



The leading complication of antiphospholipid syndrome (APS) is arterial and venous thrombotic diathesis, which usually manifests as deep vein thrombosis or cerebrovascular events. However, it can occur in any blood vessel, rarely including the adrenal vessels. This can be the first manifestation of APS, and it is frequently bilateral and triggers adrenal insufficiency (Addison’s disease). It has been proposed that the initial phenomenon is thrombosis of the adrenal veins leading to infarction. Bilateral involvement is usually irreversible and requires permanent hormone replacement therapy. Unilateral involvement is even more infrequent and appears to have a better prognosis. We report the case of a 35-year-old female patient with a history of APS (repeated spontaneous abortions, livedo reticularis, presence of antiphospholipid antibodies and lupus anticoagulant), who presented with right adrenal infarction during the puerperium and whose clinical manifestation was sudden and severe lumbar pain. The diagnosis was made with contrast enhanced tomography. The patient made satisfactory progress, with no evidence of adrenal insufficiency.
La principal complicación del síndrome antifosfolípidos (SAF) es la diátesis trombótica, tanto arterial como venosa, que suele manifestarse como trombosis venosa profunda o diversos tipos de eventos cerebrovasculares; sin embargo, puede ocurrir en cualquier vaso sanguíneo, incluyendo muy ocasionalmente los vasos adrenales. Puede ser incluso la primera manifestación del SAF, y suele ser bilateral, con el consecuente desarrollo de insuficiencia adrenal (enfermedad de Addison). Se ha propuesto que el fenómeno inicial es una trombosis de las venas adrenales que condiciona un infarto. Con frecuencia, el compromiso bilateral es irreversible y requiere terapia de suplencia hormonal de forma permanente. La afectación unilateral es más rara y parece tener mejor pronóstico. Se reporta el caso de una paciente de 35 años con antecedente de SAF (abortos a repetición, livedo reticularis, presencia de anticuerpos antifosfolipídicos y anticoagulante lúpico), que presentó un infarto adrenal derecho durante el puerperio y cuya manifestación clínica fue dolor lumbar súbito e intenso. El diagnóstico se realizó con escanografía contrastada. La paciente ha evolucionado favorablemente, sin que se evidencie insuficiencia adrenal.
Antiphospholipid syndrome (APS) is an autoimmune disease characterized by the presence of autoantibodies directed against proteins associated with some phospholipids, the most common being anticardiolipin antibodies (ACA), anti β2-glycoprotein-1 antibodies, in addition to lupus anticoagulant (LA). Its main clinical manifestation are thrombotic phenomena, whether arterial or venous, or fetal losses related to placental insufficiency.1 Approximately 90% of the complications of APS correspond to deep vein thrombosis and ischemic cerebrovascular events,2 however, it is known that patients with APS may have thrombosis in any vessel.1 At the end of the decade of 1980s, adrenal insufficiency began to be described in the context of APS,3 and since then, adrenal involvement has been increasingly known and reported as a rare manifestation associated with this disease.4–7
The registry of adrenal infarction associated with APS is restricted to reports and case series in which bilateral thrombosis of adrenal veins that entails hemorrhagic phenomena is mainly described. Such thrombosis is reported as bilateral adrenal hemorrhagic infarction (AH-AI).5 The involvement of both glands is usually simultaneous or with a short period of difference.5,8,9 It is known that the main complication of AH-AI is adrenal insufficiency (Addison's disease). It has been possible to estimate in a cohort of patients with APS that only 0.4% develop it,4 however, it is the more frequent endocrine manifestation in APS.10 Adrenal insufficiency is characterized by a deficit in the adrenal production of glucocorticoids and mineralocorticoids, whose symptoms usually appear acutely when 90% of the adrenal cortex is destroyed, which is irreversible and requires long-term replacement therapy.5 It can occur in the context of catastrophic APS in 10–26% of cases and be life-threatening.6,7,11,12 On the other hand, unilateral non-hemorrhagic adrenal infarction (NHAI) which is rarer, has been described in few occasions associated with pregnancy outside of the context of APS.13–15
This report presents the case of a patient with unilateral non-hemorrhagic infarction in the context of APS that appeared in the puerperium.
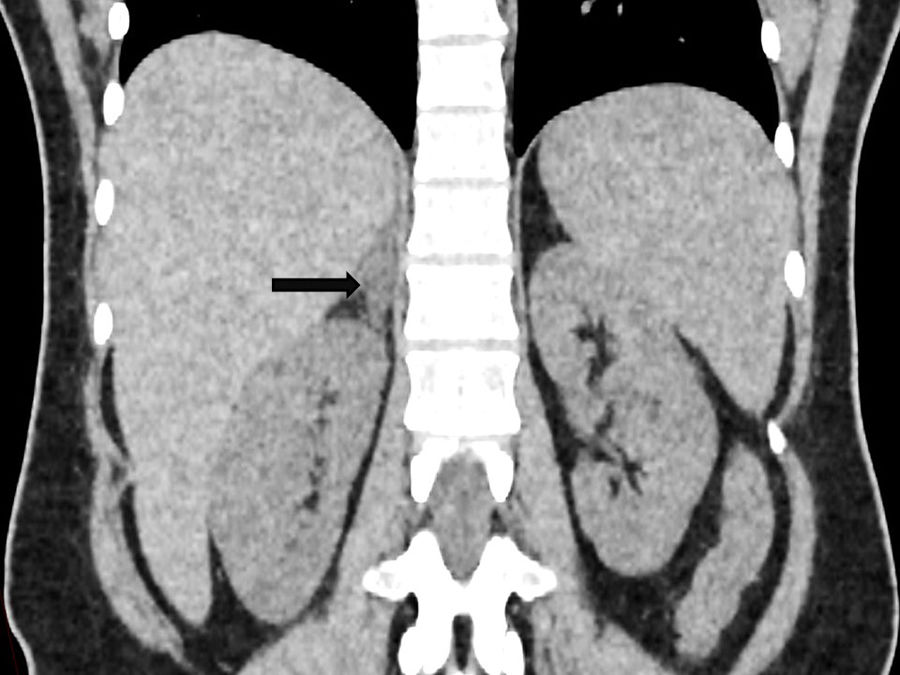
Description of the caseA 35-year-old patient with primary APS, with a history of first pregnancy with severe preeclampsia and stillbirth, second pregnancy that ended with abortion (no data of gestational age for that moment). The third and fourth pregnancies, during which she was treated with acetylsalicylic acid 100mg/day and subcutaneous enoxaparin at a dose of 1mg/kg/2 times daily were full-term and uncomplicated. Cesarean sections were performed in both successful pregnancies. The patient did not have other relevant antecedents or previous episodes of DVT or other thrombotic or hemorrhagic events. On physical examination, only livedo reticularis in upper and lower limbs was observed. The patient had triple positivity for antiphospholipid antibodies: anti-β2-glycoprotein-1, ACA (IgM and IgG) and LA. During puerperium, 11 days after her last cesarean section, she presented sudden pain in the right flank and lumbar region. On physical examination she was found afebrile, with a blood pressure of 110/68mmHg, the rest of vital signs were normal, presenting painful right lumbar fist percussion. The laboratories showed: leukocytes 9500/μl; hemoglobin 11.5g/dl; platelets 242,000/μl; sodium 139mmol/l; potassium 4.32mmol/l; increased C-reactive protein (11.8mg/dl); erythrocyte sedimentation rate 34mm/h; alkaline phosphatase 339U/l; AST 38U/l; ALT 65U/l; triglycerides 551mg/dl and PTT 60.5s. The urinalysis showed no alterations, and the blood cultures and urine culture that were taken were negative. It was performed a computed axial tomography of the abdomen in which diffuse hypodensity was found in the right adrenal gland, with striation of adjacent fat, while the left gland presented normal enhancement; these changes suggested a right adrenal infarction (Fig. 1). An abdominal ultrasound revealed mild changes of fatty liver.

The patient received acetaminophen and 2 doses of intravenous opioid with control of pain, her levels of cortisol and ACTH were17.9μg/dl and 13.7pg/ml, respectively. The treatment has been based on continuing acetylsalicylic acid and anticoagulation, initially with enoxaparin, which was switched to warfarin. Gemfibrozil was also indicated, and it was decided to stop breastfeeding due to severe mastodynia. The levels of potassium, sodium, cortisol, ACTH, and other follow-up tests continued normal 2 weeks after the event.
DiscussionIt has been proposed that the vascular phenomena that occur in the adrenal glands in patients with APS must have their origin in venous thrombosis, which manifests itself as hemorrhagic or non-hemorrhagic infarctions.7 The presence of an arterial type event is less likely, since the adrenal gland has a broad arterial irrigation thanks to the superior suprarenal artery (coming from the inferior phrenic arteries), the middle suprarenal artery (from the abdominal aorta) and the inferior suprarenal (from the renal arteries), which together guarantee adequate perfusion and make it unlikely that an arterial thrombus generates a generalized adrenal thrombosis.8 On the other hand, its venous drainage is accomplished through a single adrenal vein,16 which implies a greater predisposition to thrombotic events followed by reperfusion through necrotic vessels, which in most cases triggers secondary hemorrhagic phenomena.9 It has also been described that the eccentric arrangement of the muscles of the adrenal veins can favor the formation of thrombi in pockets of turbulence or local stasis that are generated during their contraction.5,16,17
What is exposed in the precedent lines explains the findings of the imaging studies in a case series that included 86 patients with APS and adrenal involvement.7 Magnetic resonance imaging or computed axial tomography was performed to 69 of these patients, 40 (57%) of them presented adrenal hemorrhage and 10 (14%) infarction. Among the patients with adrenal infarction, 7 had a hemorrhagic component and only 3 presented isolated adrenal infarction without bleeding; in addition, the findings were unilateral only in 23%. Remarkably, in almost all cases of unilateral NHAI in pregnancy, the affected adrenal gland has been the right; it has been suggested that this may be due to the compression of the inferior vena cava which directly receives drainage from the right adrenal vein, while in the left side the drainage goes first to the left renal vein.18
In addition to anatomical and vascular considerations, it has also been suggested that adrenal tissue, having a high lipid traffic, could provide specific epitopes from late endosomes and bisphosphatidic acid (LBPA), which in turn could attract antiphospholipid antibodies and alter local hemostatic mechanisms,8 that might explain the selective affectation in some patients. It has been found that between 60 and 90% of patients with APS and adrenal involvement have triple positivity for antiphospholipid antibodies.5,7
Complications associated with adrenal infarction, whether or not hemorrhagic, occur more frequently in patients previously diagnosed with APS, and rarely as onset of the disease. However, there are multiple reports of AH-AI or adrenal insufficiency as the first manifestation of APS.5,19–21 In patients with a previous diagnosis of APS, the suspension of anticoagulation or the lack of adequate levels of anticoagulant medication could act as precipitants of this complication,22 while other stressful circumstances such as a major or gynecological surgery, infections, pregnancy or puerperium can favor the development of this entity.7 It has been described that among patients who develop adrenal insufficiency the average age is 33–43 years, and 55% of cases occur in males.5,7
The main symptom in patients with hemorrhagic or non-hemorrhagic infarctions is abdominal pain,6,7,13,14 followed by fever, nausea, vomiting, hypotension and altered state of consciousness; the last 2 associated with the development of adrenal insufficiency, which usually has an acute presentation, with hyponatremia, hyperkalemia and hypotension secondary to the deficiency of aldosterone and cortisol.7,23 It occurs most frequently with bilateral involvement, with irreversible damage, progressive adrenal atrophy, and need for long-term replacement therapy.23 Usually, the medullary adrenal function is not impaired.5 Another complication is the recurrence of thrombosis. In this sense, it has been suggested that close follow-up and a target INR of 3–3.5 can achieve thrombosis rates of 2.9% without increasing the bleeding rate, compared to what has been described in the literature.5,24
The tomography usually reveals bilateral adrenal hypo- or hyperdensity, corresponding to infarction and hemorrhage, respectively, without radiological changes that suggest autoimmune adrenal involvement or infection. Magnetic resonance imaging shows additional benefit by providing data on chronicity in cases of hemorrhage,7 and the imaging changes usually persist, with loss of adrenal tissue observed during follow-up.8
Laboratory follow-up is performed with morning baseline cortisol levels and cortisol response to ACTH test; observing long-term persistence of hormonal deficiency.5,22
In the case of our patient, there was no acute adrenal insufficiency nor at follow-up, which may be associated with the unilateral involvement. Previously, 2 patients with unilateral involvement were described, who during follow-up at 7 and 13 years continued with normal adrenal function and normal morphology of the initially affected gland, in control images 1 and 2 years after onset,5 which indicates a more benign behavior in this subgroup of patients.
Thus, an atypical case of right non-hemorrhagic adrenal infarction in the puerperium of a patient with APS, previously manifested with maternal-fetal morbidity and triple positivity of antiphospholipid antibodies is reported. This pathology manifests itself with the presence of sudden lumbar or abdominal pain, which should warn the attending physician of this type of disease for active search by contrasted tomography or magnetic resonance imaging. Unilateral adrenal infarction does not lead to hormonal insufficiency, but it is important to be alert for the potential risk of infarction in the healthy adrenal gland. Treatment should be long-term anticoagulation.
Informed consentThe authors obtained informed consent for the use of data and images of the patient described in this case report.
FundingNo entity provided economic funding for the development of the study and the preparation of the article.
Conflict of interestAll authors declare that they have no conflict of interest for the preparation of this article.
