



A scintigraphic image is presented that shows the typical characteristics of psoriatic arthritis as a teaching aid.
Se presenta una imagen gammagráfica que muestra en forma didáctica características típicas de la artritis psoriásica.
Psoriatic arthritis (PsA) is a chronic inflammatory arthropathy associated with cutaneous psoriasis. It is considered part of the group of spondyloarthritis. Psoriasis occurs in approximately 2% of the general population, and up to 40% of these patients may suffer from PsA, with a broad clinical spectrum.1
Clinical summaryA 45-year-old woman with a clinical picture of asymmetric polyarthritis of 3 years of evolution reported a history of multiple unsuccessful diagnostic and therapeutic interventions. At her first consultation with rheumatology she arrived without a diagnosis, despite bringing many exams that included, among others, a bone scintigraphy (Fig. 1). The patient herself made emphasis on the peculiar asymmetry of her condition, because she had affected a wrist, a finger of the other hand, a shoulder of one side and the contralateral knee. Her illness began 3 years before with painful edema of the third and fourth toes of the right foot. She had suffered from psoriasis since she was 15 years old. During the physical examination we found a small psoriatic plaque in the occipital region, evident arthritis in the right wrist and in the metacarpophalangeal, proximal and distal interphalangeal joints of the fifth finger of the left hand, as well as pain in the right shoulder and enthesitis in the knees. Methotrexate-based treatment was initiated with complete improvement of her cutaneous and articular symptoms.
.")
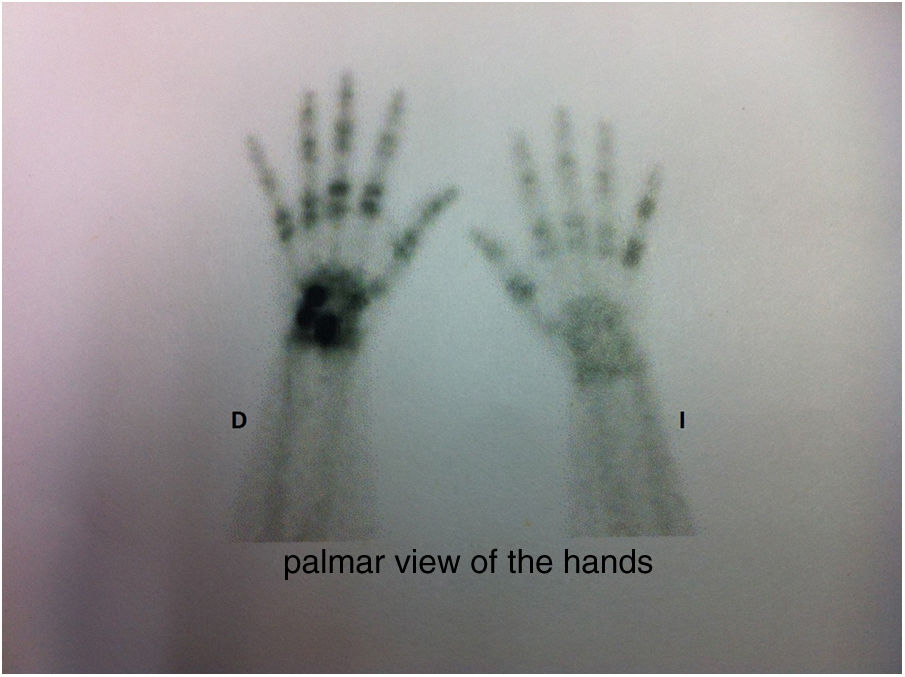
Bone scintigraphy of the hands with characteristic findings of psoriatic arthropathy2: asymmetric involvement, affection of distal interphalangeal joints and ray distribution (fifth finger of the left hand and third and fourth fingers of the right hand.).
PsA can be a diagnostic challenge if a systematic approach is not made at the time of carrying out the anamnesis and documenting the findings on the physical examination. This arthropathy has several patterns of clinical presentation that include the involvement of the distal interphalangeal joints with concomitant nail involvement, asymmetric oligoarthritis, and polyarthritis that can be asymmetric in 50% of patients,3,4 in addition, there may be axial compromise with sacroiliitis, usually bilateral asymmetric. Another equally characteristic articular presentation is the ray distribution pattern, i.e., the involvement of the distal and proximal interphalangeal joints, as well as of the metacarpophalangeal joint of the same finger.5
Radiologically, PsA is characterized by erosions and loss of joint space with preservation of bone mineralization; it is also common to observe bone neoformation, periostitis and ankylosis. The erosions can configure a typical pattern known as “pencil-in-cup” and there may also be acro-osteolysis or resorption of the distal phalanges (arthritis mutilans).
The main differential diagnoses are osteoarthritis of the hands due to the involvement of the distal interphalangeal joints, as well as the other diseases of the spondyloarthritis group, including reactive arthritis, due to the frequent association with dactylitis, enthesitis, cutaneous and ocular lesions.
ConclusionFor the approach of the joint disease, anamnesis and physical examination are of utmost importance, which can be complemented in selected cases with some imaging modalities such as simple X-rays, ultrasound and magnetic resonance. The bone scintigraphy requested previously was totally unnecessary, but it allowed us to observe and demonstrate in a didactic way a characteristic articular pattern of the PsA evident with a good clinical approach.
Conflict of interestThe authors declare that they do not have any conflict of interest.
Please cite this article as: Restrepo-Escobar M, Hernández-Zapata J. Poliartritis asimétrica con distribución en rayo. Rev Colomb Reumatol. 2019;26:214–215.
