




Fibromyalgia syndrome is characterized by chronic pain associated with non-specific somatic symptoms, and has a personal, social, occupational, and economic impact. The assessment is performed independently, by analyzing the clinical aspects, severity, therapies, and their effectiveness, as well as the impact on daily life activities and its effect on employment. The FM-Check tool is a subjective scale that can be helpful in jointly assessing all these aspects, and provide professional support in monitoring the patient, as well as contribute to a multidisciplinary approach.
MethodTo develop FM-Check is developed by starting with the clinical history in which the variables that are going to be used are defined, and grouped into 4 blocks to which a percentage limitation rate is assigned for each variable and each block. An overall percentage limitation is then calculated for the activities in each person.
ResultsThe distribution of assigned percentages was: a maximum of 10% for personal appearance, 55% for clinical-therapeutic aspects, 24% for work aspects, and 10% for impact on everyday life. The limitation levels were classified according to the overall percentage obtained after assessing the patient; grade 1: an overall percentage <20%, grade 2: 20–40%, grade 3: 41–70%, and grade 4: >70%.
ConclusionFM-Check aims to make it easier for the clinician to monitor the patient and making medical-therapeutic decisions after an overall assessment of the limitation of the fibromyalgia patient. This achieved by following a unified methodology that can compare individual developmental outcomes, as well as for conducting joint epidemiological studies.
El síndrome fibromiálgico se caracteriza por dolor crónico asociado a sintomatología somática no específica y con las limitaciones asociadas a su impacto personal, social, laboral y económico. Su valoración se realiza de forma independiente, analizando sus aspectos clínicos, de severidad, los tratamientos y su efectividad, la repercusión en las actividades de la vida diaria y la repercusión o afectación laboral. La herramienta FM-Check es una escala subjetiva que puede ser de ayuda para valorar de forma conjunta todos estos aspectos y servir de apoyo al profesional en el seguimiento del paciente y facilitar la colaboración conjunta interprofesional.
MétodoPara elaborar la FM-Check se parte de la historia clínica en la que se definen las variables que se van a utilizar agrupándolas en 4 bloques a los que se asignan porcentajes de limitación para cada variable y cada bloque, para llegar a un porcentaje global de limitación en los roles de las personas.
ResultadosLa distribución de porcentajes por cada bloque es en máximos: 10% para aspectos personales, 55% para clínico-terapéuticos, 24% para laborales y 10% para repercusión en la vida diaria. En función del porcentaje global obtenido tras la valoración del paciente se asignan grados de limitación: grado 1 hasta un porcentaje global <20%, grado 2 del 20-40%, grado 3 entre el 41-70% y grado 4 >70%.
ConclusiónFM-Check pretende facilitar la labor médica en la evolución del paciente y la toma de decisiones clínico-terapéuticas tras una valoración global de la limitación del paciente con fibromialgia, siguiendo una metodología unificada que permita comparar resultados evolutivos individuales y la realización de estudios epidemiológicos colectivos.
Fibromyalgia syndrome is a complex clinical picture characterized by chronic pain associated with non-specific somatic symptoms such as fatigue, sleep alterations, cognitive dysfunction or anxiety-depressive episodes. To the complexity of the pathophysiological mechanisms underlying this disease, which are necessary to understand the diagnosis itself,1 and the chronicity of the symptoms, should be added the economic impact entailed both on direct healthcare costs and on indirect costs,2 comparable or even higher to those of other chronic diseases better known or valued.3
Included in the medical literature of the last decades are numerous publications about the very existence or not of fibromyalgia as a disease,4 related to its impact on the quality of life and disability (especially among women as the most affected group and directly related to their occupation)5 or that address its economic cost and social impact, which are higher when the severity of the picture is greater.6
In order to be able to assess the limitations caused by a disease, even more so if its evolution is chronic, the clinical and therapeutic aspects, as well as the repercussion on daily live and labor, must be taken into account.
This tool constitutes the first step for the assessment of the limitations in fibromyalgia and the repercussions they suppose on the social and labor roles, intending to:
- •
Integrate into it patients who meet criteria for fibromyalgia.
- •
Establish a minimum of clinical and therapeutic variables necessary for the assessment.
- •
Estimate the repercussions on the activities of their daily life.
- •
Consider the repercussion on the work performance caused by the limitations secondary to the disease.
- •
Assess and quantify the set of all limitations to make easier the work of the physician regarding the follow-up of the evolution of the patient, the efficacy of the prescribed therapies and the impact in all facets of his life.
- •
Compare the patients as a whole by using an equal tool in all cases.
For the diagnosis of the patients and rating of the severity of the disease were used the questionnaires validated by consensus in fibromyalgia, according to the 2010 ACR criteria: WPI+SS-SCORE.7
For the assessment of the impact of fibromyalgia was used the CIF/FQI,8 in its version validated and approved by consensus for Spain.
For the evaluation of pain was used the visual analog scale.9
The Barthel questionnaire-index was used for the assessment of the impact on the activities of daily living.10
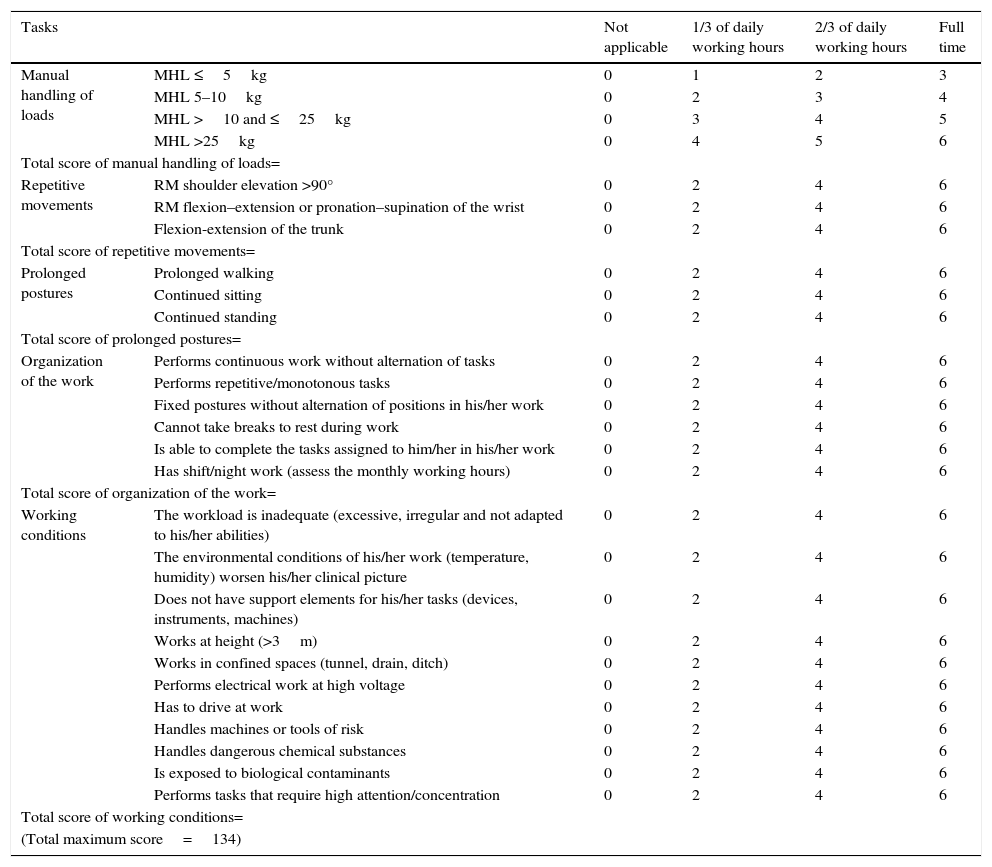
For the assessment of the limitations in the work performance, the authors designed a check-list based on the aspects of greater affectation due to the limitations in fibromyalgia and related to characteristics of the jobs, following the regulations in force in Spain (Law on Prevention of Occupational Risks)11 and the specific healthcare surveillance protocols.12
The valuation contained in the Spanish legislation on disability13 and the Spanish criteria for the evaluation of the disability of the National Institute of Social Security (INSS)14 have served as a basis for the weighting of the different sections.4
The results are grouped into 4 blocks, to which the authors assign a percentage weight of limitation for each variable and an overall percentage, estimating as a priority the clinical and therapeutic aspects as they considered them more objectifiable.
In block 1 are collected the personal aspects, in block 2 the clinical and therapeutic aspects, in block 3 the labor aspects, and in block 4 the aspects of repercussion in the activities of daily living.
With the final percentage obtained is established a degree of limitation that allows to make subsequent comparisons following the same procedure.
The tool has been tested by the authors through a pilot test in 14 patients, with results that show a correct correlation clinical and of the limitations adjusted to the assigned grade, pending a larger study with patients that would allow establishing a comparison with epidemiological validity and being object of subsequent publication as a validated tool.
ResultsThe percentage distribution assigned to the different blocks is shown in Tables 1–4. The degrees of limitation according to the percentages are shown in Table 5. The check-list used for the labor assessment is attached in Appendix A.
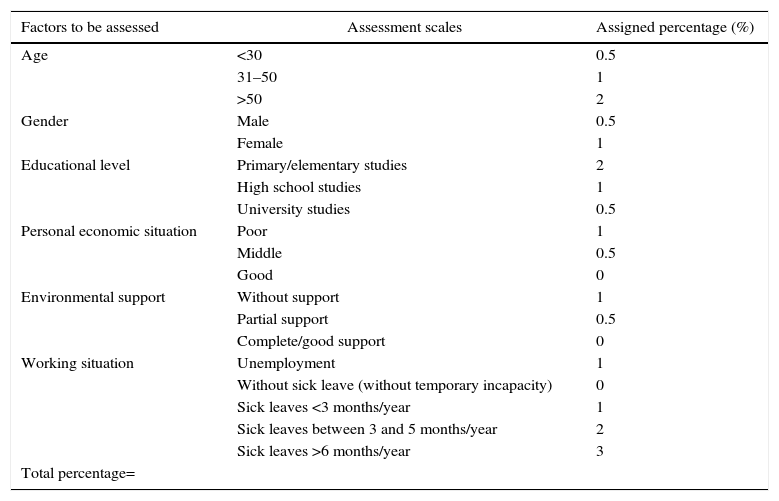
Assessment of personal aspects in fibromyalgia — FM-Check.
| Factors to be assessed | Assessment scales | Assigned percentage (%) |
|---|---|---|
| Age | <30 | 0.5 |
| 31–50 | 1 | |
| >50 | 2 | |
| Gender | Male | 0.5 |
| Female | 1 | |
| Educational level | Primary/elementary studies | 2 |
| High school studies | 1 | |
| University studies | 0.5 | |
| Personal economic situation | Poor | 1 |
| Middle | 0.5 | |
| Good | 0 | |
| Environmental support | Without support | 1 |
| Partial support | 0.5 | |
| Complete/good support | 0 | |
| Working situation | Unemployment | 1 |
| Without sick leave (without temporary incapacity) | 0 | |
| Sick leaves <3 months/year | 1 | |
| Sick leaves between 3 and 5 months/year | 2 | |
| Sick leaves >6 months/year | 3 | |
| Total percentage= | ||
The maximum percentage assigned to this block is 10% of the total.
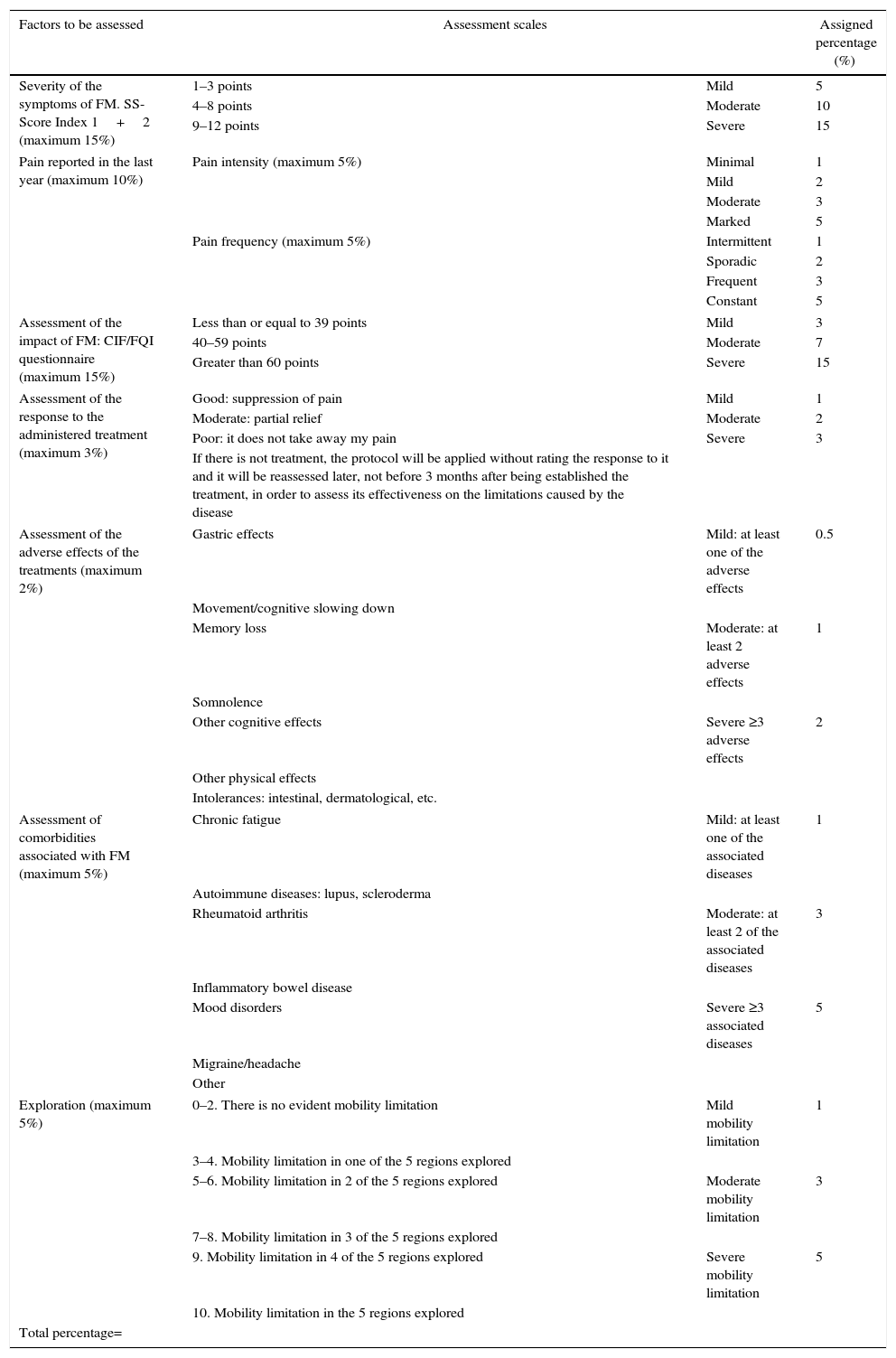
Assessment of the clinical and therapeutic aspects in fibromyalgia — FM-Check.
| Factors to be assessed | Assessment scales | Assigned percentage (%) | |
|---|---|---|---|
| Severity of the symptoms of FM. SS-Score Index 1+2 (maximum 15%) | 1–3 points | Mild | 5 |
| 4–8 points | Moderate | 10 | |
| 9–12 points | Severe | 15 | |
| Pain reported in the last year (maximum 10%) | Pain intensity (maximum 5%) | Minimal | 1 |
| Mild | 2 | ||
| Moderate | 3 | ||
| Marked | 5 | ||
| Pain frequency (maximum 5%) | Intermittent | 1 | |
| Sporadic | 2 | ||
| Frequent | 3 | ||
| Constant | 5 | ||
| Assessment of the impact of FM: CIF/FQI questionnaire (maximum 15%) | Less than or equal to 39 points | Mild | 3 |
| 40–59 points | Moderate | 7 | |
| Greater than 60 points | Severe | 15 | |
| Assessment of the response to the administered treatment (maximum 3%) | Good: suppression of pain | Mild | 1 |
| Moderate: partial relief | Moderate | 2 | |
| Poor: it does not take away my pain | Severe | 3 | |
| If there is not treatment, the protocol will be applied without rating the response to it and it will be reassessed later, not before 3 months after being established the treatment, in order to assess its effectiveness on the limitations caused by the disease | |||
| Assessment of the adverse effects of the treatments (maximum 2%) | Gastric effects | Mild: at least one of the adverse effects | 0.5 |
| Movement/cognitive slowing down | |||
| Memory loss | Moderate: at least 2 adverse effects | 1 | |
| Somnolence | |||
| Other cognitive effects | Severe ≥3 adverse effects | 2 | |
| Other physical effects | |||
| Intolerances: intestinal, dermatological, etc. | |||
| Assessment of comorbidities associated with FM (maximum 5%) | Chronic fatigue | Mild: at least one of the associated diseases | 1 |
| Autoimmune diseases: lupus, scleroderma | |||
| Rheumatoid arthritis | Moderate: at least 2 of the associated diseases | 3 | |
| Inflammatory bowel disease | |||
| Mood disorders | Severe ≥3 associated diseases | 5 | |
| Migraine/headache | |||
| Other | |||
| Exploration (maximum 5%) | 0–2. There is no evident mobility limitation | Mild mobility limitation | 1 |
| 3–4. Mobility limitation in one of the 5 regions explored | |||
| 5–6. Mobility limitation in 2 of the 5 regions explored | Moderate mobility limitation | 3 | |
| 7–8. Mobility limitation in 3 of the 5 regions explored | |||
| 9. Mobility limitation in 4 of the 5 regions explored | Severe mobility limitation | 5 | |
| 10. Mobility limitation in the 5 regions explored | |||
| Total percentage= | |||
The maximum percentage assigned to this block is 55% of the total.
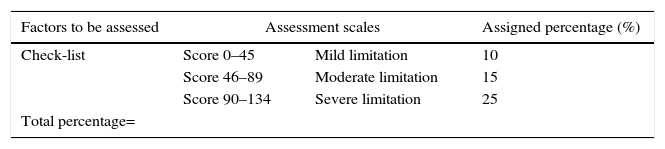
Assessment of the labor aspects in fibromyalgia — FM-Check.
| Factors to be assessed | Assessment scales | Assigned percentage (%) | |
|---|---|---|---|
| Check-list | Score 0–45 | Mild limitation | 10 |
| Score 46–89 | Moderate limitation | 15 | |
| Score 90–134 | Severe limitation | 25 | |
| Total percentage= | |||
The maximum percentage assigned to this block is 25% of the total.
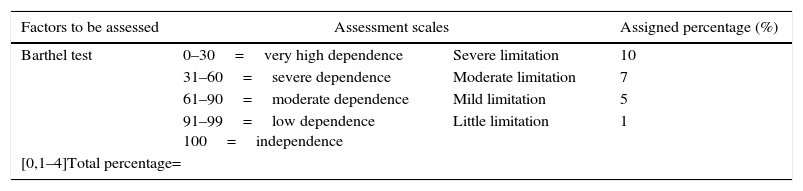
Assessment of the repercussion on the activities of daily life in fibromyalgia — FM-Check.
| Factors to be assessed | Assessment scales | Assigned percentage (%) | |
|---|---|---|---|
| Barthel test | 0–30=very high dependence | Severe limitation | 10 |
| 31–60=severe dependence | Moderate limitation | 7 | |
| 61–90=moderate dependence | Mild limitation | 5 | |
| 91–99=low dependence 100=independence | Little limitation | 1 | |
| [0,1–4]Total percentage= | |||
The maximum percentage assigned to this block is 10% of the total.
Assignment of the degree of limitation according to the overall percentage.
| Degree of limitation | Percentage of limitation (%) | Result |
|---|---|---|
| Grade 1 | <20 | Non-limiting |
| Grade 2 | 20–40 | Non-limiting or partial limitation |
| Grade 3 | 41–70 | Total permanent limitation |
| Grade 4 | >70 | Permanent limitation in need of help from a third person |
The percentage rating has been made according to the criteria of the authors.
The assessment of the limitations that a disease entails in relation to all aspects of an individual's life is complicated, especially when the disease is chronic, complex in its diagnosis, difficult to objectify and with very diverse responses and implications according to the type of patient affected, the different evolution and management, the way he/she assumes it and faces it, and its response to therapies.
The tool presented here is an attempt by the authors to unify different aspects of the same person in a way that limitations can be assessed as a whole, with purposes as diverse as estimating the evolution of the disease itself, its response to therapies, the restrictions for the performance of activities of daily living and its repercussion on work.
The way to “measure” the limitations related to a disease is always a challenge, and in order to reduce its complexity in fibromyalgia is provided this tool which is easy to use since it is computerized, although it is not exempt of the biases primarily associated with the selection made by the authors of the applied diagnostic tests, the scoring and percentages assigned to each section and the overall ones. Only its validation in a first stage and its subsequent use will be able to evidence its usefulness and the optional improvements that can be incorporated for greater efficacy in the results that will be obtained with it.
One of the most complex aspects is the assessment and quantification of the impact of the disease on the working capacity, due to the diverse demands associated with the different labor sectors and to the variability presented by each specific work performed by the patient. In the same way it is complex to assess the disability caused by the disease in relation to the decrease in his/her role as a person.15 For this reason, the authors have developed a check-list that takes as its basis the evaluation of risks prevention in our country, with a selection of those positions or labor requirements that can be more limiting for the patient with fibromyalgia and in which he/she can be more often affected in the performance of his/her daily work.
The medical bibliography on this topic reveals that it is a complex disease, whose diagnostic criteria are constantly discussed and reviewed, with continuous contributions to improvement16 and in which different types of tools are used, both for the diagnosis of the disease and for the estimation of the severity of the symptoms.17 The assessment of associated or concomitant diseases, such as cognitive and mood disorders18 or the influence of stress on the diagnosis itself and on the intensity of the symptoms,19, or the evaluation of specific aspects (anxiety, depression, physical fatigue, etc.) have shown great influence on the evolution and prognosis of the overall process.20,21
This group of authors has already collaborated previously in the development of tools for the evaluation of limitations, similar to those presented here, and in chronic conditions such as headaches, although with a fundamentally preventive-labor approach, but with the same objective of general vision of the affected patient.22
Will therefore serve this tool as an initial attempt or starting point for an overall assessment of the individual with fibromyalgia, being subject to the modifications that may be made in the future after its validation and use, both by the authors and by other professionals who work with it.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThere is no conflict of interest.
| Tasks | Not applicable | 1/3 of daily working hours | 2/3 of daily working hours | Full time | |
|---|---|---|---|---|---|
| Manual handling of loads | MHL ≤5kg | 0 | 1 | 2 | 3 |
| MHL 5–10kg | 0 | 2 | 3 | 4 | |
| MHL >10 and ≤25kg | 0 | 3 | 4 | 5 | |
| MHL >25kg | 0 | 4 | 5 | 6 | |
| Total score of manual handling of loads= | |||||
| Repetitive movements | RM shoulder elevation >90° | 0 | 2 | 4 | 6 |
| RM flexion–extension or pronation–supination of the wrist | 0 | 2 | 4 | 6 | |
| Flexion-extension of the trunk | 0 | 2 | 4 | 6 | |
| Total score of repetitive movements= | |||||
| Prolonged postures | Prolonged walking | 0 | 2 | 4 | 6 |
| Continued sitting | 0 | 2 | 4 | 6 | |
| Continued standing | 0 | 2 | 4 | 6 | |
| Total score of prolonged postures= | |||||
| Organization of the work | Performs continuous work without alternation of tasks | 0 | 2 | 4 | 6 |
| Performs repetitive/monotonous tasks | 0 | 2 | 4 | 6 | |
| Fixed postures without alternation of positions in his/her work | 0 | 2 | 4 | 6 | |
| Cannot take breaks to rest during work | 0 | 2 | 4 | 6 | |
| Is able to complete the tasks assigned to him/her in his/her work | 0 | 2 | 4 | 6 | |
| Has shift/night work (assess the monthly working hours) | 0 | 2 | 4 | 6 | |
| Total score of organization of the work= | |||||
| Working conditions | The workload is inadequate (excessive, irregular and not adapted to his/her abilities) | 0 | 2 | 4 | 6 |
| The environmental conditions of his/her work (temperature, humidity) worsen his/her clinical picture | 0 | 2 | 4 | 6 | |
| Does not have support elements for his/her tasks (devices, instruments, machines) | 0 | 2 | 4 | 6 | |
| Works at height (>3m) | 0 | 2 | 4 | 6 | |
| Works in confined spaces (tunnel, drain, ditch) | 0 | 2 | 4 | 6 | |
| Performs electrical work at high voltage | 0 | 2 | 4 | 6 | |
| Has to drive at work | 0 | 2 | 4 | 6 | |
| Handles machines or tools of risk | 0 | 2 | 4 | 6 | |
| Handles dangerous chemical substances | 0 | 2 | 4 | 6 | |
| Is exposed to biological contaminants | 0 | 2 | 4 | 6 | |
| Performs tasks that require high attention/concentration | 0 | 2 | 4 | 6 | |
| Total score of working conditions= | |||||
| (Total maximum score=134) | |||||
Please cite this article as: Vicente-Herrero MT, García LC, Ramírez Iñiguez de la Torre MV. Diseño de una herramienta para la valoración y clasificación de la limitación en fibromialgia. Rev Colomb Reumatol. 2017;24:131–137.
