



The prevalence of rheumatoid arthritis (RA) in Colombia is currently unknown. The purpose of this study was to estimate the prevalence of rheumatoid arthritis in Colombia using document bases.
Material and methodsA search was made of administrative sources for prevalent cases of RA reported by the Colombia 2005 Disease Burden study and the Servicing Individual Health Records, and corresponding to the International Classification of Diseases, tenth edition codes M05 and M06. The specific prevalences by sex and age were estimated by dividing the prevalent cases identified by the population bases reported by the National Bureau of Statistics in Colombia for the same year.
ResultsA total of 267,628 prevalent cases were found in Colombia in 2005. The overall prevalence of rheumatoid arthritis was 0.9/100 inhabitants, with a rheumatoid arthritis female/male ratio of 4:1. A progressive increase with age was observed (peaking in the group older than 80 years).
ConclusionThis is the first study of the prevalence of rheumatoid arthritis in Colombia based on administrative records. The prevalence for this methodology was similar to that found by other studies in populations of Europe and South America.
En Colombia, a la fecha, se desconoce la prevalencia de artritis reumatoide (AR). El propósito de este estudio fue hacer una aproximación a la prevalencia de la AR en Colombia con respecto a bases documentales.
Materiales y métodosMediante una revisión de bases administrativas, se identificaron los casos prevalentes de AR, notificados por el estudio Carga de Enfermedad Colombia 2005, de los Registros Individuales de Prestación de Servicios de Salud, correspondientes a la clasificación internacional de enfermedades, décima revisión, M05 y M06; dividiendo los casos prevalentes por las bases de población reportadas por el Departamento Nacional de Estadística en Colombia para el mismo año, se estimaron las prevalencias específicas por edad y sexo.
ResultadosSe encontraron 267.628 casos prevalentes en el año 2005 en Colombia, la prevalencia global de AR correspondió a 0,9/100 habitantes, la razón mujer/hombre de AR fue 4:1, se apreció un incremento progresivo con la edad (pico en el grupo de mayores de 80 años).
ConclusiónEste es el primer estudio de prevalencia de AR en Colombia con base en registros administrativos, la prevalencia por esta metodología fue similar a la encontrada por otros estudios en poblaciones de Europa y Sudamérica.
The estimation of the burden of this disease is of great importance to understand its impact on the health care services.1 Incidence and prevalence studies allow to assess the impact of the pathologies in the burden of disease and their resource consumption. The prevalence is the proportion that defines us the status of a disease in a specific point in time; it is usually used to measure the occurrence of degenerative diseases with unclear onset times.1,2 Knowledge of the prevalence is fundamental for the design of fair and equitable health policies that allow prioritization of technologies, optimal allocation of resources, and a greater coverage, which in the long term can reduce the burden of disease.3
Rheumatoid arthritis (RA) is a progressive and destructive polyarticular inflammatory disease, associated with pain and disability, with a highly significant impact on quality of life, job losses and poor social function, as well as high costs in community health care.4 It is the inflammatory disease mostly studied in the world, its prevalence in the Western Hemisphere ranges between 1% and 5%, and its clinical manifestations occur mainly between the third and the fifth decades of life, being, preferentially, of 3 women per each man.5
Several countries have identified the prevalence of arthritis in their population.5–13 However, applying surveys in large regions in order to identify patients (count), it has been considered that the measurements obtained by this methodology do not fully reflect reality; a very common option at this time is to use administrative databases.14 Currently, Colombia has a system of compulsory filling out by the healthcare providers for the regulation and control of the demand for health care services, the Registry of Provision of Healthcare Services (in Spanish: Registro de Información de Prestación de Servicios de Salud [RIPS]), the designation, structure and characteristics have been unified and standardized for all entities providers of healthcare services. The data of this record contain the identification of the provider of the healthcare service, of the user who receives it and the reason that originated its provision: diagnosis and external cause.15 The document Colombia 2005 Disease Burden compiled, from the RIPS, the incident and prevalent cases of a group of specific causes, which included the diagnosis of RA.16
The objective of this study is to estimate the point prevalence of RA in Colombia based on the burden of disease for the year 2005.
MethodsIt was calculated the point prevalence2 considered as the probability that an individual has to be a case at a given time or age; it is a proportion and it does not have dimension; its values range between 0 and 1. The point prevalence can refer to a population at a given time, to a population of a given age, or to a combination of both. It is calculated by dividing the number of existing cases in a given point of time (numerator) by the total population at that time (denominator). The point prevalence is the probability that an individual has to be a case at a given time or age.
Pt is the prevalence for the year 2005, Ct is the total number of cases of RA and by age groups for the year 2005 and Nt is the total population, population older than 16 years and by age groups for Colombia in the year 2005.
The prevalent cases in the RIPS15 of the international codes of the rheumatoid disease (M050–M060) by 2005, reported by CENDEX 200816 were identified in order to determine the prevalence of RA in Colombia; and it was determined their frequency with respect to the population bases reported by the National Administrative Department of Statistics (DANE) for the same year.
We found the absolute and relative frequencies stratified by age group for the prevalence of RA, in the general population in Colombia, of the same age and year.
The results were presented in tables and graphs, the cumulative prevalences for the year 2005 were presented taking as reference (denominator): the general population, and the population over 16 years by age groups.
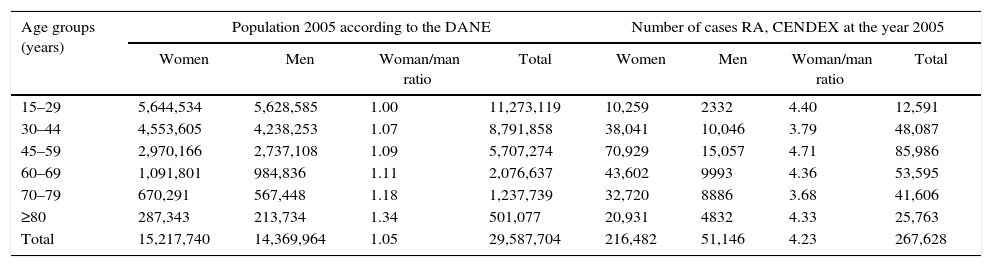
ResultsDuring the year 2005 the DANE reported a total population of 42,888,592; of these, 29,587,704 were 15 years and older (group under risk to assume criteria for RA by ACR 1987), the female/male ratio was 1.05; the age group that provided more data to this distribution was the one of 15–29 years old; the RIPS (CENDEX study 2008) recorded on the same year 267,628 cases of RA, with an overall femininity ratio of 4.23; the age group that provided more cases (85,986 cases) was the one of 45–59 years of age (Table 1).
DANE population and number of reported cases of RA by age groups and sex (ICD 10: M05–M06) Colombia 2005.
| Age groups (years) | Population 2005 according to the DANE | Number of cases RA, CENDEX at the year 2005 | ||||||
|---|---|---|---|---|---|---|---|---|
| Women | Men | Woman/man ratio | Total | Women | Men | Woman/man ratio | Total | |
| 15–29 | 5,644,534 | 5,628,585 | 1.00 | 11,273,119 | 10,259 | 2332 | 4.40 | 12,591 |
| 30–44 | 4,553,605 | 4,238,253 | 1.07 | 8,791,858 | 38,041 | 10,046 | 3.79 | 48,087 |
| 45–59 | 2,970,166 | 2,737,108 | 1.09 | 5,707,274 | 70,929 | 15,057 | 4.71 | 85,986 |
| 60–69 | 1,091,801 | 984,836 | 1.11 | 2,076,637 | 43,602 | 9993 | 4.36 | 53,595 |
| 70–79 | 670,291 | 567,448 | 1.18 | 1,237,739 | 32,720 | 8886 | 3.68 | 41,606 |
| ≥80 | 287,343 | 213,734 | 1.34 | 501,077 | 20,931 | 4832 | 4.33 | 25,763 |
| Total | 15,217,740 | 14,369,964 | 1.05 | 29,587,704 | 216,482 | 51,146 | 4.23 | 267,628 |
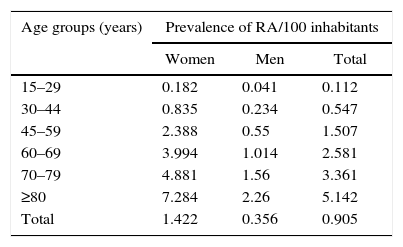
The standardized prevalence was higher as the age increased, yet it was found an overall prevalence (standardized to ≥15 years old) of 0.9 cases per 100 inhabitants (Table 2).
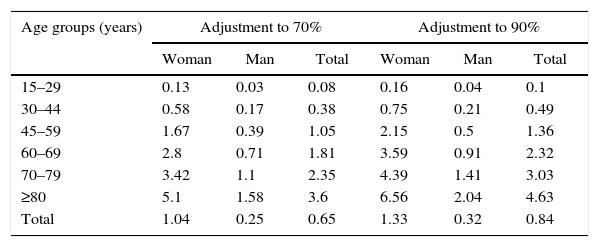
The results found were adjusted to 70% and 90%, so they allow to provide an approximation to the prevalence of seropositive RA in Colombia, for the year 2005,17 finding an approximate overall prevalence between 0.65 and 0.84 per 100 inhabitants (Table 3).
Cases of seropositive rheumatoid arthritis in Colombia during 2005, adjustments for M05: seropositive rheumatoid arthritis (adjustment to 70% and 90%).
| Age groups (years) | Adjustment to 70% | Adjustment to 90% | ||||
|---|---|---|---|---|---|---|
| Woman | Man | Total | Woman | Man | Total | |
| 15–29 | 0.13 | 0.03 | 0.08 | 0.16 | 0.04 | 0.1 |
| 30–44 | 0.58 | 0.17 | 0.38 | 0.75 | 0.21 | 0.49 |
| 45–59 | 1.67 | 0.39 | 1.05 | 2.15 | 0.5 | 1.36 |
| 60–69 | 2.8 | 0.71 | 1.81 | 3.59 | 0.91 | 2.32 |
| 70–79 | 3.42 | 1.1 | 2.35 | 4.39 | 1.41 | 3.03 |
| ≥80 | 5.1 | 1.58 | 3.6 | 6.56 | 2.04 | 4.63 |
| Total | 1.04 | 0.25 | 0.65 | 1.33 | 0.32 | 0.84 |
It is important that the development of studies on RA that direct the design of fair and equitable health policies, that allow the prioritization of technologies, optimal allocation of resources, and a greater coverage, that in the long term can reduce the disease burden.1
RA is a disease with a tendency to increase in some countries, but in Canada it demonstrated a high prevalence of RA in women (20%), being greater as age increased; given the growing trend to population aging in this country, is expected in the future a greater social burden of this disease, which demonstrates a need for strategies to mitigate the impact of arthritis.18,19
The present study shows an approach to the problem of the determination of the prevalence of RA in Colombia, and it offers a coherent methodology for utilization and organization of data, in addition of adjustments of the results to the general population, the population at risk (older than 15 years) and adjustments for subgroups (seropositive and seronegative arthritis). According to the information recorded for the year 2005, the overall prevalence of RA for Colombia was 0.905; the age group with the highest prevalence was the one older than 80 years and by gender, is the same group for women but in men it was the one of 45–59 years.
If we take into account that the coverage in the Colombian health system for the year 2005 was 85.05%, it could be adjusted to the total population recorded by the DANE, which would increase the prevalence (overall and discriminated by age groups) found in the present study. In this case, the overall prevalence would be 1.064%, a figure that is contained in the information provided by other authors for different countries.19
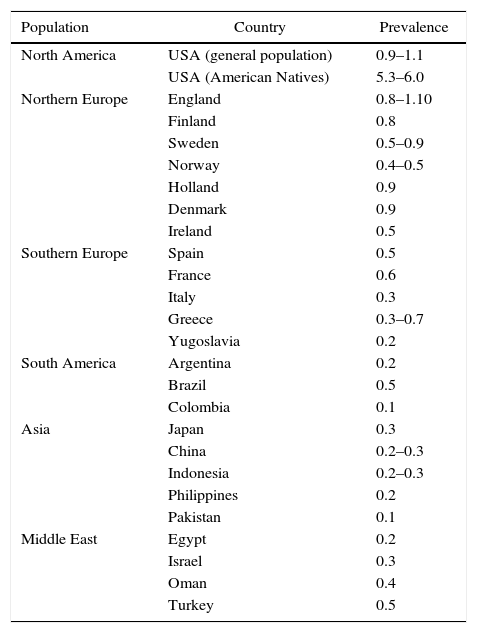
In Colombia, there are very few epidemiological studies that allow to determine the prevalence of RA; until now there is one study published in 1998,6 conducted in 1995, which estimated the prevalence of RA in 0.01 per 100 inhabitants (CI 95%: 0.008–0.02) in a sample of Afro-Colombian volunteers (people invited to free rheumatologic consultation) from the Department of Chocó. Some of the prevalences reported worldwide are shown in Table 4.
Prevalence rates of rheumatoid arthritis worldwide (cases per 100 inhabitants).
| Population | Country | Prevalence |
|---|---|---|
| North America | USA (general population) | 0.9–1.1 |
| USA (American Natives) | 5.3–6.0 | |
| Northern Europe | England | 0.8–1.10 |
| Finland | 0.8 | |
| Sweden | 0.5–0.9 | |
| Norway | 0.4–0.5 | |
| Holland | 0.9 | |
| Denmark | 0.9 | |
| Ireland | 0.5 | |
| Southern Europe | Spain | 0.5 |
| France | 0.6 | |
| Italy | 0.3 | |
| Greece | 0.3–0.7 | |
| Yugoslavia | 0.2 | |
| South America | Argentina | 0.2 |
| Brazil | 0.5 | |
| Colombia | 0.1 | |
| Asia | Japan | 0.3 |
| China | 0.2–0.3 | |
| Indonesia | 0.2–0.3 | |
| Philippines | 0.2 | |
| Pakistan | 0.1 | |
| Middle East | Egypt | 0.2 |
| Israel | 0.3 | |
| Oman | 0.4 | |
| Turkey | 0.5 |
Source: ICD-10-CM.26
To date it does not exist a standardized methodology to determine the prevalence of RA in a population,5–13 several countries have used as a method the studies of clinical records,5,11,13 others, the search using population surveys (as a screening measure) with subsequent evaluation of the suspected cases in representative samples,6–10,12 but all studies used as diagnostic criteria for this disease those proposed by the American College of Rheumatology.20 The prevalence may vary depending on the type of method. The active search for cases could generate an overvaluation of the prevalence to the extent that it detects new cases which in other circumstances would not have been diagnosed. The evaluation of clinical records has as selection bias the assessment of only the diagnosed patients who consulted (it excludes patients with asymptomatic arthritis, and patients without access to health care services) and at the time, the under-record or under-reporting of the RIPS has not been clearly established yet.21
The RIPS are mandatory medical records, completed by all providers of health services in Colombia, immediately after the medical care. A measure to estimate a prevalence based on these records, assuming in turn a stricter adherence to the use of the diagnostic criteria, would be by the exclusive review of the medical records of the specialized staff (Internists, specialists in Family Medicine and in Rheumatology) responsible for the definitive diagnosis and treatment of this disease; this has been done by studies subsequent to the Cendex study.16
Currently there is an increasing development of tools and methods for the surveillance of chronic rheumatic diseases based on the information from the administrative health databases,14,22 such as universal insurance,7 reinbursement23 and demand for services specialized in Rheumatology.24 The use of administrative data has been recognized by reviews prior to this one, as a validated method to determine the prevalence of RA.25
Given the finding in the medical records of multiple ICD 10 codes to indicate the same condition, the American College of Rheumatology has proposed the adoption of the ICD 10 M05.40 to M5.47 codes, as the codes that replace the formerly used ICD 9 diagnosis code 714.0 for the classification of RA.26
As weaknesses and limitations of this study it was found as a first step the use of non-standardized diagnoses to determine the prevalence of RA.26 The statistical adjustment to 70% and 90% to select the seropositive RA was carried out based on the findings of international studies,27 but it is possible that this frequency does not correspond to the Latin American population, particularly to the Colombian people. The prevalence of a disease varies according with the distribution of the ages of the population that makes it up, the entry of prevalence data from 15 to 80 years of age could lead to an overestimation of the frequency of RA. In the last few decades, several studies have reported a variable occurrence of the disease among different populations.19,28
These and other methodological considerations have been recognized in the past by other reviews as constraints for comparison, that is how, a review expanded in 2010 (of studies between 1965 and 2009) found as a methodological limitation to define the geoepidemiology in rheumatic diseases (including RA), the great diversity in temporal considerations, socio-economic factors and methodology of epidemiological studies for the comparison of the findings.19
In conclusion, in this clinical epidemiological study based on medical records, representative of the Colombian population, it was found a prevalence of 0.905 for users of the Health System over 15 years old, with an overall woman/man ratio of 4.23; figures that do not show differences with the studies published to date in different countries in Latin America, Europe and North America. The studies designed to date to determine the prevalence of RA show big methodological differences, there is no unity of methodological criteria to define the prevalence in RA and the use of administrative records as a source of data is an accepted method to determine the prevalence of this disease.25
Ethical responsibilitiesProtection of people and animalsThe authors declare that no experiments were performed on human beings or animals for this research.
Data confidentialityThe authors state that patient data do not appear in this article.
Right to privacy and informed consentThe authors state that patient data do not appear in this article.
FundingThis work was developed in the context of the Doctoral Thesis in Pharmaceutical Sciences of the National University by Jorge Augusto Díaz Rojas and directed by Professors Paul Brown and Fabio Aristizábal Gutiérrez.
Conflict of interestThe authors do not have any conflict of interest for the development of this work.
Please cite this article as: Díaz-Rojas JA, Dávila-Ramírez FA, Quintana-López G, Aristizábal-Gutiérrez F, Brown P. Prevalencia de artritis reumatoide en Colombia: una aproximación basada en la carga de la enfermedad durante el año 2005. Rev Colomb Reumatol. 2016;23:11–16.
