



Rheumatic diseases are the leading cause of permanent disability. The COPCORD model is an effective tool in the determination of the prevalence of diseases. The objective of this study is to estimate the prevalence of rheumatic disease in a Colombian population over 18 years of age.
MethodsA prevalence study was carried out using a probabilistic method of stratified random sampling in three stages: cartographic sectors in each city, selection of the blocks of each sector, and the households of each block. The COPCORD questionnaire adapted for Colombia was applied by standardized interviewers. Confirmation of the diagnosis was made by a rheumatologist with access to all the information.
ResultsOut of a total of 6693 patients that completed the questionnaire, 64% were women. Pain not associated with trauma was reported by 48% of the participants. The most frequent locations were: knees 35%, hands 26%, lumbar spine 20%, and shoulders 16%. Non-specific skeletal muscle discomfort, osteoarthritis, regional appendicular syndrome, and non-inflammatory low back pain, were the most prevalent diseases. Rheumatoid arthritis and chronic inflammatory low back pain were the most common inflammatory conditions. The prevalence of Chikungunya fever was estimated at 6.68%.
ConclusionThe prevalence of rheumatoid arthritis in Colombia is higher than commonly reported, lower than for fibromyalgia and gout, and similar for osteoarthritis, systemic lupus erythematosus and spondyloarthritis. In Colombia these diseases are a public health problem without awareness of their impact on the general population.
Las enfermedades reumáticas son causa frecuente de discapacidad, deterioran la calidad de vida y causan alto gasto en salud. El modelo COPCORD se ha implementado universalmente para estimar su prevalencia. El objetivo es estimar la prevalencia de las enfermedades reumáticas en la población colombiana mayor de 18 años.
MétodosSe realizó un estudio de prevalencia utilizando un método probabilístico de muestreo aleatorio estratificado en 3 etapas: selección de los sectores cartográficos en cada ciudad, selección de los bloques de cada sector y del hogar de cada bloque. El cuestionario COPCORD, adaptado para Colombia, fue aplicado por entrevistadores estandarizados. La confirmación del diagnóstico fue hecha por un reumatólogo con acceso a toda la información.
ResultadosDe un total de 6.693 personas encuestadas el 64% fueron mujeres. El dolor no asociado con trauma fue reportado por el 48% de los participantes. Los sitios más frecuentes fueron rodillas (35%), manos (26%), columna lumbar (20%) y hombros (16%). El malestar musculoesquelético no específico, la osteoartritis, el síndrome de dolor regional apendicular y la lumbalgia no inflamatoria fueron las enfermedades más prevalentes. La artritis reumatoide y la lumbalgia crónica inflamatoria fueron las condiciones inflamatorias más comunes. La fiebre chikungunya afectó al 6,68% de la población.
ConclusiónLa prevalencia de la artritis reumatoide en Colombia es mayor a lo comúnmente reportado, menor para fibromialgia y gota, y similar para osteoartritis, lupus eritematoso sistémico y espondiloartritis. En Colombia, estas enfermedades representan un problema de salud pública sin que exista conciencia de su impacto en la población general.
Osteomuscular and connective tissue diseases are a group of disorders with a diverse demographic, genetic and clinical profile. Although they usually affect the locomotor apparatus, sometimes are accompanied by multiorgan systemic commitment derived from generalized autoimmune phenomena.1 They are characterized by pain, chronic and persistent inflammation, alteration of functional ability and deterioration in quality of life. Several of these diseases are linked with a significant decrease in life expectancy.2
In the past 40 years, it has been documented a 2–4-fold progressive increase in the prevalence of musculoskeletal symptoms3; phenomenon to which the Latin American countries have not been oblivious.4 This increase has represented a significant rise of the costs derived from their medical care.5 Several strategies have been designed to try to impact the public health problem that these disorders represent. One of the most significant was the declaration, by the World Health Organization, of the Bone and Joint Decade for the period comprised between the years 2000 and 2010, which sought to join efforts of governmental and non-governmental organizations in the search for integral solutions to the public health problem that these entities represent.6
The World Health Organization and the International League of Associations of Rheumatology (ILAR) developed the Community Oriented Program for Control of Rheumatic Diseases (COPCORD) as an epidemiologic strategy designed for the identification, prevention and control of the rheumatic diseases in developing countries.7 The strategy consists of 3 stages, the first one identifies the patients with osteomusculoarticular symptoms of non-traumatic origin through a direct interview, classifies the symptoms by pain or limitation with the use of questionnaires and, finally, with the participation of a trained physician, the rheumatologic diagnosis is established. Stages 2 and 3 are addressed to the design of strategies that allow the integral care of patients with these diseases.8
Its use allows to identify the frequency of these diseases, their distribution and potential intervention factors as public health strategies.9 The COPCORD strategy has been implemented in several Latin American countries: Argentina,10 Mexico,11 Guatemala,12 Cuba,13 Peru,14 Venezuela,15 Brazil16 and Ecuador.17 Studies have also been conducted in indigenous populations from Venezuela (Warao, Kariña and Chaima), Mexico (Mixteco, Maya-Yucateco and Rarámuri) and Argentina (Qom).18 In these countries it has been reported a prevalence between 17 and 50%. Osteoarthritis (OA) has been the most frequent disease, and rheumatoid arthritis (RA) ranges between 0.9 and 1.6%.
Epidemiological studies are the base for the determination of the economic impact of the diseases through the estimation of the number of affected individuals. The combination of the prevalence with factors related with the quality of life, the functional limitation and the costs allows to establish the attributable economic impact and burden of these conditions on the macroeconomic variables of the State.5 In developed countries, the costs of the rheumatic diseases can represent between 1 and 3% of the gross domestic product, which constitutes them in a public health problem of high impact.19 In Latin America and Colombia there is little information related to the prevalence, costs and economic impact of these diseases.
The objective of this study is to estimate the prevalence of musculoskeletal manifestations and of the main rheumatic diseases in Colombian population through the implementation of the stage i of the COPCORD strategy.
MethodologyThe study conducted in Mexico during the years 2012–2014 was taken as reference for the development of this study. It was performed the transcultural adaptation and validation of the methodology and screening questionnaire (COPCORD) Mexican version 220 to identify musculoskeletal discomforts and rheumatic diseases, following the guidelines proposed by Beaton et al.21 The population studied consisted of adults over 18 years of age, who had been living in the household surveyed for more than 2 years and who were mentally able to answer the survey and fill out the forms that were included in it. Persons residing in hospitals, military institutions or prisons, as well as individuals unable to answer the interviews or questionnaires were excluded.
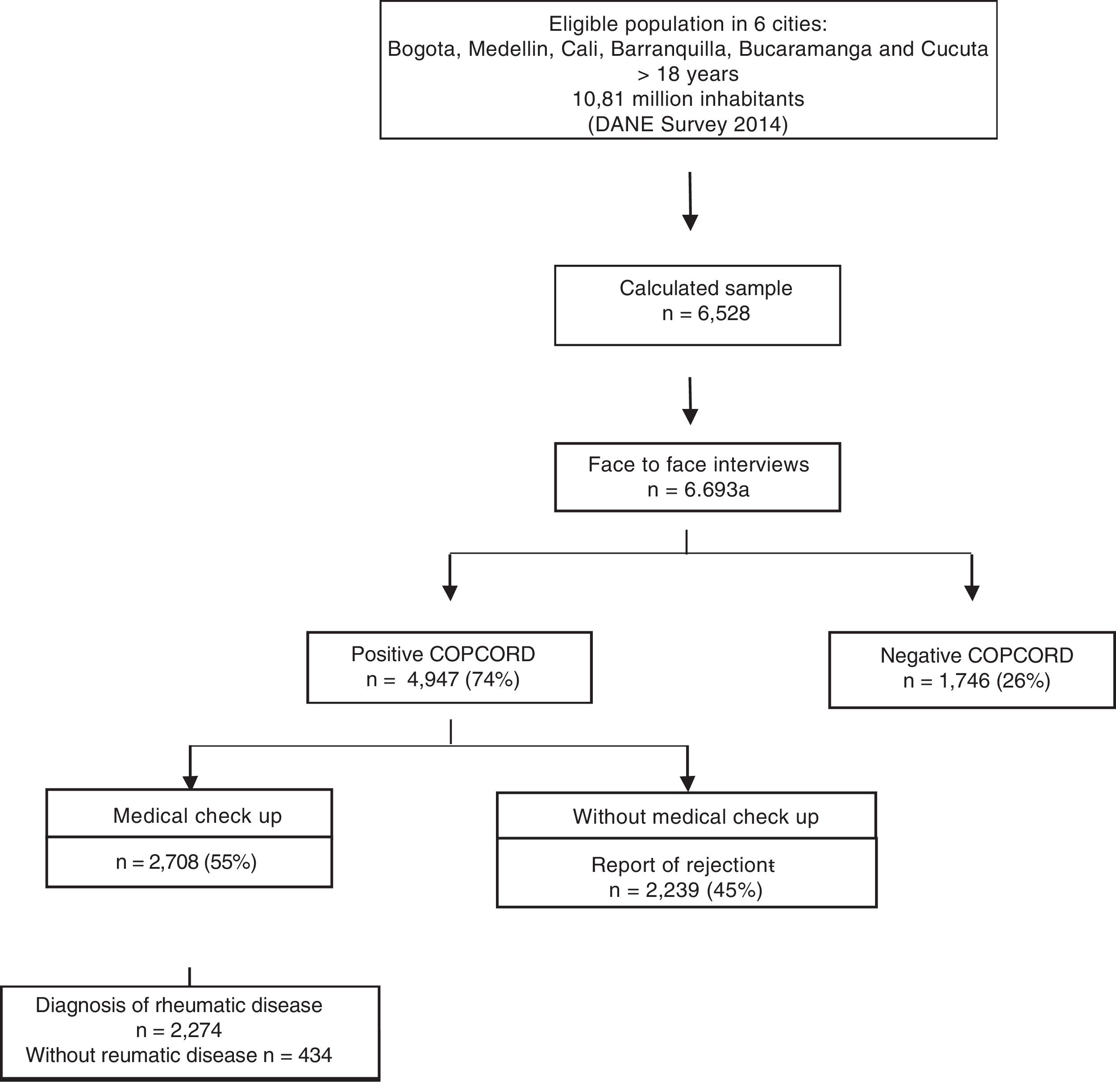
SampleIt was used a randomized sampling method of several stages: primary unit: city; secondary unit: city blocks within each city; tertiary unit: households. The candidate households were selected through the database of houses, homes and people (VIHOPE, for its acronym in Spanish) of the National Administrative Department of Statistics (DANE, for its acronym in Spanish), taking as the reference population the projections for the year 2014 conducted for residents in 6 cities that are representative of 80% of the population of the country (Bogota, Medellin, Cali, Barranquilla, Bucaramanga and Cucuta). It was estimated a total of 6528 respondents (Bogota 2336, Medellin 1220, Cali 1220, Barranquilla 746, Cucuta 503 and Bucaramanga 503), using an estimated prevalence for RA of 1.2%, with a confidence level of 95% (95% CI), a sample design effect of 1.5 and a sampling error of 14%.
RecruitingTrained interviewers applied questionnaires structured and validated for the Colombian population, face to face, in the homes of the participants. Different variables were collected: sociodemographic (age, gender, race, educational level, marital status), socioeconomic (family income, current professional status, health insurance, health care opportunity, medication coverage, percentage of the family income dedicated to health, among other econometric variables). The quality of life was measured using the EQ-5D-3L questionnaire, a generic and multidimensional instrument, which evaluates 5 dimensions (mobility, self-care, activities of daily living, pain/discomfort, and anxiety/depression), in 3 levels of response (1=without problems, 2=moderate problems, 3=extreme problems), and a scale to measure the health state in the present day (EQ-5D-VAS) (from 0=the best imaginable health state to 100=the worst imaginable health state)22,23; the physical function was measured using the Health Assessment Questionnaire (HAQ-DI), which is an instrument that contains 20 items organized into 8 categories which are qualified from 0 to 3.24 The latter 2 forms were previously validated for the Spanish language and the Colombian population. Information related with the antecedents of self-reported non-communicable chronic diseases (chronic high blood pressure, diabetes mellitus, cardiopathy, cancer, tuberculosis, mental disorders, obesity, venous insufficiency of the lower limbs, cerebrovascular disease, epilepsy and headache) was also collected.
The COPCORD questionnaire identifies individuals with rheumatic symptoms through an interview with trained surveyors. It includes questions related to the symptoms (pain and stiffness), disability, treatment and adaptation to the problem. This instrument includes a section on help-seeking behavior and a list of unconventional remedies.9 Individuals who manifested: pain, inflammation or stiffness during the past 7 days, at any time during their life and not associated with trauma, were classified as positive COPCORD. They were evaluated by a physician resident in Rheumatology of the programs of the Nueva Granada Military University or of the University of La Sabana, who completed a medical history and a physical examination using the Mexican strategy previously adapted and validated. Those subjects with possible rheumatic disease were assessed by a specialist in Rheumatology. The general performance of the previously validated screening procedure reported a sensitivity of 71% and a specificity of 35% for rheumatic disease. The definitive diagnosis was established based on the classification criteria of the American College of Rheumatology for OA, fibromyalgia (FM), RA, systemic lupus erythematosus (SLE), gout, Sjögren's syndrome, dermatomyositis, and systemic sclerosis; and based on the criteria proposed by the European Spondyloarthropathies Study Group (ESSG) for the spondyloarthritis (SpA).
For the classification of soft-tissue rheumatism, was used the definition of regional appendicular pain syndrome (RRPS), proposed by Álvarez-Nemegyei, which groups the tendinopathies, bursopathies, entrapment neuropathies and enthesopathies non-associated with systemic disease.25,26 For the manifestations of pain, inflammation or stiffness of some osteomusculoarticular structure that are non-classifiable within the previous categories, it was used the denomination non-specific musculoskeletal discomfort and non-rheumatic diseases were classified according with the CIE-10 registry.
A specific questionnaire for OA, FM, RA, gout, SpA and SLE was conducted (Fig. 1).
, Cali 628 (28%), Medellin 457 (20%), Cucuta 131 (6%), Barranquilla 125 (6%), Bucaramanga 92 (4%).")
General scheme of the study. DANE: National Administrative Department of Statistics.
aAdditional surveys n=165.
bNot interested: 614; Did not attend the evaluation after 7 contacts: 1123; Wrong contact information provided: 497; Deaths: 1; Dangerous area: 4. Discrimination by city: Bogota 806 (36%), Cali 628 (28%), Medellin 457 (20%), Cucuta 131 (6%), Barranquilla 125 (6%), Bucaramanga 92 (4%).
During the fieldwork of the study there was an epidemic of chikungunya fever which compromised 80% of the territory of the country and 5 of the 6 cities selected for the survey. An instrument for data collection of the patients suspected of chikungunya fever was designed according to the criteria of the World Health Organization. Serologic determination of IgG and IgM was performed for the confirmation of the cases with rheumatic commitment secondary to the infection. The specific data of this measurement will be reported in another publication.
Statistical analysisNo data was imputed or estimated in the construction of the database. The determinations of the prevalence for rheumatic diseases were calculated as weighted proportions using the expansion factors corresponding to each city. Participants with and without rheumatic disease were compared. The analyses of the variables were performed considering the study design. Tables with distribution of frequencies and percentages or measures of central tendencies and dispersion were used for the presentation of the data, depending of the characteristics of the variables. Parametric or non-parametric tests were used for the comparisons, according with the distribution and characteristics of the data.
To adjust the differences between groups, the following confounding factors were included: age, sex, educational level, working situation, family income and the number of comorbidities, to evaluate the independent relationship of each rheumatic disease with disability (HAQ) and quality of life (EQ-5D). It was established a value of statistical significance of 0.05% and 95% CI. It was used the Statistical Package for Social Sciences, SPSS Inc.
Ethical issuesThe research project was approved by the Research Subcommission and the Ethics Committee of the Faculty of Medicine of the University of La Sabana; all patients included in the study signed an informed consent. All participants gave their informed consent to participate in all phases of the study. The confidentiality of the information was maintained following the principles of the Helsinki declaration.
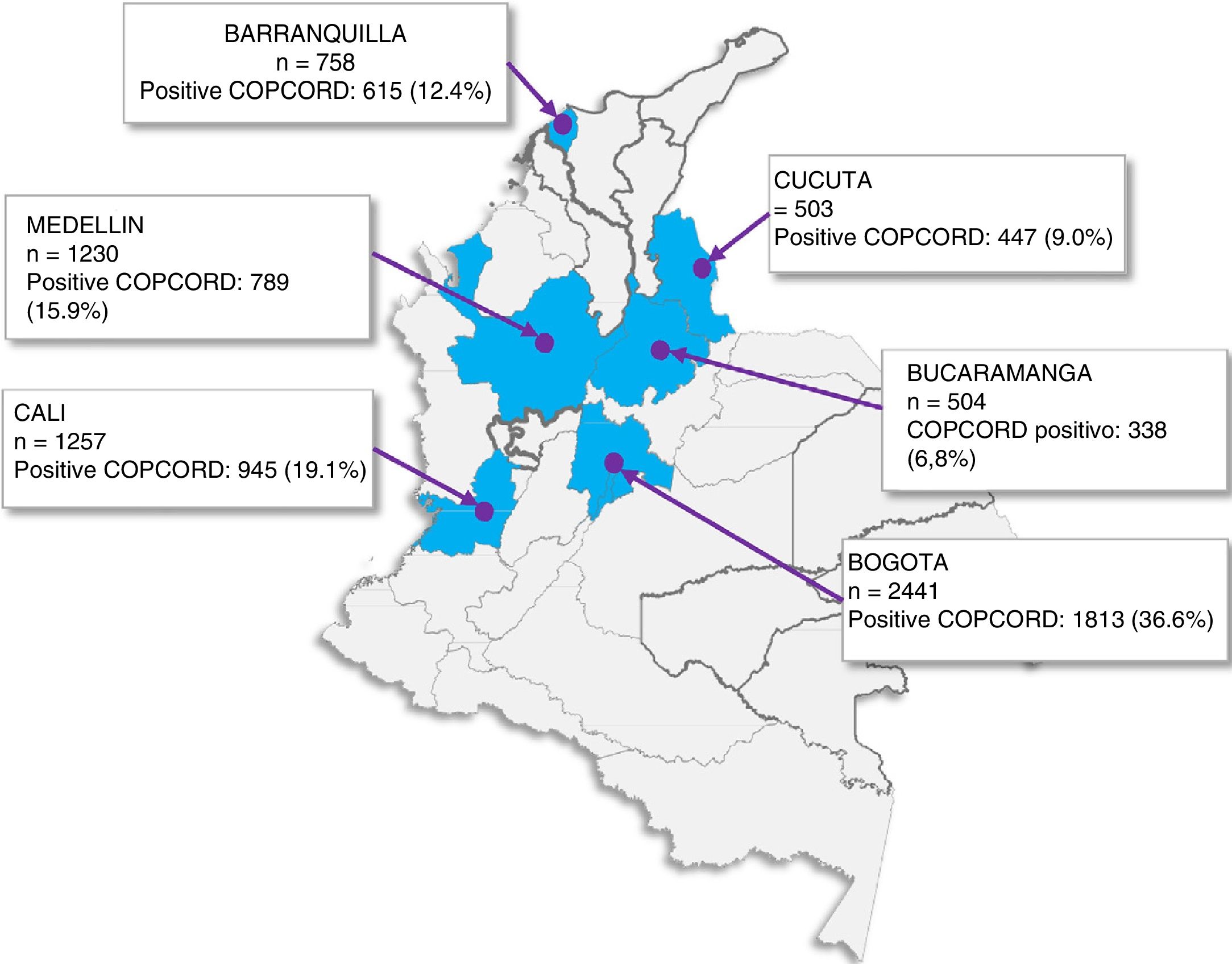
Results6693 individuals from 6 cities of Colombia were evaluated. The average age was 46.40±18.35 years and 4283 (64%) were women. In Fig. 2 is shown the population of each city with positive response to the COPCORD form.

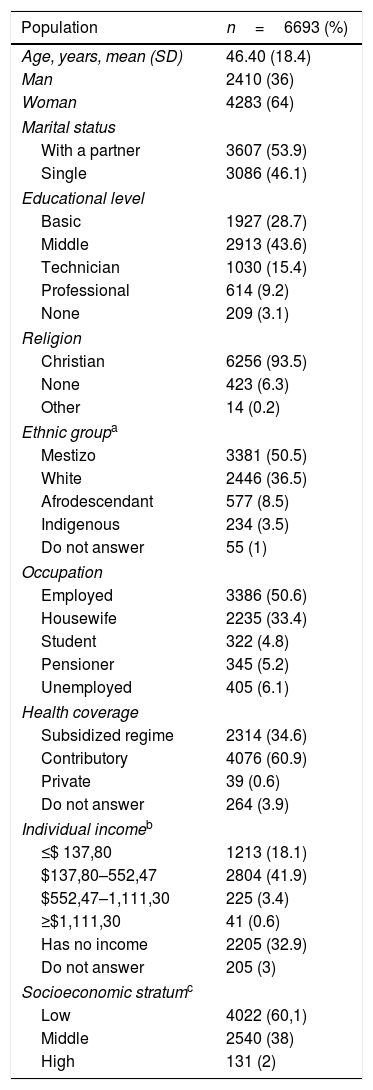
The majority of patients belonged to the low socioeconomic stratum with middle educational level and 50.5% of people were occupationally active. The sociodemographic characteristics of the population are shown in Table 1.
General characteristics of the population.
| Population | n=6693 (%) |
|---|---|
| Age, years, mean (SD) | 46.40 (18.4) |
| Man | 2410 (36) |
| Woman | 4283 (64) |
| Marital status | |
| With a partner | 3607 (53.9) |
| Single | 3086 (46.1) |
| Educational level | |
| Basic | 1927 (28.7) |
| Middle | 2913 (43.6) |
| Technician | 1030 (15.4) |
| Professional | 614 (9.2) |
| None | 209 (3.1) |
| Religion | |
| Christian | 6256 (93.5) |
| None | 423 (6.3) |
| Other | 14 (0.2) |
| Ethnic groupa | |
| Mestizo | 3381 (50.5) |
| White | 2446 (36.5) |
| Afrodescendant | 577 (8.5) |
| Indigenous | 234 (3.5) |
| Do not answer | 55 (1) |
| Occupation | |
| Employed | 3386 (50.6) |
| Housewife | 2235 (33.4) |
| Student | 322 (4.8) |
| Pensioner | 345 (5.2) |
| Unemployed | 405 (6.1) |
| Health coverage | |
| Subsidized regime | 2314 (34.6) |
| Contributory | 4076 (60.9) |
| Private | 39 (0.6) |
| Do not answer | 264 (3.9) |
| Individual incomeb | |
| ≤$ 137,80 | 1213 (18.1) |
| $137,80–552,47 | 2804 (41.9) |
| $552,47–1,111,30 | 225 (3.4) |
| ≥$1,111,30 | 41 (0.6) |
| Has no income | 2205 (32.9) |
| Do not answer | 205 (3) |
| Socioeconomic stratumc | |
| Low | 4022 (60,1) |
| Middle | 2540 (38) |
| High | 131 (2) |
SD: standard deviation.
Musculoskeletal discomfort given by pain, inflammation or stiffness was reported by 4947 (74%) individuals. Its manifestation in the past 7 days was present in 3493 (48%), with a pain intensity of 6.67 (SD: 2.79) according to the visual analogue pain scale (from 0 to 10cm). Of the respondents, 4947 (73%) referred osteomuscular symptoms at some time in their life, with an average of 6.81 (SD: 3.99) (visual analogue pain scale of 0–10cm).
The main location of pain was in the knees for both forms of presentation of the musculoskeletal discomfort; in the past 7 days it was of 31% and at some time in life of 35%. It was followed by the hands (25 vs. 26%) and the lumbar spine (18 vs. 20%), respectively.
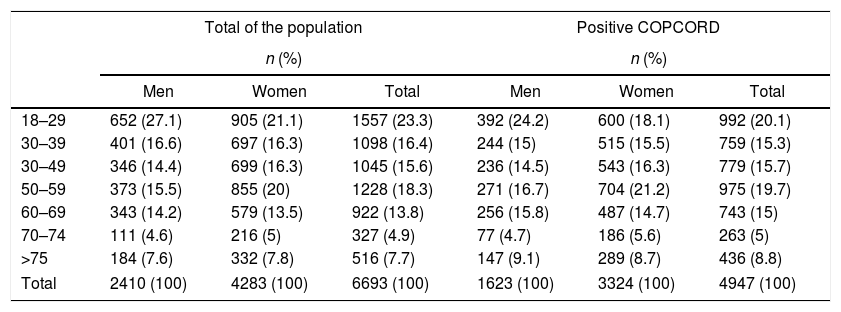
Table 2 shows the distribution by ages of the general population and the positive COPCORD population. The age range in which osteomusculoarticular symptoms were most frequent in women was between 50 and 70 years (35.9%), while in men the symptoms were most frequent between 18 and 29 years (24.2%).
Distribution of the population by age group.
| Total of the population | Positive COPCORD | |||||
|---|---|---|---|---|---|---|
| n (%) | n (%) | |||||
| Men | Women | Total | Men | Women | Total | |
| 18–29 | 652 (27.1) | 905 (21.1) | 1557 (23.3) | 392 (24.2) | 600 (18.1) | 992 (20.1) |
| 30–39 | 401 (16.6) | 697 (16.3) | 1098 (16.4) | 244 (15) | 515 (15.5) | 759 (15.3) |
| 30–49 | 346 (14.4) | 699 (16.3) | 1045 (15.6) | 236 (14.5) | 543 (16.3) | 779 (15.7) |
| 50–59 | 373 (15.5) | 855 (20) | 1228 (18.3) | 271 (16.7) | 704 (21.2) | 975 (19.7) |
| 60–69 | 343 (14.2) | 579 (13.5) | 922 (13.8) | 256 (15.8) | 487 (14.7) | 743 (15) |
| 70–74 | 111 (4.6) | 216 (5) | 327 (4.9) | 77 (4.7) | 186 (5.6) | 263 (5) |
| >75 | 184 (7.6) | 332 (7.8) | 516 (7.7) | 147 (9.1) | 289 (8.7) | 436 (8.8) |
| Total | 2410 (100) | 4283 (100) | 6693 (100) | 1623 (100) | 3324 (100) | 4947 (100) |
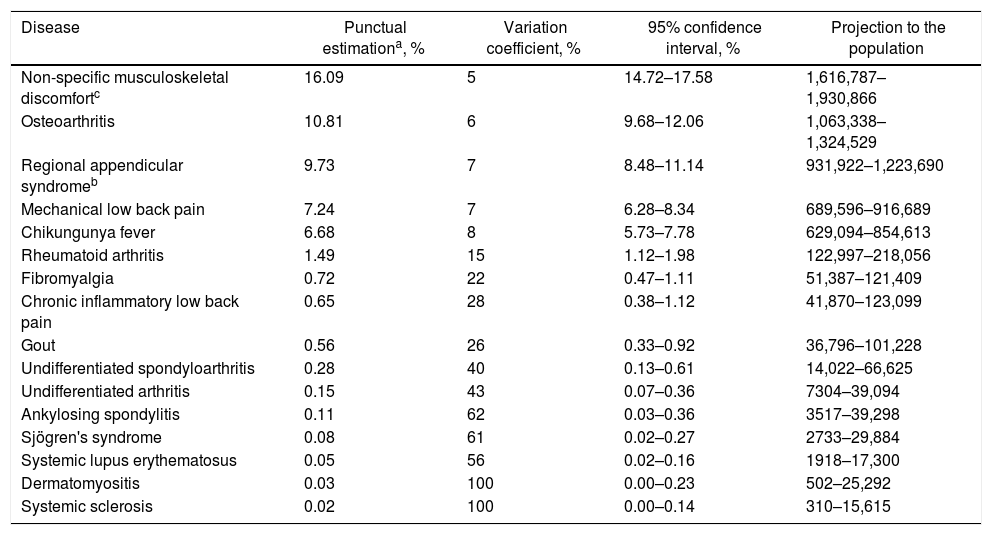
The prevalence of rheumatic diseases in Colombia is shown in Table 3. The majority of osteomusculoarticular symptoms manifested by the population correspond to non-specific muscle discomforts with a prevalence of 16.09% (95% CI: 14.72–17.58%).
Prevalence of rheumatic diseases in 6 cities of Colombia.
| Disease | Punctual estimationa, % | Variation coefficient, % | 95% confidence interval, % | Projection to the population |
|---|---|---|---|---|
| Non-specific musculoskeletal discomfortc | 16.09 | 5 | 14.72–17.58 | 1,616,787–1,930,866 |
| Osteoarthritis | 10.81 | 6 | 9.68–12.06 | 1,063,338–1,324,529 |
| Regional appendicular syndromeb | 9.73 | 7 | 8.48–11.14 | 931,922–1,223,690 |
| Mechanical low back pain | 7.24 | 7 | 6.28–8.34 | 689,596–916,689 |
| Chikungunya fever | 6.68 | 8 | 5.73–7.78 | 629,094–854,613 |
| Rheumatoid arthritis | 1.49 | 15 | 1.12–1.98 | 122,997–218,056 |
| Fibromyalgia | 0.72 | 22 | 0.47–1.11 | 51,387–121,409 |
| Chronic inflammatory low back pain | 0.65 | 28 | 0.38–1.12 | 41,870–123,099 |
| Gout | 0.56 | 26 | 0.33–0.92 | 36,796–101,228 |
| Undifferentiated spondyloarthritis | 0.28 | 40 | 0.13–0.61 | 14,022–66,625 |
| Undifferentiated arthritis | 0.15 | 43 | 0.07–0.36 | 7304–39,094 |
| Ankylosing spondylitis | 0.11 | 62 | 0.03–0.36 | 3517–39,298 |
| Sjögren's syndrome | 0.08 | 61 | 0.02–0.27 | 2733–29,884 |
| Systemic lupus erythematosus | 0.05 | 56 | 0.02–0.16 | 1918–17,300 |
| Dermatomyositis | 0.03 | 100 | 0.00–0.23 | 502–25,292 |
| Systemic sclerosis | 0.02 | 100 | 0.00–0.14 | 310–15,615 |
The most prevalent rheumatic disease in Colombia is OA (10.81%; 95% CI: 9.68–12.06%). RRPS is a group of entities frequent in the population (9.73%; 95% CI: 8.48–11.14%). Mechanical low back pain represented the third leading cause of rheumatic disease (7.24%; 95% CI: 6.28–8.34%), being slightly more prevalent in men than in women (8.58 vs. 8.19%).
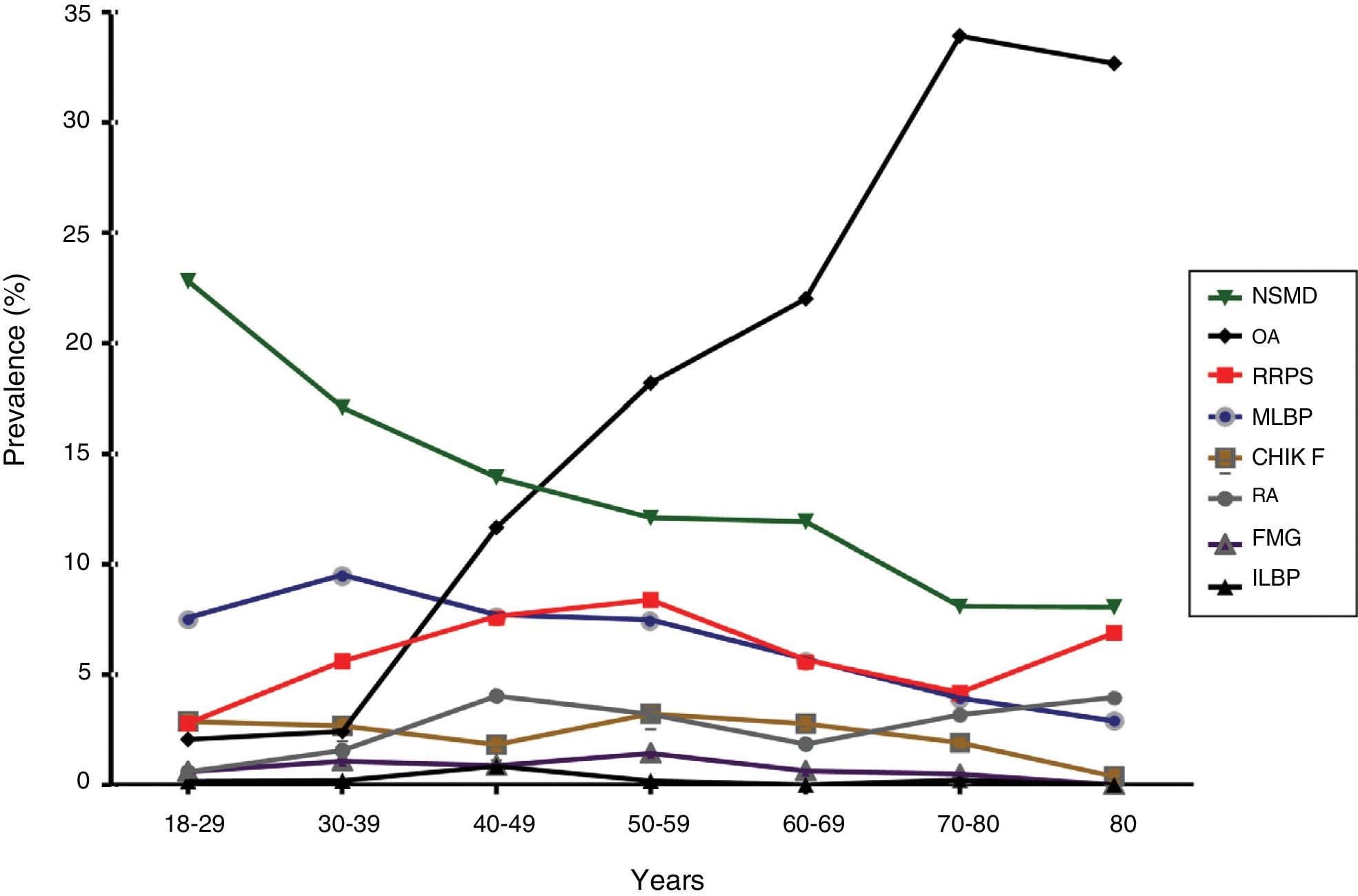
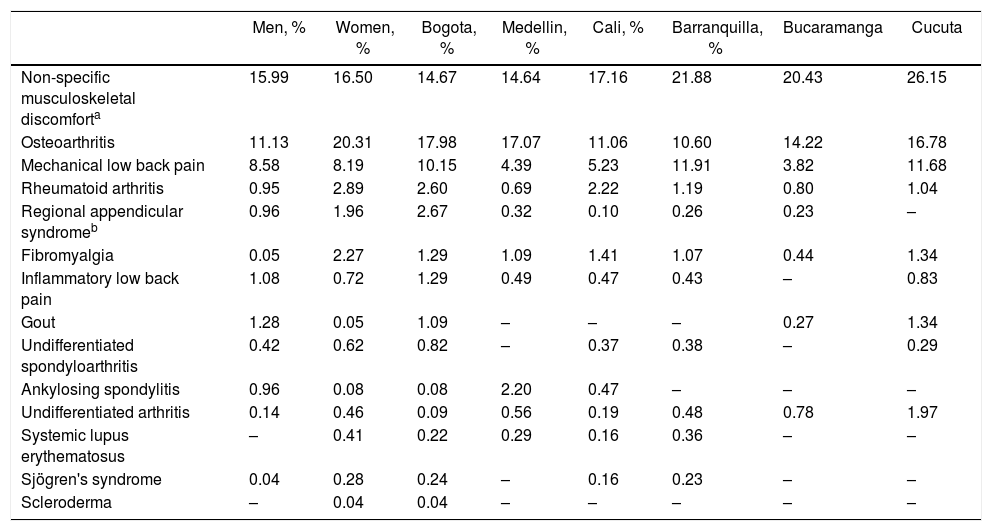
Of the inflammatory rheumatic diseases, RA was the most prevalent in the adult population (1.49%; 95% CI: 1.12–1.98%); followed by FM (0.72%; 95% CI: 0.47–1.11%). Gout, the SpAs, Sjögren's syndrome and SLE are less prevalent diseases. The distribution of the prevalence by cities is presented with detail in Table 4 and the distribution of the prevalence by age group of the most common diseases is shown in Fig. 3.
Prevalence of rheumatic diseases distributed by city.
| Men, % | Women, % | Bogota, % | Medellin, % | Cali, % | Barranquilla, % | Bucaramanga | Cucuta | |
|---|---|---|---|---|---|---|---|---|
| Non-specific musculoskeletal discomforta | 15.99 | 16.50 | 14.67 | 14.64 | 17.16 | 21.88 | 20.43 | 26.15 |
| Osteoarthritis | 11.13 | 20.31 | 17.98 | 17.07 | 11.06 | 10.60 | 14.22 | 16.78 |
| Mechanical low back pain | 8.58 | 8.19 | 10.15 | 4.39 | 5.23 | 11.91 | 3.82 | 11.68 |
| Rheumatoid arthritis | 0.95 | 2.89 | 2.60 | 0.69 | 2.22 | 1.19 | 0.80 | 1.04 |
| Regional appendicular syndromeb | 0.96 | 1.96 | 2.67 | 0.32 | 0.10 | 0.26 | 0.23 | – |
| Fibromyalgia | 0.05 | 2.27 | 1.29 | 1.09 | 1.41 | 1.07 | 0.44 | 1.34 |
| Inflammatory low back pain | 1.08 | 0.72 | 1.29 | 0.49 | 0.47 | 0.43 | – | 0.83 |
| Gout | 1.28 | 0.05 | 1.09 | – | – | – | 0.27 | 1.34 |
| Undifferentiated spondyloarthritis | 0.42 | 0.62 | 0.82 | – | 0.37 | 0.38 | – | 0.29 |
| Ankylosing spondylitis | 0.96 | 0.08 | 0.08 | 2.20 | 0.47 | – | – | – |
| Undifferentiated arthritis | 0.14 | 0.46 | 0.09 | 0.56 | 0.19 | 0.48 | 0.78 | 1.97 |
| Systemic lupus erythematosus | – | 0.41 | 0.22 | 0.29 | 0.16 | 0.36 | – | – |
| Sjögren's syndrome | 0.04 | 0.28 | 0.24 | – | 0.16 | 0.23 | – | – |
| Scleroderma | – | 0.04 | 0.04 | – | – | – | – | – |

Distribution of prevalence by age groups of the most common diseases.
NSMD: non-specific musculoskeletal discomfort; OA: osteoarthritis; RRPS: regional appendicular pain syndrome; MLBP: Mechanical low back pain; CHIK F: Chikungunya Fever; RA: rheumatoid arthritis; FMG: fibromyalgia; ILBP: inflammatory low back pain.
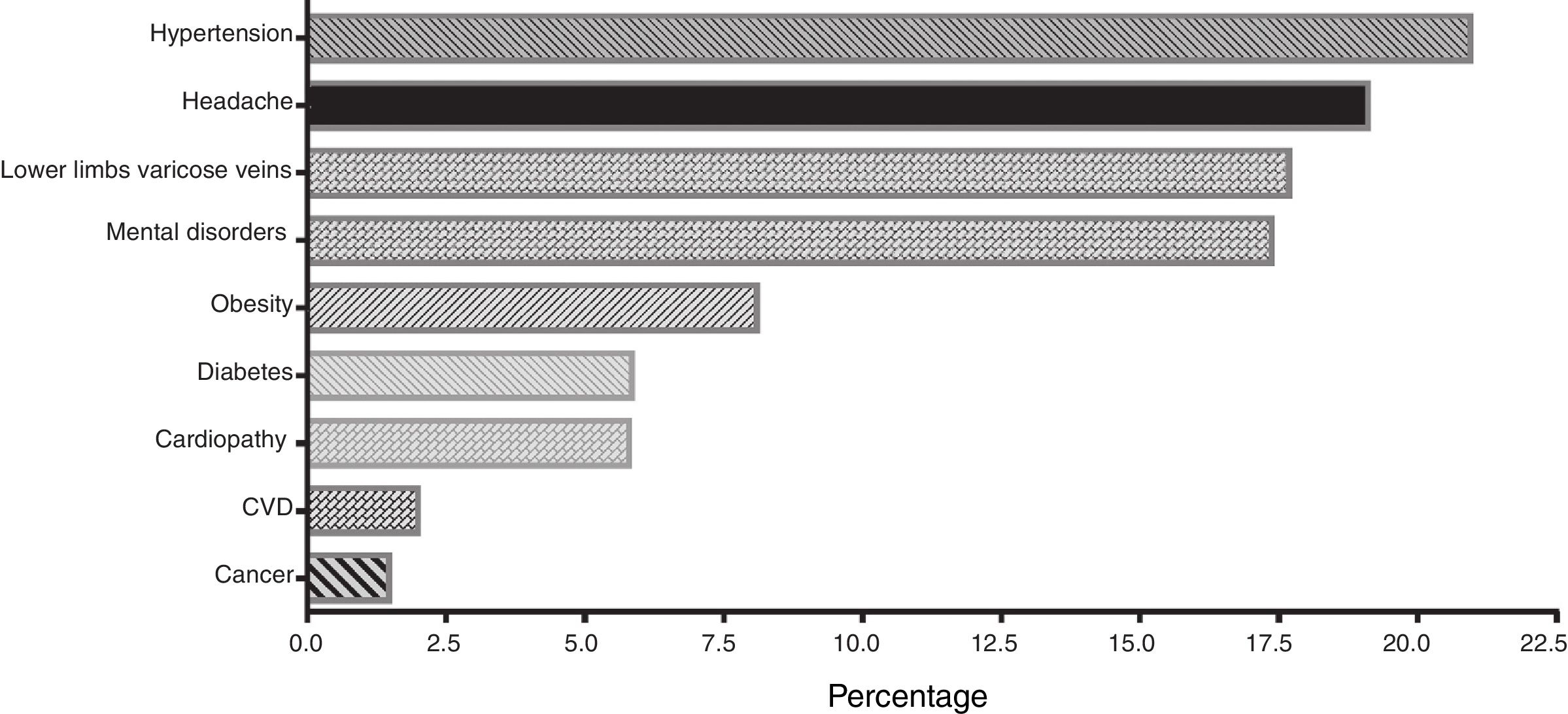
69% of the Colombian rheumatic patients reported having some comorbidity. The most frequent were chronic high blood pressure in 330 (20.95%), migraine in 300 (19.11%), venous insufficiency in 278 (17.69%) and mental disorders in 273 (17.3%) (Fig. 4).

When comparing the biomechanical load measured by a standardized instrument, significant differences were observed between the group of individuals with musculoskeletal pain and those who do no report it, and in the limitation of the participants to perform a work or daily living activities.
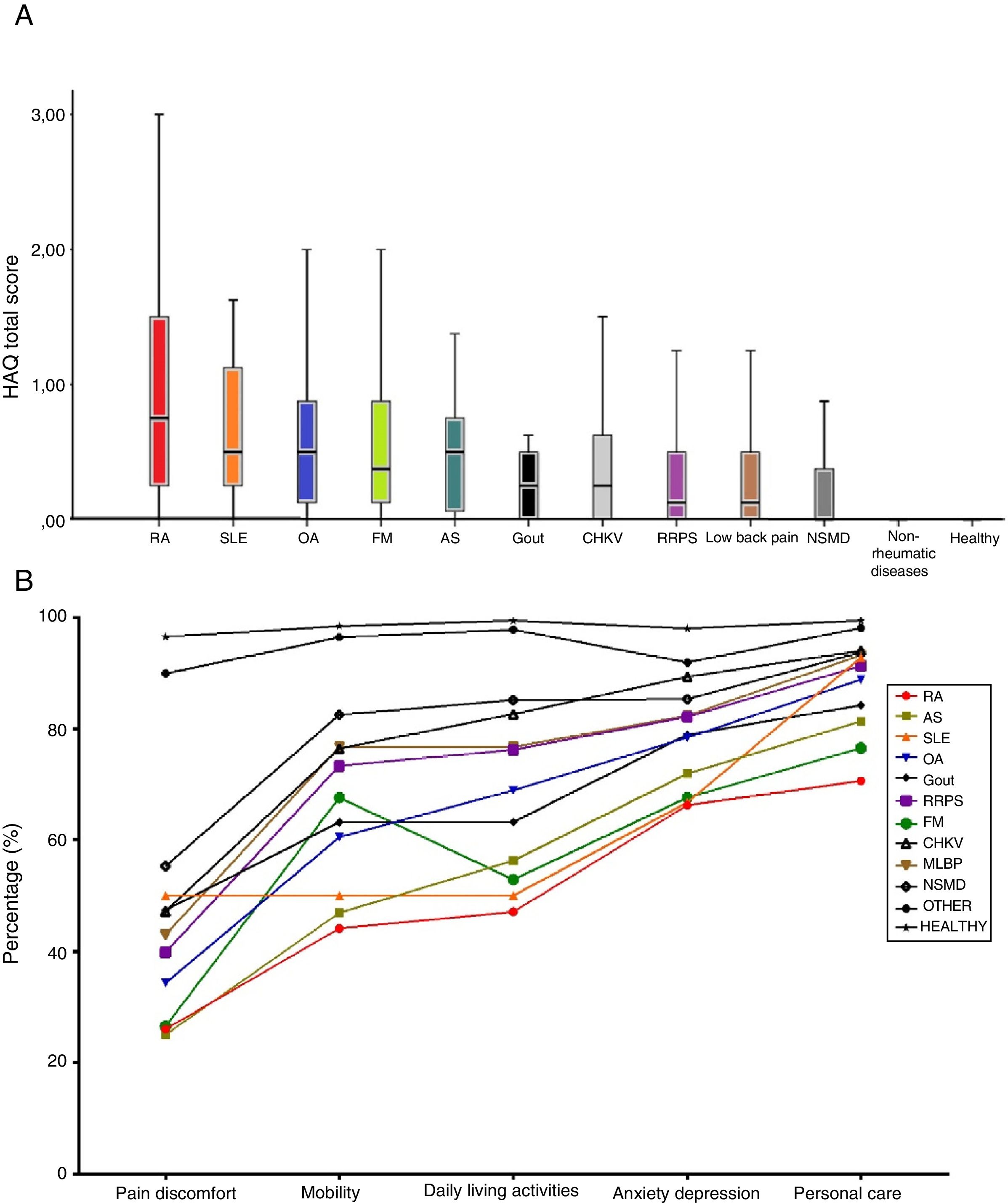
The patients with inflammatory rheumatic diseases (RA, SpA and SLE) had a greater alteration in the quality of life assessed by the EQ-5D-3L generic instrument. The patients with FM presented results very similar to those of RA in pain and discomfort, in the difficulty for the development of daily living activities and in the levels of anxiety and depression. In the same way, the patients with RA and SLE had the biggest functional limitation measured by HAQ-DI, followed by FM and OA (Fig. 5).

Quality of life and functional limitation assessed by EQ-5D-3L and HAQ-DI.
Panel A: Functional ability assessed by HAQ, the dots represent the mean of the instrument. Panel B: The lines represent the percentage of patients without pain of discomfort, anxiety or depression, or without mobility problems to perform daily living activities or personal care. RA: rheumatoid arthritis; CHIKV: chikungunya fever; FM: fibromyalgia; SLE: systemic lupus erythematosus; MLBP: mechanical low back pain; OA: osteoarthritis; OTHER: other non-rheumatic diseases; RRPS: regional appendicular pain syndrome; HEALTHY: healthy individuals; SpA: spondyloarthritis.
This is the first study conducted to estimate the prevalence of the most frequent rheumatic diseases in Colombia: OA, mechanical low back pain, RA, FM, systemic autoimmune diseases, gout, Sjögren's syndrome, SLE, dermatomyositis and systemic sclerosis. To the best of our knowledge there is no previous report in our population based on a direct assessment of the patients in a representative sample of 80% of the population of the country. Likewise, there does not seem to exist any information that is directly derived from a detailed evaluation of the prevalence of these diseases such as the data related to the burden of the disease and the economic impact on our setting.
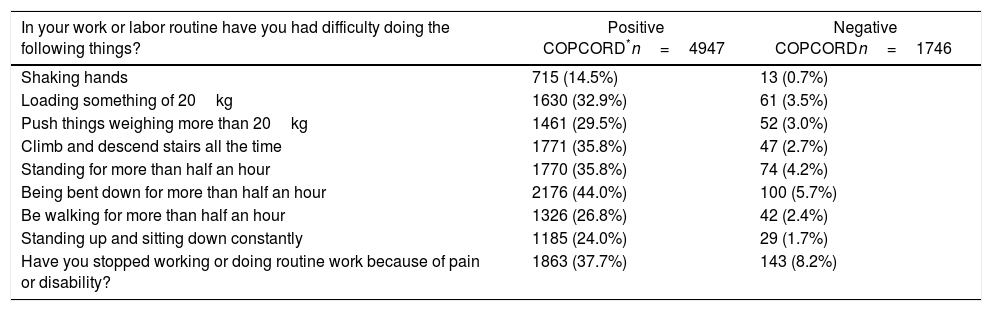
Another aspect that is worth highlighting in the realization and the results obtained in this research is related with the application of the instrument that measures the mechanical stress to which the joints and the soft tissues of the osteomuscular apparatus are subjected. Although there are reports in specific population groups, this appears to be the first study in open population with a broad sample, in which this information is recorded (Table 5).
Positive biomechanical load in positive and negative COPCORD populations.
| In your work or labor routine have you had difficulty doing the following things? | Positive COPCORD*n=4947 | Negative COPCORDn=1746 |
|---|---|---|
| Shaking hands | 715 (14.5%) | 13 (0.7%) |
| Loading something of 20kg | 1630 (32.9%) | 61 (3.5%) |
| Push things weighing more than 20kg | 1461 (29.5%) | 52 (3.0%) |
| Climb and descend stairs all the time | 1771 (35.8%) | 47 (2.7%) |
| Standing for more than half an hour | 1770 (35.8%) | 74 (4.2%) |
| Being bent down for more than half an hour | 2176 (44.0%) | 100 (5.7%) |
| Be walking for more than half an hour | 1326 (26.8%) | 42 (2.4%) |
| Standing up and sitting down constantly | 1185 (24.0%) | 29 (1.7%) |
| Have you stopped working or doing routine work because of pain or disability? | 1863 (37.7%) | 143 (8.2%) |
The prevalence of pain and musculoskeletal discomfort excluding trauma, in the past 7 days, in the present study, was 48%, a figure that significantly increased up to 73% when their presence at some time in life was considered. This percentage of population resulted high when compared with other results obtained in Latin American countries with similar cultural and sociodemographic conditions. In these countries, the prevalence of these symptoms varies from 11.86% reported in Guatemala12 to 53.7% in Argentina.10 This could be explained by the development of the epidemics of chikungunya fever between the years 2014 and 2015 in the country, which coincided with the fieldwork related to the direct population survey, and could have generated a global increase in the prevalence of rheumatic manifestations, especially in the category qualified as non-specific musculoskeletal discomfort, which involved 16.09% of the population, in comparison with the results obtained in Cuba (6.4%),13 Ecuador (7.0%)17 and Mexico (2.3%).25 This figure resulted similar to that reported in population of Portugal where the frequency was 15.8%.27 These results could be explained in part by the similarity in the distribution of the age groups in these 2 studies.
OA has a behavior similar to that reported in the majority of populations, with a value very similar to that reported in Mexican and North American populations.In neighboring countries such as Venezuela and Cuba it was between 15% and 20.4% of the population, respectively. The increase in the prevalence from 40 years (2.43%), until affecting one of every 3 individuals (33.9%) after 70 years of age is striking. This situation poses a challenge for all the agents involved in the solution of health problems, in the implementation of primary prevention programs where obesity plays an important etiologic role. All these problems of mechanical origin will continue to grow directly proportionally to the increase in survival and the secondary aging of the population.28
The low back pain (lumbago) of mechanic characteristics turned out to be a frequent manifestation in the young population, especially in men younger than 50 years of age. It calls the attention that, in Medellin and Bucaramanga, the prevalence was lower when compared with the other cities. It could be related to the type of work and the body mass index. As in OA our data were similar to those reported in the majority of Latin American countries except Cuba. In Portugal the prevalence was 26.4%. The figures of low back pain and OA in Cuba and Portugal had a similar behavior with figures significantly higher in comparison with the other countries.
The RRPS was more prevalent than what was reported in other studies such as in Mexico in 2011, where the global prevalence was 5% (95% CI: 4.7–5.4), with an important variation according with the studied region, being lower in the state of Yucatán 2.3% (95% CI: 1.8–2.8), and higher in Mexico City 6.9% (95% CI: 6.2–7.7). However, the term RRPS in other cohorts is superimposed to the concept of non-specific musculoskeletal discomfort. It is important to highlight the non-inflammatory etiology of the majority of components of this syndrome, for which a mechanic origin has been proposed, as a probable consequence of the use, overuse or misuse of the osteomuscular apparatus.
The foregoing could be related to the significant difference found between the patients who resulted positive in the screening of the COPCORD form and those who did not. The positive patients reported that they have been working in activities that involve frequent exposure to biomechanical stress, either static or dynamic, as described in Table 5. This relationship has been reported in the studies conducted in Mexican indigenous populations: Maya-Yucateca29 and Raramuri in the State of Chihuahua, in the north of the country.30
It is important to highlight the prevalence of RA found in our work, which was estimated in 1.49 (95% CI: 1.1–1.92), being similar to the reported in Mexico,25 higher to that of Venezuela15 and Brazil,31 and lower to that found in some Mexican indigenous groups of the Yucatan Peninsula (2.8%)26 and in Argentina (2.4%) in the Qom group (Toba) located in the Province of Rosario, in the Northwest of the country.10 The distribution of the prevalence of RA by cities was higher in Bogota, Cali and Barranquilla.
In Colombia, it has been reported a lower prevalence equivalent to 0.01% (95% CI: 0.008–0.02) in the African Colombian population of the municipality of Quibdó, located in the Pacific region in the West of the country.32 Due to logistic difficulties, this population is not represented in the sample of this study. The ethnic diversity and the miscegenation patterns in the regions involved in this study could explain in part this difference. In the city of Medellin (capital of Antioquia), the European ancestral pattern represents 96.7% of the population, situation that contrasts with the population of Cali (department of Valle del Cauca) where this pattern is of 21%.33
Another study recently reported a global prevalence of RA of 0.9%, which was obtained by an approximation based on the review of administrative reports from the National Department of Statistics.34 The data may be influenced by multiple factors that can turn into confounders or biases depending on the solidity of the sources from which the data are obtained.
The prevalence of FM in the Colombian population resulted similar to that previously reported in Mexico (0.7%), a figure comparative lower than the prevalence in Brazil, Portugal and Ecuador. However, it is necessary to recognize the impact of the disease on an individual level. In Colombia the patients with FM have been qualified as with the worst quality of life, below patients with inflammatory diseases such as RA, systemic autoimmune diseases, SLE and other conditions of generalized chronic pain. This deterioration has been related with the compromise of the functional ability due to pain, poor sleep pattern, less productivity, more comorbidities, greater chronic use of analgesics and increased costs.31 Thus, it has been proposed to consider FM as a complex dimensional disorder, beyond the simple representation of chronic pain, to consider the impact on the quality of life of these patients, especially in the aspects related with the physical function, the fatigue and the associated mental disorders such as depression and anxiety.32
Another information that this study provides is the impact of living in environments of high physical demand that lead to have chronic musculoskeletal pain; besides conditioning a limitation to work or perform the daily living activities.29 This is an important element for the design of population interventions for the management of working conditions with high physical demand that will reduce the disability secondary to living with chronic musculoskeletal pain and the socioeconomic impact that it conditions.
Limitations of the studyWhile the sample evaluated in this work represents a significant percentage of the Colombian urban population, it is not possible to make inferences of the result in the rural population which constitutes 20% of the current total population of the country, and the results cannot be interpreted as representative of specific American or African American native ethnic groups, which were not included in the randomization for the selection of the sample size. It is evident that these situations represent a limitation of this study.
Similarly, the difficulty, in some of the cities selected for the development of the study, because a significant percentage of the individuals who were selected to be evaluated by the physician given the possibility of suffering a rheumatic disease, finally were not assessed, constitutes a limitation of the study and could result in a underestimation in the final prevalence of the diverse rheumatic diseases studied. However, the methodological soundness of the study and a large and sufficient sample size makes that this situation has little impact on the final results obtained. As we have mentioned previously, this situation is directly related to the feeling of insecurity that the citizen perceives in some cities of the country.
This study was characterized by a varied participation in the medical evaluation of the population with osteomusculoarticular symptoms depending on the city evaluated, ranging between 38% corresponding to Cali and 96% in Bucaramanga. In Bogota 74% and in Medellin 55% of symptomatic patients completed the medical evaluations with the establishment of a definitive diagnosis when it was pertinent. The foregoing is related with the violence levels and the perception of insecurity of the inhabitants of the capital, Cali and Medellin.
Women accounted for 64% of the total of surveyed individuals. A possible explanation would be related to the transportation and mobility difficulties in the big cities that require long working days and restricted hours of presence of men at home, which facilitates the greater time availability of women at home. This situation could partially justify the higher frequency of RA in women in Colombia with respect to other Latin American countries.
The purpose of the present study and of the institutions that supported its development is to have own data of the Colombian population that allow to establish the true dimension of the public health problem that rheumatic diseases represent. Their impact on the functional ability, the deterioration of the quality of life of the individuals suffering from these conditions, as well as the significant increase in the costs generated by their attention, condition the establishment of health policies that allow a global reduction of the impact of these diseases on the society and the productive system of the country. Starting from these data, we intend to give continuity to this line of research on socioeconomic issues, by conducting a study on the burden of the rheumatic disease in Colombia.
One of the greatest challenges of the health system in Colombia is to have criteria and inputs for a true risk management; for this we must have, among other aspects, reliable information about the disease, its social determinants, its epidemiological aspects and the scientific evidence that allows to project comprehensive care where payers, providers, prescribers and society, have clear rules to make the health system sustainable and provide solutions to the medical problems of the population. This study becomes a transcendental information source so that the different agents of the health system can make effective and informed decisions around diseases that result in functional limitation and alteration of the quality of life of many Colombians, not counting the detriment in social productivity and the great expense in health that they bring about.
ConclusionThe rheumatic diseases in Colombia, like in the majority of countries of the Western hemisphere, represent frequent ailments. In the country, one of every 4 adults suffers from any of these pathologies. The problems derived from the use, overuse, misuse or overload due to overweight of the musculo-articular apparatus, justifies the majority of the ailments in the population younger than 50 years of age, being more prevalent in occupationally active men. The diseases caused by wear of the structures of the locomotor system are the most frequent in adults over 50 years of age. OA is the most important disease, with an exponential growth that causes that at the age of 80 years it affects one of every 3 individuals. Autoimmune diseases, especially RA, were more prevalent in Colombia than in the majority of Latin American countries, with the implication that this represents at the individual level secondary to the impact on the functional ability and the quality of life, and at the collective level, on the health expenditure derived from their treatment.
FundingThis study had the unrestricted economic support of the Colombian Association of Rheumatology and the University of la Sabana which guaranteed the full realization of the project.
Conflict of interestThe authors declare that they do not have any conflict of interest.
In its realization, specialized institutions were committed in each of its fields: the Colombian Association of Rheumatology, which economically supported the development of the project; the University of La Sabana, that gave the methodological and academic support, and the National Consulting Center, which conducted the fieldwork in 6 different cities of the country. We thank the GEEMA group (Group of Epidemiological Study of Musculo-Articular Diseases: Peláez-Ballestas I, Rodríguez-Amado J, Álvarez-Nemegyei J, Burgos-Vargas R, Garza M, Sanín LH, Goycochea MV, Cardiel MH) associated to the Mexican College of Rheumatology, for the methodological support in the development of this project.
We thank the EuroQol Research Foundation for the establishment of an academic collaboration agreement with the University of La Sabana which allowed the use of the EQ-5D-3L instrument, to determine the quality of life of the individuals who took part in this research.
Please cite this article as: Londoño J, Ballestas IP, Cuervo F, Angarita I, Giraldo R, Rueda JC, et al. Prevalencia de la enfermedad reumática en Colombia, según estrategia COPCORD-Asociación Colombiana de Reumatología. Estudio de prevalencia de enfermedad reumática en población colombiana mayor de 18 años. Rev Colomb Reumatol. 2018;25:245–256.
