


Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by the presence of autoantibodies and multisystemic disease. Viruses are widely associated with autoimmunity, and are also implicated in the pathogenesis of systemic lupus erythematosus. Two cases are described that have an autoimmune response related to dengue infection. The clinical presentation of systemic lupus erythematosus is very diverse, and in these cases it was important to consider SLE as a diagnosis.
El lupus eritematoso sistémico (LES) es una enfermedad autoinmune, caracterizada por la presencia de autoanticuerpos y afección multisistémica. Los virus se encuentran ampliamente asociados a autoinmunidad y también se han encontrado implicados en la patogénesis del LES. A continuación se presentan 2 casos con respuesta autoinmune relacionada con infección por el virus del dengue. La presentación clínica del LES es muy diversa, en estos casos fue importante tener la sospecha diagnóstica.
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by the presence of autoantibodies and multisystemic involvement.1 It should be considered as a differential diagnosis in all patients with multisystemic compromise.
Our country is currently considered endemic for dengue, with hyperimmune response.3 We present two pediatric cases with autoimmune response related to dengue virus (DV) infection.
Case 1A 6-year-old female patient, who a week prior to her admission starts having fever, arthralgias and generalized dermal lesions. Mucocutaneous ulcers, generalized erythematous maculopapular lesions, interphalangeal arthritis in the right elbow, both hands, knees and ankles were observed on physical examination, in addition to hepatomegaly. It was requested a dengue serology test, which showed positivity, and for this reason it was made a diagnosis of severe dengue. During her stay she presented pericardial effusion, anemia, thrombocytopenia, leukopenia, transaminasemia, high CRP, high LDH, proteinuria and hematuria, and therefore was assessed by the service of pediatric rheumatology, which requested antibodies, presenting antinuclear antibodies with an homogeneous pattern 1280 3+ and a cytoplasmic pattern 1280 1+, anti-native DNA antibodies 1:10 4+, antinucleosome antibodies of 52.0U/ml, and hypocomplementemia; based on the ACR criteria, it was made a diagnosis of SLE (Table 1) in addition to infection with DV. It was started management with chloroquine, azathioprine, prednisone, and naproxen sodium.
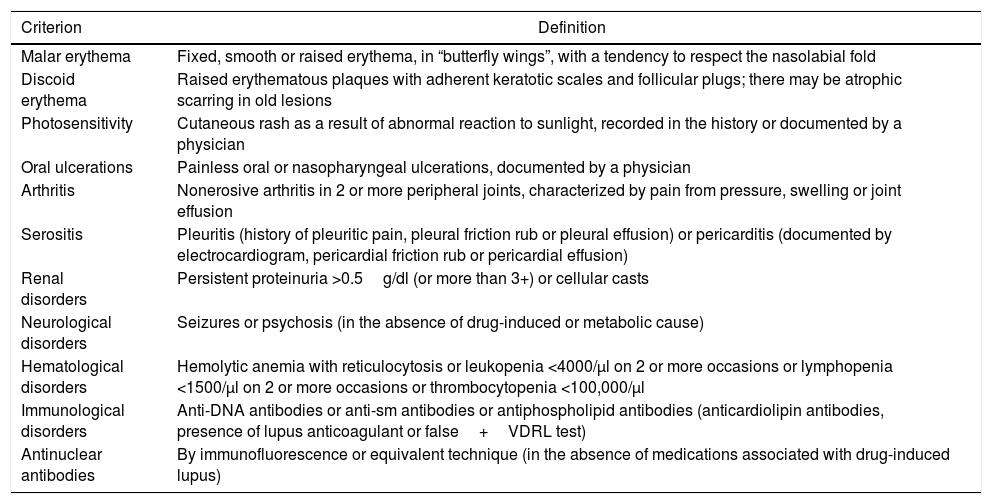
Criteria of the American College of Rheumatology reviewed in 1997 for the classification of systemic lupus erythematosus.
| Criterion | Definition |
|---|---|
| Malar erythema | Fixed, smooth or raised erythema, in “butterfly wings”, with a tendency to respect the nasolabial fold |
| Discoid erythema | Raised erythematous plaques with adherent keratotic scales and follicular plugs; there may be atrophic scarring in old lesions |
| Photosensitivity | Cutaneous rash as a result of abnormal reaction to sunlight, recorded in the history or documented by a physician |
| Oral ulcerations | Painless oral or nasopharyngeal ulcerations, documented by a physician |
| Arthritis | Nonerosive arthritis in 2 or more peripheral joints, characterized by pain from pressure, swelling or joint effusion |
| Serositis | Pleuritis (history of pleuritic pain, pleural friction rub or pleural effusion) or pericarditis (documented by electrocardiogram, pericardial friction rub or pericardial effusion) |
| Renal disorders | Persistent proteinuria >0.5g/dl (or more than 3+) or cellular casts |
| Neurological disorders | Seizures or psychosis (in the absence of drug-induced or metabolic cause) |
| Hematological disorders | Hemolytic anemia with reticulocytosis or leukopenia <4000/μl on 2 or more occasions or lymphopenia <1500/μl on 2 or more occasions or thrombocytopenia <100,000/μl |
| Immunological disorders | Anti-DNA antibodies or anti-sm antibodies or antiphospholipid antibodies (anticardiolipin antibodies, presence of lupus anticoagulant or false+VDRL test) |
| Antinuclear antibodies | By immunofluorescence or equivalent technique (in the absence of medications associated with drug-induced lupus) |
VDRL: venereal disease research laboratory.
A 3-year-old female patient, hospitalized for presenting fever accompanied by convulsive crisis, in addition of thrombocytopenia, facial edema and proteinuria. It was carried out a diagnostic approach for infection with DV,4 which was confirmed due to a positive epidemiological study for dengue, in addition to nephrotic syndrome. One week after admission the patient entered the intensive care unit due to decompensation of the crisis, as well as cardiovascular deterioration. The patient was managed with furosemide, hydralazine, prednisone, calcium, levetiracetam and phenobarbital. Two months after, she reenters presenting bilateral periorbital and facial edema, alopecia, malar erythema, anemia, thrombocytopenia, proteinuria and hematuria. The patient was assessed by the service of pediatric rheumatology and antibodies testing were requested, presenting antinuclear antibodies with a fine speckled pattern of 1:1280, anti-double stranded DNA antibodies of 31IU/ml and antinucleosome antibodies of 258IU/ml. A diagnosis of SLE was made based on the ACR criteria. At discharge was managed with intravenous gammaglobulin, hydroxychloroquine, mycophenolic acid, enalapril and vitamin D. One week later the patient died from pulmonary hemorrhage and consequent cardiorespiratory arrest (Table 2).
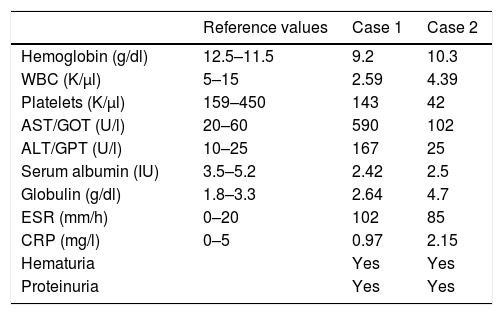
Descriptive analysis of the variables of the patients at their admission to the hospital.
| Reference values | Case 1 | Case 2 | |
|---|---|---|---|
| Hemoglobin (g/dl) | 12.5–11.5 | 9.2 | 10.3 |
| WBC (K/μl) | 5–15 | 2.59 | 4.39 |
| Platelets (K/μl) | 159–450 | 143 | 42 |
| AST/GOT (U/l) | 20–60 | 590 | 102 |
| ALT/GPT (U/l) | 10–25 | 167 | 25 |
| Serum albumin (IU) | 3.5–5.2 | 2.42 | 2.5 |
| Globulin (g/dl) | 1.8–3.3 | 2.64 | 4.7 |
| ESR (mm/h) | 0–20 | 102 | 85 |
| CRP (mg/l) | 0–5 | 0.97 | 2.15 |
| Hematuria | Yes | Yes | |
| Proteinuria | Yes | Yes |
ALT/GPT: alanine-aminotransferase; AST/GOT: aspartate-aminotransferase; LDH: lactic dehydrogenase; ESR: erythrocyte sedimentation rate; WBC: leukocytes.
Viral infections have been implicated in autoimmunity and SLE. Several hypotheses on the pathogenesis of the DV have been proposed. Viruses can induce autoimmunity through several mechanisms, including molecular mimicry, activation of T cells by superantigens and dissemination of T cells previously activated in a site of inflammation, among others.5 A retrospective study conducted in 97 patients confirmed the association between the pathogenesis of dengue and the development of an autoimmune response.
We suspected that our patients presented clinically an autoimmune response developed due to the infection with the DV, which in both cases was diagnosed as SLE. It should be noted that a patient with SLE and fever is always a challenge since it may be due to a relapse or infection due to the immunosuppression that these patients have. The first case was timely diagnosed presenting an adequate response under treatment with glucocorticoids, immunosuppressants and antimalarial agents. The patient of the second case enters through the emergency service due to fever in addition to thrombocytopenia; at her discharge from the intensive care unit is assessed by the service of pediatric rheumatology, coming to the suspicion of SLE due to her clinical evolution, being confirmed this diagnosis with antibodies. It should be mentioned that the second case presented a poor response to treatment due to a late diagnosis, which caused her death.
It is proposed that after the infection with DV, the non-neutralizing reactive antibodies found in the circulation of infected individuals facilitate the viral entry of different serotypes of dengue virus through the FC receptor, which worsens the patient's condition. The FC receptors are glycoproteins that are found on the surface of several types of leukocytes, in which an alteration in their function, due to polymorphism, contributes to an inadequate antibody response, which leads to the development of an autoimmune disease.6
Rajadhyaksha et al. propose that the dengue viremia can be the trigger for the formation of immune complexes in patients who are predisposed to develop an autoimmune disease.7 In addition, it can be suspected that anti-dengue NS1 antibodies show cross-reactivity with endothelial cells and inhibit the active form of plasminogen by molecular mimicry.6,8
It could be hypothesized that after an infection by the DV, the antibodies cross-react, and due to an alteration in the FC receptor, there is an inadequate elimination of immune complexes, which leads to the synthesis of inflammatory cells.6
ConclusionThe clinical presentation of SLE is very diverse; in these cases it was important the diagnostic suspicion despite the positivity of the serological test for dengue. It is worth noting that it is not possible to determine the chronology between dengue and SLE because infection processes can trigger autoimmunity. It is important to continue with extension studies in order to be able to conclusively determine the relationship between the presence of antibodies against dengue, as well as anti-nuclear antibodies in SLE.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors declare they do not have any conflict of interest.
Please cite this article as: Luevanos-Velázquez A, Vega-Cornejo G, Monteón-Galván D. ¿Qué estamos buscando? Lupus eritematoso sistémico vs. infección por dengue: reporte de casos. Rev Colomb Reumatol. 2017;24:251–253.
