteria and 0 if not, with a maximum added score of 12 points. In addition, questionnaires about patient flow, facility infrastructure, health services provided, the reasons why the patients leave the treatment, and the main diseases treated were sent. This was a self-evaluation process that was answered and returned by each of the director of the participant communities. Like any self-evaluation process, there were some biases such as the alteration of self-perception, either in a positive or negative way.
De Leon criteria.
| Component | Brief description |
|---|---|
| Planned duration of the treatment | The length of the treatment will be adjusted to the individual needs of each patient |
| Alienation from the community | In a residential context, the patients will be kept away from the exterior community 24 h a day for at least some months, before acquiring privileges of permit |
| Community activities | Excepting the individual counseling, all the activities are scheduled in community with the other residents |
| Staff roles and functions | Independently of the professional function, each member has to fullfill the function of community member. For this reason, the mission from each member of the staff is to provide help and aids according to the method of community self-help |
| Residents as role model | The members who show expected conducts and capture the values, ideas and beliefs of the community are used as role model for the other residents |
| Structured day | Activities are daily planned in order to distract residents from their cravings, thoughts about consumption and drugs, and also from the routine of their daily living |
| Job as therapy and education | According to the methodology of self-help, all members are responsible of the daily management of the facilities. The work is distributed among the users creating responsibilities and duties with education and therapeutic goals |
| A vision of recovery and right living | There are some established concepts in the methods used by the therapeutic community to instruct about topics around the rehabilitation and drug cessation through the self-help methodology |
| Meeting groups between residents | The common sense of conducting this kind of meeting is to create awareness in each patient about patterns and attitudes related to the pattern of consumption that could be identified sharing their experiences with other residents of the community |
| Awareness training | The main goal of all therapeutic or educational activities is to increase self-awareness of the individual about the consequences, impacts and repercussions of their previous conducts and attitudes in themselves and in their social environment |
| Personal growth training | To achieve this goal, the community should guarantee education and instructions to the patient of how to identify their own feelings with their respective management and expression in a constructive way and how to share them in community |
| Care continuity | Fulfilling the treatment plan, with the goals of increasing self-awareness and change of their vision based in the community and self-help method, is the first step. After this, a network between the user and community should be established in order to keep the process of continuous personal and growth and providing personal experiences to newcomers |
Once the answers from each of the TCs were obtained, this data was collected on a Microsoft Excel document, with the subsequent calculation of rates and proportions, and finally we generate the respective charts and organized summaries.
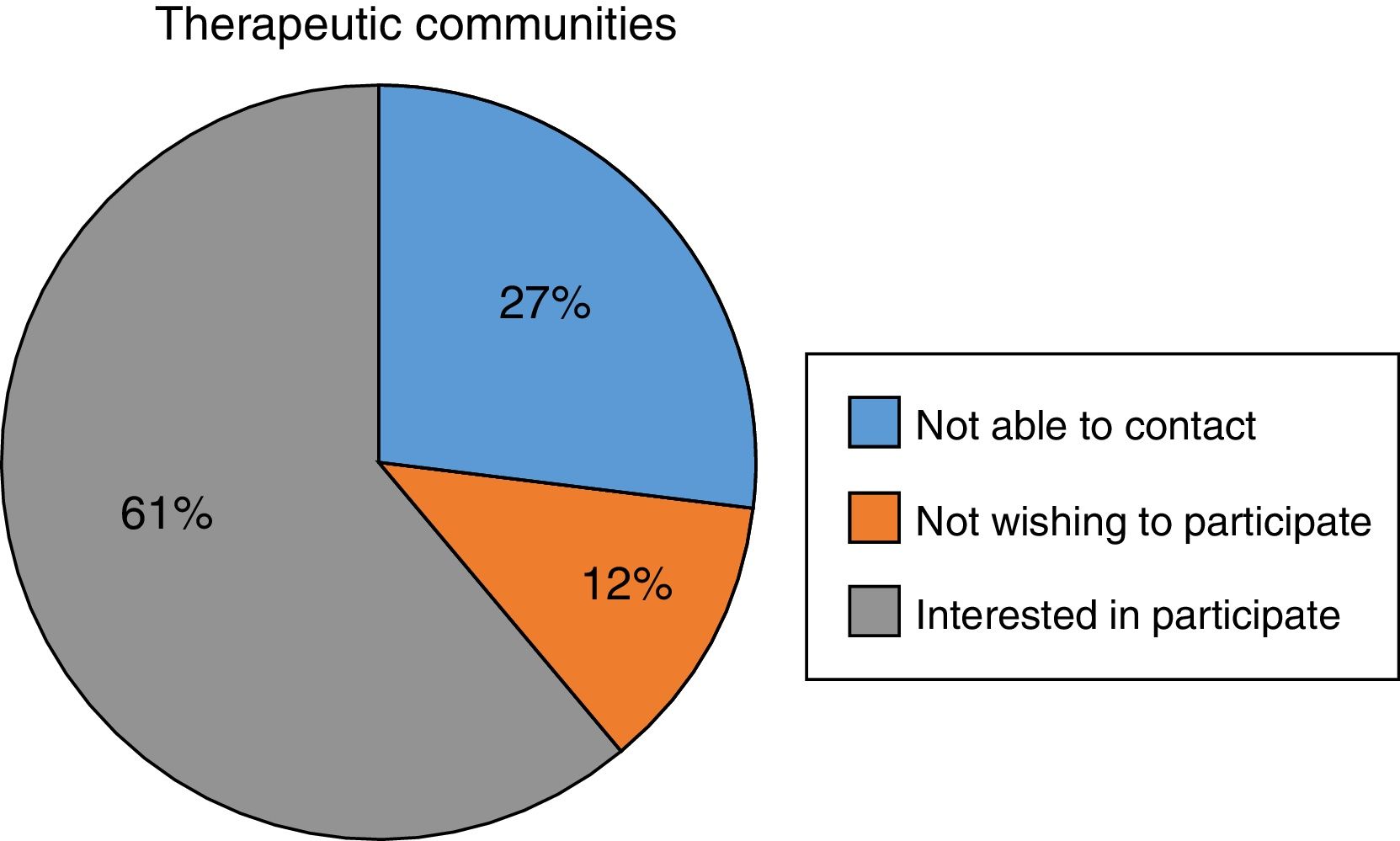
ResultsTherapeutic communities identified and participation in the studyA total of 285 TCs were identified in the 5 countries, with an overall participation rate of 62% (n=176), the country with the highest rate of acceptance was Mexico with 100%; Brazil had the lowest participation rate with 46.5%. Was not possible to contact by any means 27% (n=77) of the TCs, and 11% (n=32) did not wish to participate in the study (figure 1). Table 2 shows the distributions and answers of TCs classified by country.

Distribution of therapeutic communities and their respective responses, by country.
| Brazil | Colombia | Mexico | Peru | Argentina | Total | |
|---|---|---|---|---|---|---|
| Overall, n | 43 | 68 | 20 | 101 | 53 | 285 |
| Not able to contact, n (%) | 3 (7.0) | 18 (26.5) | 0 | 54 (53.5) | 2 (4.0) | 77 (27.0) |
| Not wishing to participate, n (%) | 20 (46.5) | 1 (1.5) | 0 | 0 | 11 (21.0) | 32 (11.0) |
| Willing to participate, n (%) | 20 (46.5) | 49 (72.1) | 20 (100) | 47 (46.5) | 40 (75.0) | 176 (62.0) |
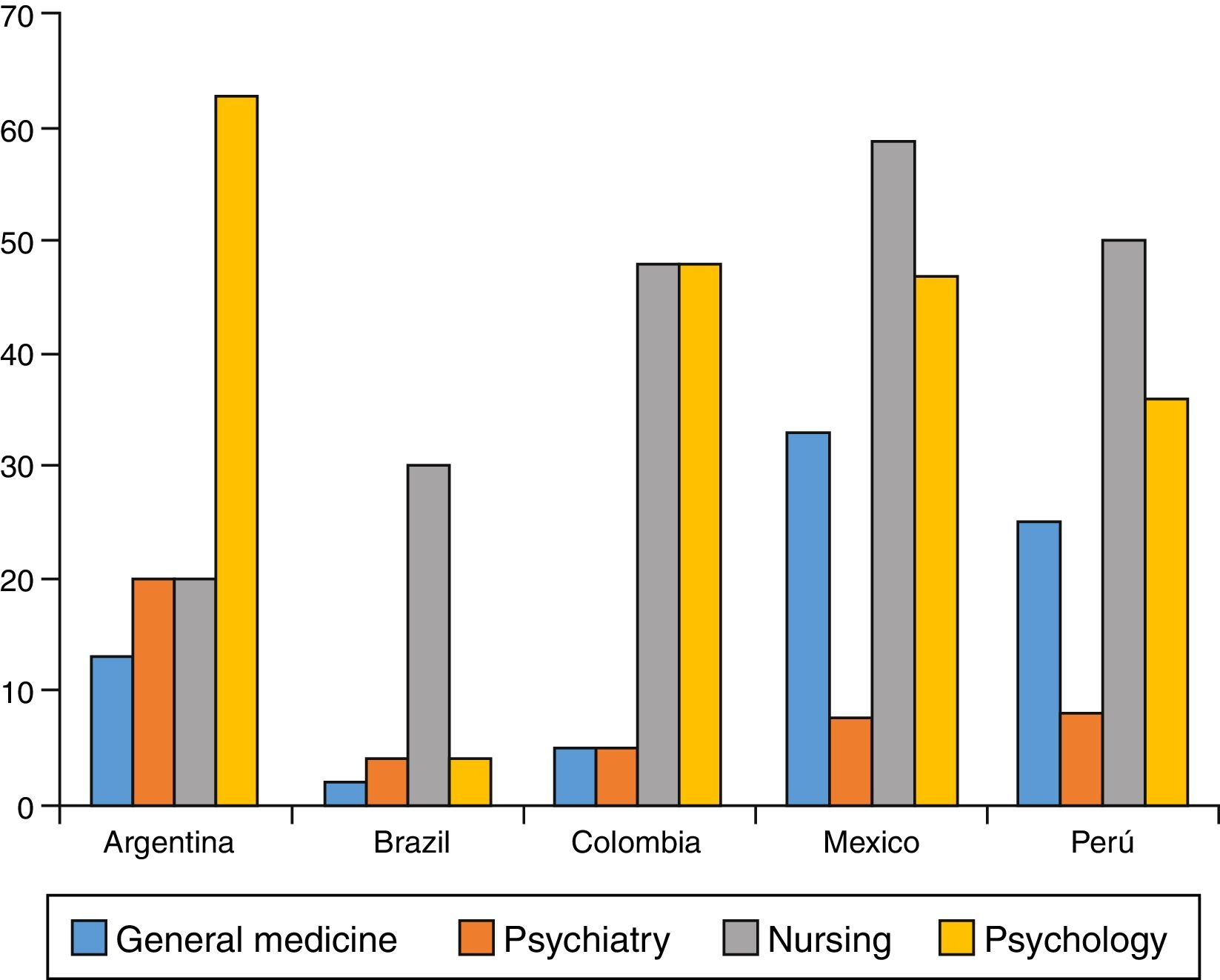
Health services outlined in our questionnaire included the staff's weekly schedule in general medicine, psychology, psychiatry and nursing. Nursing worked longer hours, with an average of 41 h/week, with values ranging between 4 to 168 h/week, followed by psychology services, that had a workload of 39 h/week. Psychiatry had the lowest time intensity, with an average of 9 h/week ranging between 4 h/week in Brazil to 20 h/week in Argentina. Figure 2 shows the weekly different time intensities depending on the country.
Abuse problems treated
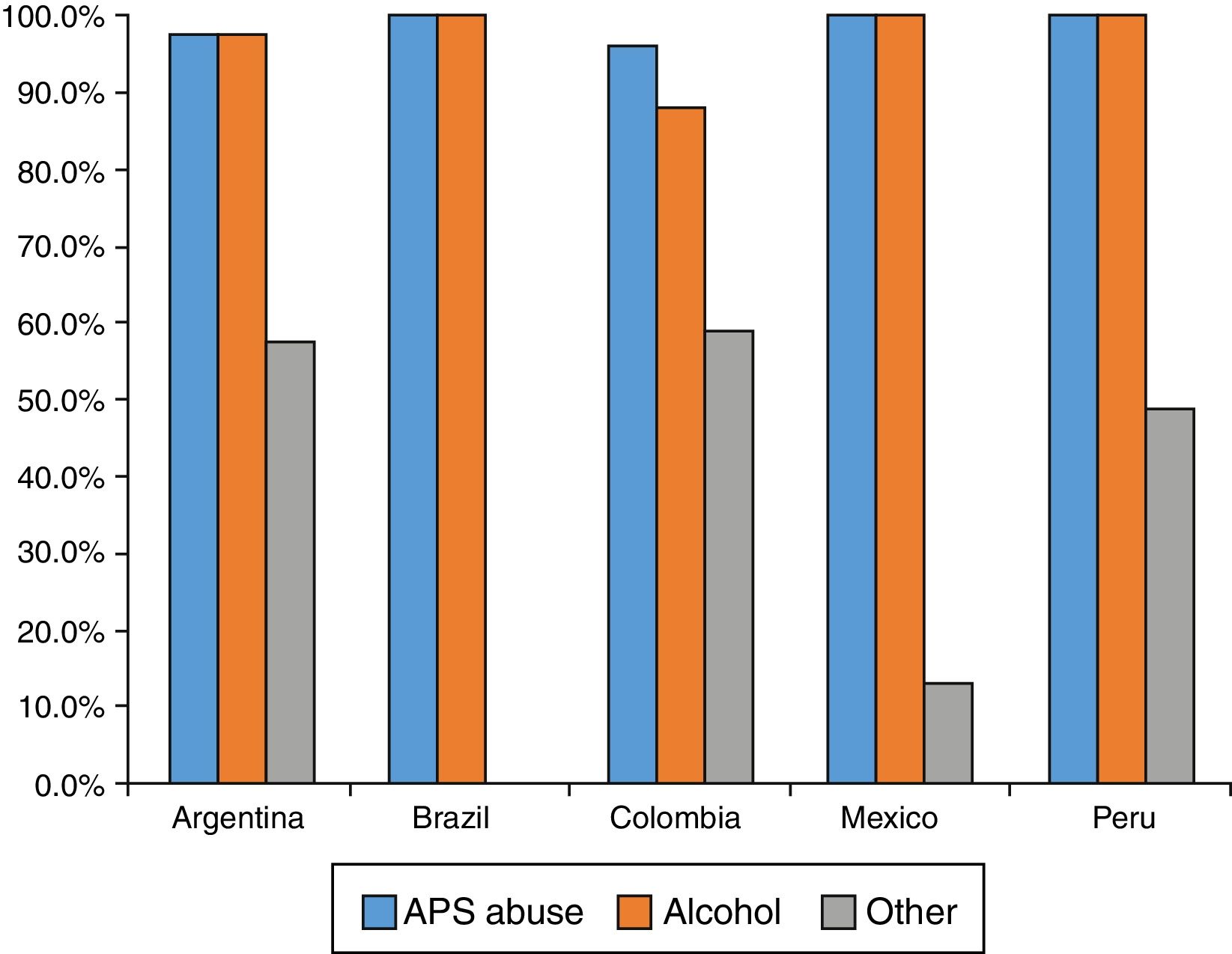
Regarding the type of disorders treated, patients with disorders of substance abuse was the most reported, accounting for 98% (n=170) of the TCs, followed by alcohol abuse treatment with 94% (n=164), and 40% (n=70) of the TCs treated other abuses including compulsive gambling, sex offenders and law offenders. Figure 3 shows the various abuse problems treated by country.
Abandonment reasons
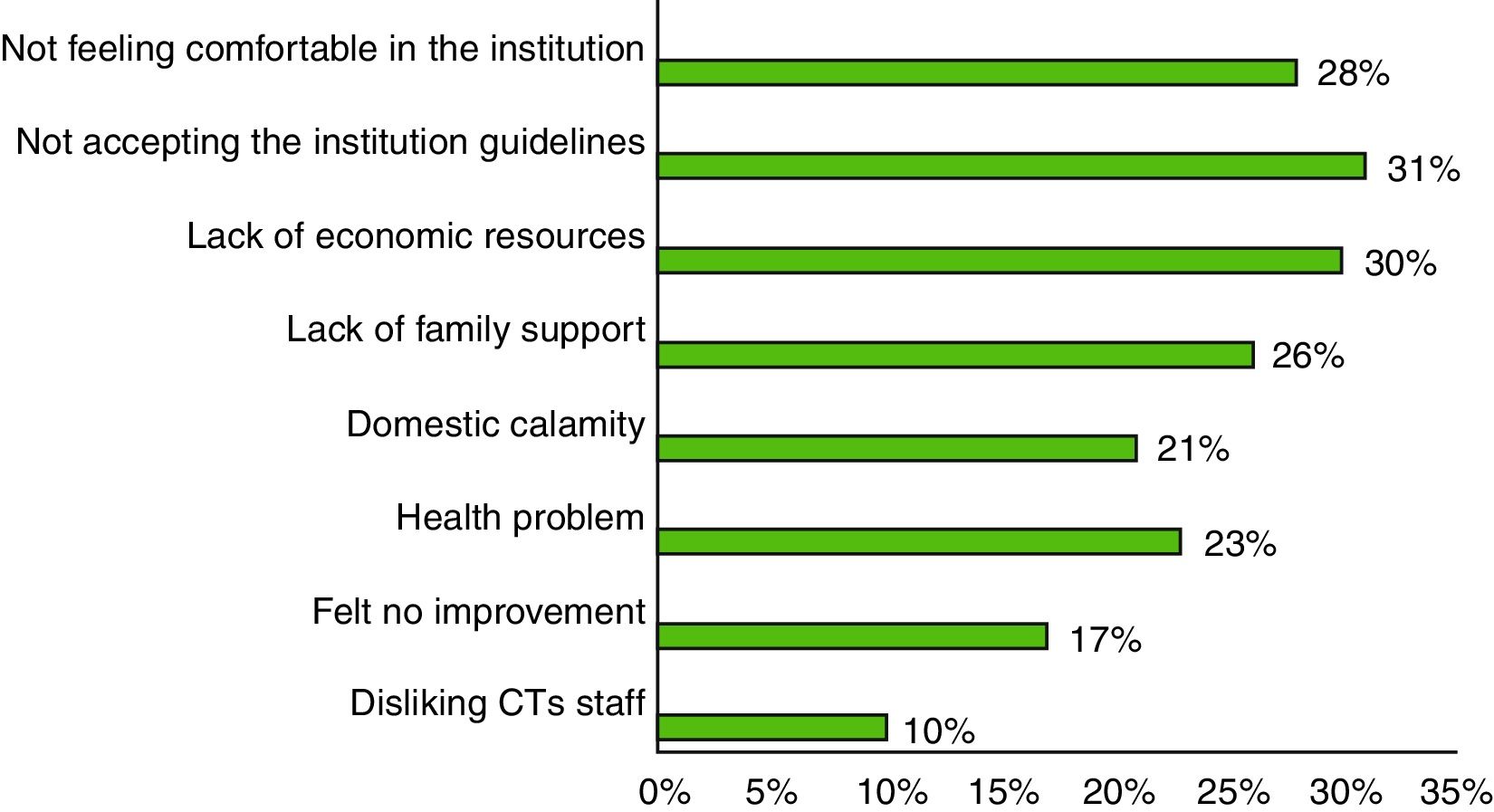
The most common reasons for patients to leave the treatment were similar in all countries, being the main one “not accepting institution guidelines” (31%), followed by “lack of financial resources” (30%), and “not feeling good in the institution” (28%). Less frequent reasons were also homogeneous across countries; the most uncommon one was not liking the staff of the TC (10%) (figure 4).
De Leon criteria individual score
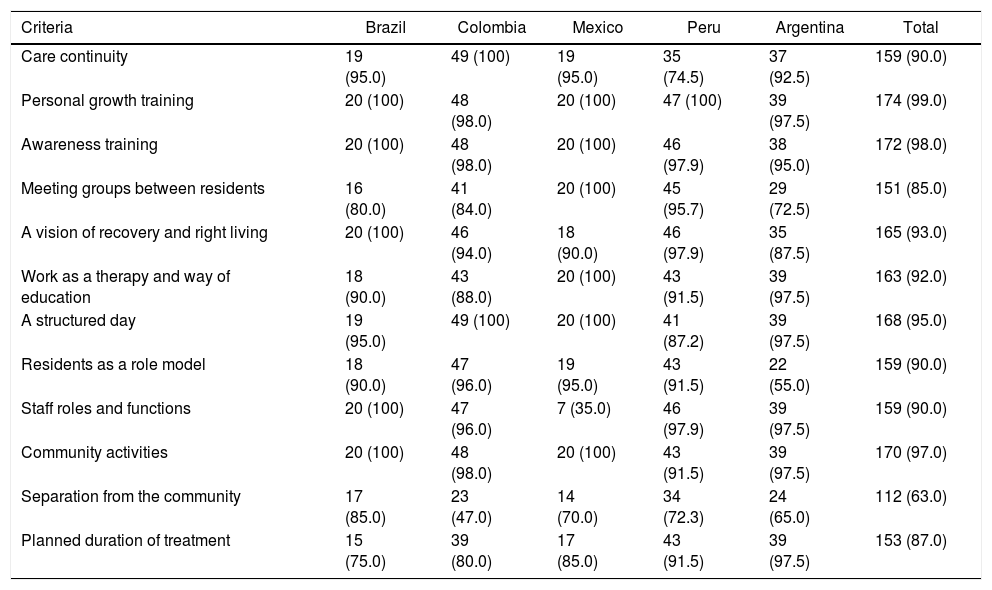
Individual performance results for each of the De Leon criteria which were showing the highest and lowest compliance by each TC were accounted (Table 3). Most criteria were met by more than 90% of TCs in the sample; the most frequently met in the 5 countries were “community activities”, “awareness training” and “personal growth training”. The least accomplished criteria were highly variable between countries, being “planned duration of treatment” (75%) in Brazil, “separation from the community” (47%) in Colombia, “staff roles and functions” (35%) in Mexico, “separation of the community” (72.3%) in Peru, and “residents as a role model” (55%) in Argentina.
Compliance with individual De Leon criteria.
| Criteria | Brazil | Colombia | Mexico | Peru | Argentina | Total |
|---|---|---|---|---|---|---|
| Care continuity | 19 (95.0) | 49 (100) | 19 (95.0) | 35 (74.5) | 37 (92.5) | 159 (90.0) |
| Personal growth training | 20 (100) | 48 (98.0) | 20 (100) | 47 (100) | 39 (97.5) | 174 (99.0) |
| Awareness training | 20 (100) | 48 (98.0) | 20 (100) | 46 (97.9) | 38 (95.0) | 172 (98.0) |
| Meeting groups between residents | 16 (80.0) | 41 (84.0) | 20 (100) | 45 (95.7) | 29 (72.5) | 151 (85.0) |
| A vision of recovery and right living | 20 (100) | 46 (94.0) | 18 (90.0) | 46 (97.9) | 35 (87.5) | 165 (93.0) |
| Work as a therapy and way of education | 18 (90.0) | 43 (88.0) | 20 (100) | 43 (91.5) | 39 (97.5) | 163 (92.0) |
| A structured day | 19 (95.0) | 49 (100) | 20 (100) | 41 (87.2) | 39 (97.5) | 168 (95.0) |
| Residents as a role model | 18 (90.0) | 47 (96.0) | 19 (95.0) | 43 (91.5) | 22 (55.0) | 159 (90.0) |
| Staff roles and functions | 20 (100) | 47 (96.0) | 7 (35.0) | 46 (97.9) | 39 (97.5) | 159 (90.0) |
| Community activities | 20 (100) | 48 (98.0) | 20 (100) | 43 (91.5) | 39 (97.5) | 170 (97.0) |
| Separation from the community | 17 (85.0) | 23 (47.0) | 14 (70.0) | 34 (72.3) | 24 (65.0) | 112 (63.0) |
| Planned duration of treatment | 15 (75.0) | 39 (80.0) | 17 (85.0) | 43 (91.5) | 39 (97.5) | 153 (87.0) |
Data presented as n (%).
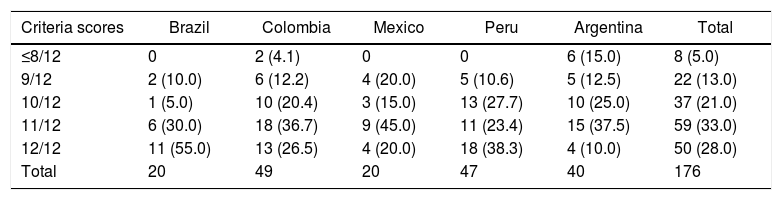
Having the number of criteria met and TCs that reached them, 61% of the participant communities met 11 or all of the De Leon criteria according to the inquiry realized. It can be seen that only in Colombia and Argentina communities that met 8 criteria or less were found, while in Brazil more than half of the communities surveyed met the 12 criteria established in our inquiry (Table 4).
Overall quality of therapeutic communities according to the De Leon criteria.
| Criteria scores | Brazil | Colombia | Mexico | Peru | Argentina | Total |
|---|---|---|---|---|---|---|
| ≤8/12 | 0 | 2 (4.1) | 0 | 0 | 6 (15.0) | 8 (5.0) |
| 9/12 | 2 (10.0) | 6 (12.2) | 4 (20.0) | 5 (10.6) | 5 (12.5) | 22 (13.0) |
| 10/12 | 1 (5.0) | 10 (20.4) | 3 (15.0) | 13 (27.7) | 10 (25.0) | 37 (21.0) |
| 11/12 | 6 (30.0) | 18 (36.7) | 9 (45.0) | 11 (23.4) | 15 (37.5) | 59 (33.0) |
| 12/12 | 11 (55.0) | 13 (26.5) | 4 (20.0) | 18 (38.3) | 4 (10.0) | 50 (28.0) |
| Total | 20 | 49 | 20 | 47 | 40 | 176 |
Data presented as n (%).
Our study results evaluate that, at Latin American level, the TCs are highly widespread and established, and are mostly registered in national bodies responsible for regulating them. One of the first findings is that the establishment of the TCs was unrelated to the number of inhabitants of a country, because one with the highest number of inhabitants, like the Brazilian (State of Sao Paulo), had less TCs available than countries with fewer inhabitants, like Peru; this may be because Peru has already conducted several training programs for the use of such strategies 15 or the existence of underreporting of TCs with regulators.
The response rate of the TCs willing to participate was similar to studies done in other places, such as in a study conducted in Europe and USA,16 which had a response rate of approximately 64%, while our study had an average of 61%. This response rate limits the external validity of the data and its ability to identify the strengths and weaknesses of TCs, and with it the development or generation of public health policies to improve these facilities. Among those TCs not responding it can be assumed to have an organization that does not meet the standards for these types of facilities. However, in countries like Colombia some of the not respondents are affiliated with the FLACT, which suggests a minimum quality. Also in Mexico (Estado de Guadalajara) there is a 100% response enabling better decisions.
Another result of our study was the workload of health professionals working in the TCs. Although the results were not very homogeneous, it was found that despite the variability of countries included, the nurse has the highest workload, probably as a result of these professionals performing day and night shifts for proper care the patients. Another highlight was the low workload of the psychiatry specialists, despite being one of the health professionals that should be more involved in the integrated handling of patients with a disorder of abuse or substance dependence.9,14 These findings are consistent with results of studies conducted worldwide, as performed by Jacob et al. (2007), in which it was found that there is a shortage of nurses and trained mental health physician and a deficiency of beds and institutions specializing in management of mental illness.17 Another reasonable explanation is that, despite having specialized professionals, working conditions may not be ideal for them or not have enough budget to hire them for a longer shift.
The pathologies most frequently treated by TCs were substance abuse disorders, followed by alcohol abuse and other kinds of abuse, which varied slightly depending on the country, except in handling those classified as other abuses. This result is in line with global reporting, in which it has been seen that most of the patients treated in these communities is for use or abuse of any substance different to alcohol.15,18
The most common reason for abandonment identified in our study was not to accept the rules of the institution, which is similar to that reported by Lopez-Goñi et al.,19 who encountered the same reason for abandoning these programs. The least frequent reason in our study was not liking the CT staff, a result that was also found by those authors. It is striking that among the reasons for abandonment found in our study, the need to consume drugs or substances was not found among the most prevalent reasons.19,20
The score of the majority of the TCs included in the study exceeds or equals 10 points according to the De Leon criteria, however, is difficult to compare these results with others performed, because this is the first study evaluating the quality of the TCs using these criteria, being the following the most met by the institutions: “community activities”, “personal growth training”, and “establishment of a structured day”; the least met criteria in our sample were “separation of the community” and “residents as a role model”.
In a study conducted in England on TCs, it was found, that although they did not use the De Leon criteria, a similar one was employed and the most met were “behaviors feedback”, “living and learning in community”, and “established staff functions”; and less frequently met were “the lack of personnel”, “groups meeting daily”, and “activities among residents”.21
In another study by Goethal et al. (2011), European and American TCs were compared through the questionnaire of Essential Elements of the Therapeutic Community, evaluating the performance of elements like “TCs perspective”, “structure of treatment”, “community as a therapeutic agent”, and “therapeutic formal elements and processes”. That study found that European TCs met mostly those elements of patient participation and the role of the family in the treatment, especially in the traditional European TCs.16
Among the strengths of our study, it highlights the use of a representative sample of the region, including 5 countries and 174 TCs, which allows us to evaluate and find the similarities and differences between the TCs in the region, becoming one of the larger samples carried out for this type of study. Additionally, it is the first study in Latin America evaluating the quality of the TCs at a regional level, allowing studies to compare our results with other regions of the world, being possible to establish the infrastructure available in the region for the design of future studies on TCs.
Among the weaknesses of our study, we should note the high non-response rate, which was approximately 41%, indicating a lack of collaboration of these institutions to identify all their strengths and weaknesses. Also the methodology of self-reported methodology of each the communities adds bias to the results due to the exclusion of the results of the excluded and communities and also reporting the bias because the directors may avoid informing the negative qualities of their communities. The failure to classify the type of the TCs, that is, if the TC was performed in a prison or if its orientation was merely spiritual or scientific, was not clear in our study, unlike those made in Thailand,18 Europe, and USA,16; however, De Leon criteria numbers 2 and 3 include a spiritual focus, so that much of the TCs met with them infer that participating institutions have a mixed orientation in their processes treatment.
As we can see, the Latin American region has a considerable number of TCs meeting the quality criteria proposed by De Leon, but it is needed to assess the acceptance and usefulness of TCs by its users and working staff. Based on these results, we will lead a second phase exploring the impact generated by TCs in the same 5 countries, whose sample is taken from the TCs identified in this study.
ConclusionsOur study has identified in a representative sample the quantity and quality of the TCs available in our region and their main strengths and weaknesses, which could be used in future studies, and could be useful in the generation of new health policies public to standardize, homogenize and improve treatment plans and management of TCs in Latin America.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial supportThis study was funded by Corporative Foundations, A.C., the United States Embassy in Peru and the Bancolombia S.A.
Conflicts of interestsThe authors have no conflicts of interest to declare for this study.
Special thanks to Brazilian Federation of Therapeutic Communities (FEBRACT), Colombian Federation of Therapeutic Communities (FECCOT), State Council Against Addictions in Jalisco (CECAJ), Mexican Federation of Therapeutic Communities (FEMEXCOT), Developing Life without Drugs (DEVIDA) by the Peruvian Ministry of Health (MOH), Peruvian Association of Therapeutic Communities (PTCA), Centre for Information and Education for the Prevention of Drug Abuse (CEDRO), Argentine Drug Observatory (SEDRONAR), and the Latin American Federation of Therapeutic Communities (FLACT).
