



Using data from the Ministry of Health of Colombia, we performed an analysis of prevalence and general demographic characteristics of patients with inflammatory myopathies, with data from 2012 to 2018.
Materials and methodsA descriptive cross-sectional study based on data from the Ministry of Health of Colombia. We used as key terms the diagnostic codes of the International Manual of Diseases related to the diagnosis of inflammatory myopathies.
ResultsWe founded 12,401 individuals with a diagnosis of inflammatory myopathy and estimated an overall prevalence of 25.7 cases per 100,000 inhabitants. This diagnosis is more common in the age group of 65–69 years, and in the female population (64%), with a female-to-male ratio 1.79:1. In addition, we calculated a prevalence of 15.1 cases per 100,000 inhabitants for dermatomyositis and 7.3 cases per 100,000 inhabitants for polymyositis (based on a total population of 48,203). There is little information on the epidemiology of myopathies in Latin America, and records are essential to know their behaviour in populations. In Colombia, the Ministry of Health collects information from the health system, which has nearly universal coverage (around 95%). This information makes it possible to carry out epidemiological studies on different diseases. For the present study we analysed the available data on inflammatory myopathies in Colombia.
ConclusionsThe present work describes for the first time the demographic characteristics of inflammatory myopathies in the Colombian population based on official data from the Ministry of Health, where the most frequent was dermatomyositis and a predominance in the female population was evidenced.
A partir de los datos del Ministerio de Salud de Colombia, se realizó un análisis de la prevalencia y las características demográficas generales de los pacientes con miopatías inflamatorias, con los registros correspondientes a los años 2012 a 2018.
Materiales y métodosEstudio descriptivo de corte transversal en el que se tomaron los datos del Ministerio de Salud de Colombia, utilizando como términos clave los códigos diagnósticos del manual internacional de enfermedades relacionados con el diagnóstico de miopatías inflamatorias.
ResultadosSe documentaron 12.401 individuos con diagnóstico de miopatía inflamatoria, con una prevalencia global estimada de 25,7 casos por 100.000 habitantes, siendo más frecuente en el grupo de 65 a 69 años, con un predominio de afectación en población femenina (64%) y una relación mujer a hombre de 1,79:1. Adicionalmente, se calculó una prevalencia de 15,1 casos por 100.000 habitantes para dermatomiositis y de 7,3 casos por 100.000 habitantes para polimiositis (con base en una población total de 48.203.405).
ConclusionesEste trabajo describe por primera vez las características demográficas de las miopatías inflamatorias en la población colombiana, a partir de los datos oficiales del Ministerio de Salud, donde la más frecuente fue la dermatomiositis, y se evidencia un predominio en población femenina.
Idiopathic inflammatory myopathies (IIMs) are a group of diseases that are characterized by sharing three characteristics: inflammatory involvement of striated muscle, acquired diseases and potentially treatable. They are differentiated in 3 entities: dermatomyositis (DM), polymyositis (PM) and myositis by inclusion bodies, given the histological and immunological findings, treatment response and prognosis.1–3
In Colombia, a work was carried out using Community Oriented Program for Control of Rheumatic Diseases (COPCORD) methodology, in which a prevalence of 0.03% (95% CI 0.00–0.23%) was estimated.4 However, the distribution in the different departments of the country is unknown, and there is no individual analysis of each IIM; for this reason, in this work we present epidemiological data based on official statistics to obtain demographic information on Colombian patients with IMM from the official statistics of the Ministry of Health.
Materials and methodsThe Colombian health system is based on public financing and a mixed public and private provision, with a nearly universal coverage (around 95%).5 The Ministry of Health of Colombia has developed an information collection and storage tool, called the Comprehensive Social Protection Information System (SISPRO), which has four components: health, pensions, labor risks and social promotion. In the first component, the basic and minimum data that the General Social Security System in Health requires for management, regulation and control processes are stored and processed. This data is taken from the Individual Health Services Delivery Registry (RIPS). The information contained in these databases is accessible to the public. The data to carry out the present study were obtained by consulting the online dynamic tables of the Ministry of Health. We obtained information from January 1, 2012 to December 31, 2018. Following the STROBE guidelines for observational studies, we conducted an analysis of RIPS databases, using the codes of the International Classification of Diseases (ICD-10) for IIMs (M330, M331, M332, M339); we also analyzed variables such as sex, type of insurance and distribution in five-year groups, according to official data of the National Administrative Department of Statistics (DANE), based on the projections of the 2005 national census.6 To calculate the prevalence in Colombia we did an analysis by five-year groups. The SISPRO database diagnostic criteria for IIMs are not standardized and depend on clinical and diagnostic judgment of each physician when registering a patient with a CIE-10 IIM-related code. We included patients registered with an IIM diagnosis as “main diagnosis”. The diagnosis of IMM for the SISPRO database is made by the diagnosis established by a general practitioner or specialist during any outpatient or inpatient medical care. If there are multiple diagnoses, there is a possibility that these are recorded by the attending physician. It is important to note that the Colombian health system is one with the highest coverage in Latin America (45.2 million; the Colombian population is estimated at 48.2 million), according to the Ministry of Health's latest measurement in June 2019.5 This high rate of coverage is important to highlight because being almost universal, allows us to infer that there are few patients with IMM that would be beyond the scope of this study.
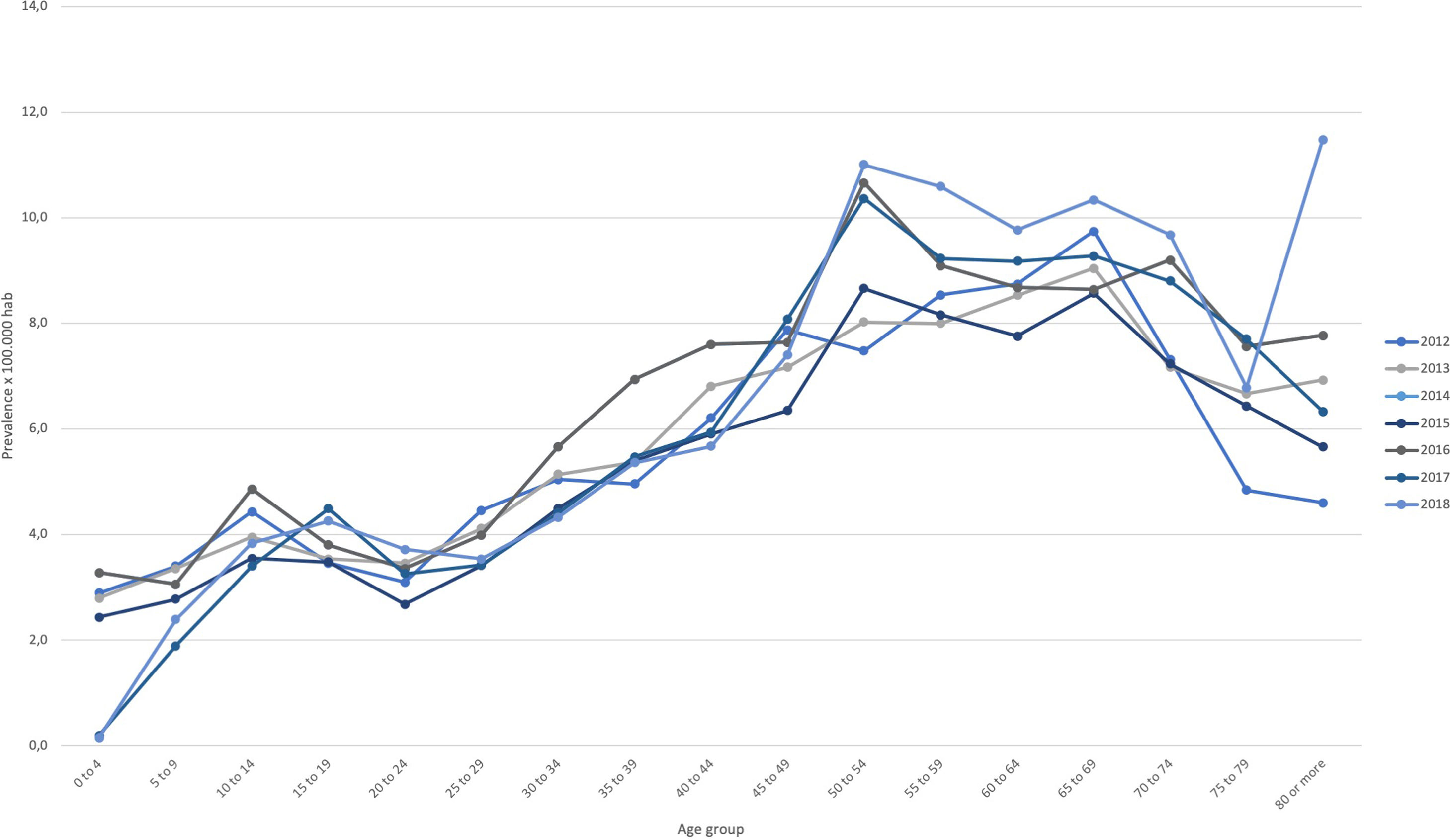
ResultsWe identified 12,401 cases (“people attended”) with a main diagnosis of IIM, which allowed to calculate a prevalence 25.7 cases per 100,000 inhabitants. In the pathology-based differential analysis, 7277 cases of DM were registered, and we estimated a prevalence of 15.1 cases per 100,000 inhabitants. In the case of PM, 3507 cases were registered, with a prevalence of 7.3 cases per 100,000 inhabitants. An analysis of the prevalence of IIM by five-year groups shows a higher prevalence in the 65–69 years group (Table 1 and Fig. 1).
Patients with a main diagnosis of inflammatory myopathy according to age group between 2012 and 2018 in Colombia.
| Age group | Total patients* | Total Prev | DM¿ | PMΔ | Prev DM* | Prev PM* |
|---|---|---|---|---|---|---|
| 0–4 | 684 | 15.8 | 586 | 24 | 1.2 | 0.0 |
| 5–9 | 721 | 16.9 | 585 | 77 | 1.2 | 0.2 |
| 10–14 | 1003 | 23.4 | 819 | 102 | 1.7 | 0.2 |
| 15–19 | 971 | 22.3 | 685 | 157 | 1.4 | 0.3 |
| 20–24 | 784 | 18.3 | 499 | 181 | 1.0 | 0.4 |
| 25–29 | 829 | 20.9 | 491 | 218 | 1.0 | 0.5 |
| 30–34 | 930 | 26.3 | 516 | 295 | 1.1 | 0.6 |
| 35–39 | 938 | 29.3 | 483 | 326 | 1.0 | 0.7 |
| 40–44 | 986 | 34.2 | 470 | 357 | 1.0 | 0.7 |
| 45–49 | 1105 | 38.3 | 547 | 375 | 1.1 | 0.8 |
| 50–54 | 1252 | 46.7 | 581 | 449 | 1.2 | 0.9 |
| 55–59 | 1059 | 47.7 | 484 | 398 | 1.0 | 0.8 |
| 60–64 | 843 | 48.8 | 376 | 310 | 0.8 | 0.6 |
| 65–69 | 689 | 52.7 | 284 | 289 | 0.6 | 0.6 |
| 70–74 | 468 | 50.5 | 201 | 183 | 0.4 | 0.4 |
| 75–79 | 289 | 42.2 | 118 | 118 | 0.2 | 0.2 |
| 80 or more | 291 | 42.2 | 121 | 101 | 0.3 | 0.2 |
| Total | 12.401 | 25.7 | 7.277 | 3.507 | 15.1 | 7.3 |
Prev: prevalence; DM: dermatomiositis; PM: polimiositis.
The “Total patients” column corresponds to the number of people attended at some time during the period studied with diagnosis of any inflammatory myopathy. The prevalence is calculated with the average population for the period as denominator per 100,000 population.

Regarding the distribution by sex, a jointly analysis of IIMs we founded is more frequently in women (77% of cases), with a female-to-male ratio of 3.27:1. In the individual analysis, we observed 63% of DM diagnoses were in women, with a female-to-male ratio of 1.73:1. In the case of PM, 64% of the diagnoses were in women, with a female-to-male ratio of 1.84:1. Table 2 shows the number of patients according to sex and age group.
Patients with a main diagnosis of inflammatory myopathy by gender and age group in the 2012–2018 period.
| Age group | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| IIM patients | Total prevalence† | DM prevalence | PM prevalence | IIM patients | Total prevalence† | DM prevalence | PM prevalence | |
| 0–4 | 337 | 15.2 | 13.0 | 0.7 | 346 | 16.4 | 14.1 | 0.4 |
| 5–9 | 342 | 15.7 | 12.4 | 2.2 | 367 | 17.6 | 14.6 | 1.3 |
| 10–14 | 428 | 19.6 | 15.9 | 2.1 | 567 | 27.1 | 22.2 | 2.7 |
| 15–19 | 376 | 16.9 | 11.4 | 3.2 | 592 | 27.8 | 20.3 | 4.0 |
| 20–24 | 273 | 12.4 | 7.1 | 3.6 | 510 | 24.3 | 16.3 | 4.9 |
| 25–29 | 262 | 13.1 | 8.1 | 3.5 | 567 | 29.0 | 16.8 | 7.6 |
| 30–34 | 337 | 19.4 | 10.3 | 6.6 | 593 | 32.9 | 18.7 | 10.0 |
| 35–39 | 299 | 19.2 | 9.5 | 7.7 | 639 | 38.8 | 20.3 | 12.5 |
| 40–44 | 279 | 20.1 | 9.6 | 7.9 | 707 | 47.3 | 22.6 | 16.5 |
| 45–49 | 339 | 24.6 | 12.1 | 8.7 | 766 | 50.8 | 25.3 | 16.9 |
| 50–54 | 396 | 31.0 | 14.0 | 12.0 | 856 | 60.9 | 28.6 | 21.1 |
| 55–59 | 331 | 31.6 | 14.9 | 12.0 | 727 | 62.0 | 27.9 | 23.2 |
| 60–64 | 256 | 31.5 | 13.3 | 12.7 | 587 | 64.1 | 29.3 | 22.6 |
| 65–69 | 233 | 38.3 | 14.8 | 15.4 | 456 | 65.3 | 27.8 | 27.9 |
| 70–74 | 176 | 41.7 | 19.4 | 13.7 | 292 | 57.8 | 23.6 | 24.8 |
| 75–79 | 92 | 30.9 | 13.1 | 12.8 | 196 | 50.6 | 20.2 | 20.7 |
| 80 or more | 105 | 37.0 | 16.5 | 10.9 | 184 | 45.4 | 18.0 | 17.3 |
| Total | 4444 | 18.7 | 11.2 | 5.2 | 7933 | 32.5 | 18.9 | 9.3 |
IIM: inflammatory myopathy; DM: dermatomiositis; PM: polimiositis.
Prevalence calculated with the average population of the period as denominator per 100,000 population.
When analyzing the type of coverage that patients have according to the health system affiliation regime, we found that the majority of IIM patients belong to the contributory regime (62%), followed by the subsidized regime (31%), complementary plans (5%) and special regimes (1%).
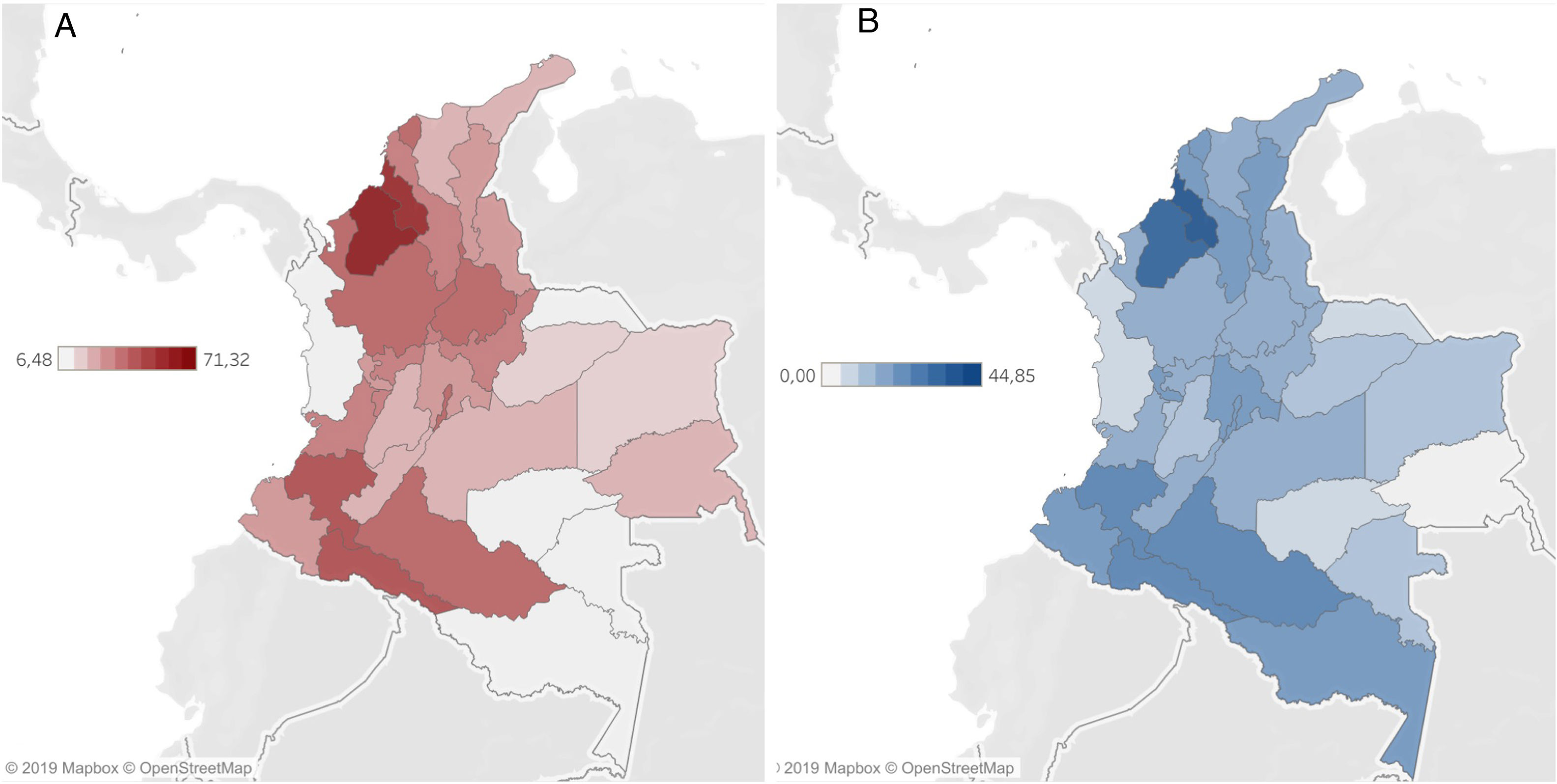
Regarding the distribution of IIM by departments of the country, we found a prevalence range of 0 to 44.8 per 100,000 inhabitants in men, and from 6.48 to 71.32 per 100,000 inhabitants in women (Fig. 2).
Discussion Female. (B) Male.")
Our work collects information on inflammatory myopathies in the Colombian population, using data from the Ministry of Health database. Previously, another work had been developed in Colombia with COPCORD methodology, which showed an IIM prevalence similar to that found in our study (30 cases per 100,000 inhabitants).4 This is interesting because using different methodologies, a similar prevalence estimate was reached, which increases the validity of both works.
There is lacking and limited information on epidemiology of inflammatory myopathies. The existence of different classification criteria and the use of heterogeneous methodologies in the studies makes it difficult to compare results.7,8 Despite this, in a systematic literature review conducted in 2014, it was estimated that the world prevalence of IIM ranges from 2.4 to 33.8 cases per 100,000 inhabitants, and it is striking that only one of the works in this review was carried out in Latin America.8 The study was conducted in Argentina and its results differ from ours, not only because it reports a lower IIM prevalence, but also because it shows that IIMs are less common in women (59% of patients), with an average age of 46.6 years (lower than that reported in Colombia).9
A work carried out in the United States in 2008 based on the insurance model, reports a DM prevalence of 8.7–9.18 per 100,000 (11.24–13.7 in women and 3.26–4.03 in men),10 which is lower than founded in Colombia. On the other hand, PM prevalence in the United States in 2008 was 11.19–15.48 per 100,000 (12.2–18.15 in women and 8.9–9.77 in men),10 more than double the value reported in data of Colombia, maintaining the difference between men and women.
Regarding the female-to-male ratio, other research has shown that IIMs are more common in women, as reported in Pennsylvania (USA),11 with a female-to-male ratio of 2.2:1, as well as a study in Israel with a female-to-male ratio of 1.69:1,12 similar to what was reported in our study.
One of the limitations in different works on the prevalence of myopathies, and ours is not an exception, is the difficulty in differentiating against myopathies that have another etiology, such as inherited disorders, metabolic dystrophies and myopathies, or acquired etiologies, such as rhabdomyolysis, infections and other inflammatory conditions.13
The main limitation of the present work is the possible underreporting or wrong reporting by physicians at the moment of entering the CIE 10 code in the medical records, and the diagnostic criteria used for each case is unknown. However, this data is legally registered in the care of patients in Colombia, and it deserves this type of analysis, which provides valuable information, allowing us to give an idea of the epidemiology of IIMs in our country. Also, there are different methodologies between the studies (i.e. selected cohorts, insurance database, medical records) that could explain the difference between our study and other reported works. Also, this is not the first work that uses this methodology in autoimmune diseases, and the authors has already published other works that showed a correlation between RIPS and other methodologies.14–17
Due to the characteristics of the registry and the fact that there is no criterion to determine which is the “main diagnosis” from one year to another, a variation in the registry may occur. For this reason, it is not possible to calculate the incidence or duration of the disease.17 Likewise, due to the nature of the available data, it is not possible to establish the time of evolution of the disease, the specific clinical characteristics of the patients, their response to treatment, the severity of the disease or the mortality. However, this is an approximation from the statistics of the Colombian Ministry of Health, with which public health policy decisions are made, drugs approval, which is important for a disease that generates a great economic and social impact.
ConclusionsThe present work characterizes IIMs for the first time in the Colombian population and is the second such work in Latin America. The most frequent type of IIM in Colombia is dermatomyositis, with predominance in the female population in the 65–69 years group.
Ethical approvalAll procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The ethical and methodological quality of the study was appraised and approved by the Cómite de Ética e Investigación of the Hospital Universitario San Ignacio and Pontificia Universidad Javeriana.
FundingThe authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors thank their colleagues at Internal Medicine Department at Hospital Universitario San Ignacio for their fruitful discussions and contributions to this work.
