

A retrospective study was undertaken to assess causes of maxillofacial trauma in Recife, Pernambuco, Brazil.
MethodA review of 186 patients with maxillofacial injuries aged 19 and 83 years old seen and treated at the Hospital da Restauração between January and December 2006 was conducted and were analyzed according to age, sex, etiology, site of fracture, dentoalveolar trauma and alcohol abuse. Analysis was made in Epi Info using the Chi-square and Fisher's Exact Tests.
ResultsIt was found that maxillofacial injuries were most frequent in males (89.2%) and in the 19–28 year age group (46.8%). Traffic accidents/motorcycle (23.7%) and physical violence (20.4%) were the most common etiological factor. Facial fractures were detected in 90.9% and a statistically significant difference between sex and facial fracture was found (p = 0.000). The most common facial fracture was maxilla (29.1%), followed by the mandible (27.5%). A positive association between the presence of facial fracture and alcohol consumption was observed (p = 0.002). Dentoalveolar trauma was present in 7.5% of patients.
ConclusionThe incidence of facial fractures in Brazilian population is similar than previously reported elsewhere. There were most common in male patients, mainly due to traffic accidents/motorcycle and physical violence.
Se llevó a cabo un estudio retrospectivo para evaluar las causas de traumatismo maxilofacial en Recife, Pernambuco, Brasil.
MétodoSe hizo una revisión de 186 pacientes con lesiones maxilofaciales de 19 a 83 años atendidos y tratados en el Hospital da Restauração entre Enero y Diciembre 2006, analizándoles según edad, sexo, etiología, localización de la fractura, traumatismo dentoalveolar y abuso de alcohol. Se llevó a cabo el análisis en Epi Info, utilizando el Chi cuadrado y la prueba exacta de Fisher.
ResultadosResultó que las lesiones maxilofaciales fueron más frecuentes en los hombres (89,2%) y en el grupo de edad de 19-28 años (46,8%). Accidentes de tráfico/motocicleta (23,7%) y violencia física (20,4%) fueron los factores etiológicos más comunes. Las fracturas faciales fueron detectadas en 90,9%, con una diferencia estadisticamente significativa entre el sexo y la fractura facial (p = 0,000). La fractura facial más común fue maxilar (29,1%), seguida por la de la mandíbula (27,5%). Hubo una asociación positiva entre la presencia de la fractura facial y el consumo de alcohol (p = 0,002). El traumatismo dentoalveolar estuvo presente en el 7,5% de los pacientes.
ConclusiónLa incidencia de las fracturas faciales en la población Brasileña es similar a la informada previamente en otros lugares. Las fracturas fueron más comunes en pacientes masculinos, principalmente debidas a accidentes de tráfico/motocicletas y a la violencia física.
The human face constitutes the first contact point in several human interactions, thus injuries and/or mutilation of the facial structures may have a disastrous influence on the affected person1. There are numerous published reports on the incidence of maxillofacial injuries in different countries2-8.
Road traffic accidents, assaults and fights, falls, sports injuries, industrial accidents, home accidents and domestic violence, gunshot/firearm injuries and animal bites/accidents are the commonly recognized and reported etiological factors1,3,6,9. These etiologic factors are influenced by such factors as geography, social trends, alcohol and drug abuse, road traffic legislations, and seasons of the year10.
In the more developed countries of Europe, violence followed by road crashes are the predominant causes while in the developing world the causative factors are reversed with most being the result of road crashes2.
The age distribution of persons sustaining craniomaxillofacial injuries differs from one country to another10. The mean age of presentation is between second and third decades of life, and with respect to sex distribution previously males were more commonly involved1,4,7.
Although few studies on maxillofacial fractures from Brazil are found in medical literature11-13.
The aim of the present study was to analyze the etiology and pattern of maxillofacial injuries in patients aged 19 and 83 years in the Recife City, Pernambuco, Brazil.
MethodsThe protocol was approved by the State University of Paraiba ethics review committee. The records of all patients with facial injuries between the ages of 19 and 83 years who were treated at the Hospital da Restauragao, Recife, Brazil, between the beginning of January 2006 and the end of December 2006 were retrospectively examined. Data were analyzed according to age, sex, etiology of the injury, anatomic location of facial fractures, soft tissue injuries, dentoalveolar injury and alcohol abuse.
The etiology was classified as: traffic accidents (cars, motorcycles and pedestrian), physical violence, accidental falls, sports accidents, weapon injuries (knife and fire gun), bicycle accidents and other causes. Mandibular fractures were grouped into condylar, coronoid, ramus, angle, body, parasymphyseal, symphyseal, and dentoalveolar. Dentoalveolar injuries included: avulsion, tooth fracture, luxation and concussion.
Data analysis included descriptive statistics such as frequency distribution and cross tabulation. Comparisons of data were evaluated statistically using the Chi-square and Fisher's Exact Tests at a significance level of 5% (p<0.05). Odds ratio (OR) with confidence intervals to 95% were calcu- lated (CI 95%). They were calculated using the Epi Info Software (Centers for Disease Control and Prevention, CDC, Atlanta, USA).
ResultsAge and sex distributionOver all injuries, 57% were sustained during the weekend (Friday, Saturday or Sunday). Wednesday was the day on which fewest maxillofacial injuries was sustained (7.5%).
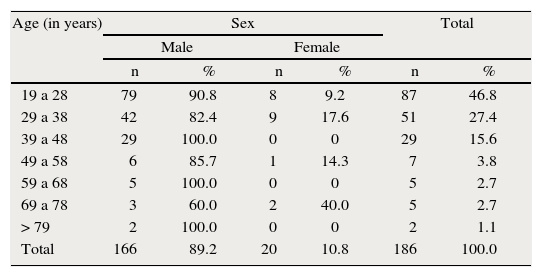
The average age was 33.2 (standard deviation [SD] 13.1 years). There were 166 male (89.2%) and 20 female (10.8%), a ratio of 8.3:1. Starting after the third decade of life, the overall age distribution shows a decreasing accident rate with each new decade. The most common age group involved was 19 and 28 years (46.8%) (table 1).
Distribution of patients by age and sex
| Age (in years) | Sex | Total | ||||
| Male | Female | |||||
| n | % | n | % | n | % | |
| 19 a 28 | 79 | 90.8 | 8 | 9.2 | 87 | 46.8 |
| 29 a 38 | 42 | 82.4 | 9 | 17.6 | 51 | 27.4 |
| 39 a 48 | 29 | 100.0 | 0 | 0 | 29 | 15.6 |
| 49 a 58 | 6 | 85.7 | 1 | 14.3 | 7 | 3.8 |
| 59 a 68 | 5 | 100.0 | 0 | 0 | 5 | 2.7 |
| 69 a 78 | 3 | 60.0 | 2 | 40.0 | 5 | 2.7 |
| > 79 | 2 | 100.0 | 0 | 0 | 2 | 1.1 |
| Total | 166 | 89.2 | 20 | 10.8 | 186 | 100.0 |
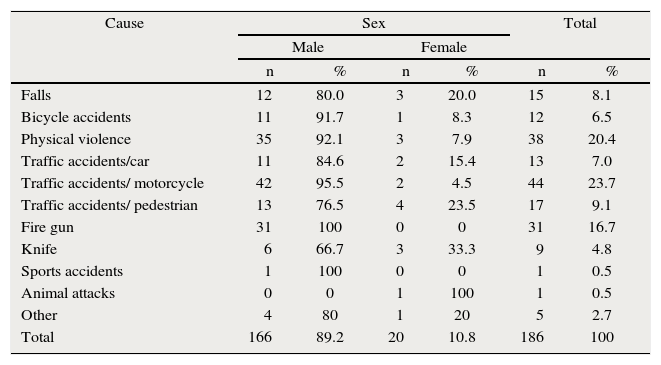
The distribution of the various etiologic factors among the sex is shown in table 2. The most frequent cause was traffic accidents/motorcycle, with 44 cases (23.7%), followed by physical violence with 38 cases (20.4%).
Distribution of patients by etiology and gender
| Cause | Sex | Total | ||||
| Male | Female | |||||
| n | % | n | % | n | % | |
| Falls | 12 | 80.0 | 3 | 20.0 | 15 | 8.1 |
| Bicycle accidents | 11 | 91.7 | 1 | 8.3 | 12 | 6.5 |
| Physical violence | 35 | 92.1 | 3 | 7.9 | 38 | 20.4 |
| Traffic accidents/car | 11 | 84.6 | 2 | 15.4 | 13 | 7.0 |
| Traffic accidents/ motorcycle | 42 | 95.5 | 2 | 4.5 | 44 | 23.7 |
| Traffic accidents/ pedestrian | 13 | 76.5 | 4 | 23.5 | 17 | 9.1 |
| Fire gun | 31 | 100 | 0 | 0 | 31 | 16.7 |
| Knife | 6 | 66.7 | 3 | 33.3 | 9 | 4.8 |
| Sports accidents | 1 | 100 | 0 | 0 | 1 | 0.5 |
| Animal attacks | 0 | 0 | 1 | 100 | 1 | 0.5 |
| Other | 4 | 80 | 1 | 20 | 5 | 2.7 |
| Total | 166 | 89.2 | 20 | 10.8 | 186 | 100 |
A total of 169 patients (90.9%) had facial fractures. This sample consisted of 159 man (94.1%) and 10 women (5.9%) and a statistically significant difference between sex and facial fracture was found (p=0.000; OR 22.71 [7.13-72-32]). Eighty-five patients (50.3%) sustained single fractures, 41 patients (24.3%) had two fractures, 28 patients (16.6%) had three fractures and 15 (8.8%) had multiple (four or more) fractures. A total of 375 fractures were registered, representing 2.2 fractures per patient.
Type and location of fracturesThe most common facial fracture was maxilla (29.1%), followed by the mandible (27.5%), zygomatic-orbital complex (20.2%), nasal (9.6%), frontal (8%), and naso-orbital-ethmoid (5.6%). The most common mandibular fracture site were the symphyseal and parasymphyseal regions (28.8%), the body (23.3%), the condyle (18.5%), the angle (15.8%), the ramus (6.8%), the mandibular dentoalveolar (4.1%), and the coronoid (2.7%).
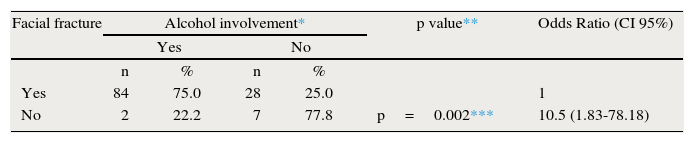
The table 3 shows a positive association between the presence of facial fracture and alcohol consumption (p=0.002). According to these data, patients who reported drin- king alcohol have 10.5 times more chance of have facial fracture.
Maximum patients had mixed type of injury i.e. soft tissue and bone involvement (89.8%), followed by soft tissue only (9.7%) and bone only (0.5%). Those patients sustained soft tissues injuries, 32 patients (17.3%) sustained single soft tissues injuries, 70 patients (37.8%) had two injuries, 50 patients (27%) had three injuries and 33 (17.8%) had multiple (four or more) soft tissues injuries. A positive association between the presence of facial fracture and the number of soft tissues injuries was observed (p=0.002). Soft tissue injuries in the form of edema (58.6%), followed by ecchymosis (24.7%) and hematoma (16.7%) were the most common types of injury.
A total of 89 patients (47.8%) had orofacial injuries and no statistically significant difference between the presence of orofacial injuries and facial fracture was found (p=0.064; OR 3.28 [1.03-10.49]). Dentoalveolar trauma was present in 7.5% of the patients. The most common injury was avulsion (35.7%) and teeth fractures (35.7%), followed by subluxation (21.5%) and intrusion (7.1%).
The 186 patients admitted to the hospital had a length of stay (LOS) totaling 3.137 days (average LOS of 16.8 days per patient; one patient had a 125-day LOS).
DiscussionInjuries to the craniomaxillofacial area affect a significant number of trauma patients, and consequences of trauma to this region can include any combination of dental, bone, or soft tissue injury10.
Most patients with facial injuries were seen on the wee- kend (Friday, Saturday or Sunday), similar to previous report7. These are days of great opportunity for outdoor and sports activities, short trips, recreation. Especially in Brazil, most soccer games occur on weekends, increasing the risk of violence among fans. Also, alcohol intake is greater on weekends11.
The sex distribution in the present study is consistent with that of others, with a higher frequency of craniomaxillofacial fractures in males compared with females4-6,9,11,13,14. This study found a higher male-to-female ratio (8.3:1) than was noted in previous study in Chennai7 (3.7:1), in Tehran1 (4.5:1) and in United Arab10 (7:1). This male-to-female ratio is attri- buted to the fact that men are more involved in outdoor activities and more frequently exposed to violent interactions10,11.
Maxillofacial trauma is most common in the third decade, consistent with much of the international literature. The age distribution in this study showed that the most common age group involved was 19 and 28 years, in agreement with previous reports5,10,11,13,15. The highest incidence in this age group is due to the fact that this age group take part in dan- gerous exercises and sports, drive motor vehicles carelessly, and are most likely to be involved in violence4,16.
The etiology of maxillofacial injuries varies from one coun- try to another and even within the same country depending on the prevailing socioeconomic, cultural and environmental factors3,7,9,11,17.
Traffic accidents have been the most common cause of maxillofacial injuries worldwide as reported in most previous epidemiologic studies1,6,13,14,16 and the present study supports the findings of these earlier studies, showing that traffic acci- dents (car, pedestrian and motorcycle) represents 39.8% of all etiological factors. In this study, 23.7% of cases with maxillo- facial injuries were involved in motorcycle related crashes. Similar studies have shown that the incidence of motorcycle crashes in other developing countries is about 19-62%7,18. Motorcycles have become a prominent mode of transportation in both urban and suburban cities in Brazil.
The World Health Organization (WHO) has estimated that nearly 25% of all injury fatalities worldwide are a result of road traffic crashes, with 90% of the fatalities occurring in the low and middle-income countries19.
Traffic accidents have a special relevance and a negative impact not only for their costs, but also for the pain, suffering and loss of life quality that are inflicted to the victims, their relatives and society as a whole. Perhaps specific measures are needed with respect to training of motorcyclists, definition of requirements for delivery services, improvement in education campaigns and inspection of proper helmet use12.
Physical violence was the second most common cause of maxillofacial injuries in adults. Perhaps, robbery, excessive drinking and the high index of violence12 in Recife can explain the number of aggression-related maxillofacial injuries. Violence prevention programs focusing on both assault and self- inflicted injury may help decrease the maxillofacial trauma resulting from intentional injuries among the population11.
The maxilla was the most frequently involved bone in this study, followed by the mandible. These findings were similar to other studies that reported maxilla fractures as the most frequent site of injury8. Mandibular fractures were reported to be commoner than maxilar fractures11,13,16. The site depends on the mechanism of injury8.
In this study, the most common mandibular fracture site were the symphyseal and parasymphyseal regions, the body, the condyle and the angle. According to previous reports parasymphyseal regions7 and the body12,16 are the most frequently injured region of the mandible.
The average number of facial fractures per patient was 2.2. Larger series of facial fractures have found lower numbers of fractures per patient, ranging from 1.220 to 1.511,14. The higher average number of fractures per patient could be explained by the fact that the mechanism of injury in this study population was predominantly traffic accidents, that tend to cause a greater number of fractures per patient because of a higherforce of impact12,20.
In the study reported here, alcohol was associated with about 75% of facial fractures, a proportion significantly hig- her. Some studies have shown a high correlation between alcohol consumption and maxillofacial injuries3,21,22. Our finds showed that alcohol consumption was strongly associated with the occurrence of facial fractures. Clearly there is evidence of increased morbidity in patients who abuse alcohol and present with facial fractures.
This study showed a positive association between the presence of facial fracture and the number of soft tissues injuries (p=0.002). Edema, ecchymosis and hematoma were the most common types of injury.
Orofacial injuries were detected in 47.8% of patients, but no statistically significant difference between the presence of orofacial injuries and facial fracture was found. Dentoalveolar trauma showed a lower incidence in the adult population, similar to previous report8. Avulsions and teeth fractures were the more prevalent types of dental trauma.
An understanding of the cause, severity and temporal distribution of maxillofacial trauma can assist in establishing clinical and research priorities for effective treatment and prevention of these injuries17. Therefore, more evaluation studies should be conducted to assess the physical, social and psychological quality of life for patients affected with maxi- llofacial trauma.
ConclusionsThe incidence of facial fractures in Brazilian population is similar than previously reported elsewhere. There were most common in male patients, mainly due to traffic accidents/ motorcycle and physical violence, and the maxilla followed by the mandible were the most frequently involved bones. It was observed a positive association between alcohol consumption and the occurrence of facial fractures.
DiscusiónA. Valiente Álvarez(Jefe de Servicio de Cirugía Oral y Maxilofacial, Hospital Universitario Carlos Haya, Málaga, España.)
He leído con interés este artículo en el que se hace un estudio epidemiológico sobre traumatología facial en una zona geográfica determinada como es Recife, capital de Pernambuco, al nordeste de Brasil, y llama la atención cómo no se relaciona la muestra con la población general ni las características especiales de la zona, como son su influencia turística por sus playas y carnavales y por su población, de aproximadamente un millón y medio de habitantes (la población del estado de Pernambuco es de ocho millones).
En primer lugar debemos considerar que no es fácil actualmente encontrar estudios sobre traumatología facial en países desarrollados y sí en aquellos que están en vías de desarrollo, quizá por la disminución de la casuística debido en gran parte al cumplimiento de las normas de tráfico, el aumento de la seguridad vial y la tecnología de los medios de locomoción. Las series se estudian en países tales como Nigeria o India, y les puedo asegurar que después de patearme de norte a sur este último país, creo que es un auténtico milagro que la traumatología facial no sea una epidemia como la gripe. De todas maneras, en países desarrollados tal como el nuestro, hasta hace unos meses en una preciosa ciudad del sur se llegó a regalar el casco a los motoristas, y ni por esas.
La muestra puede ser significativa (169 pacientes en un año) y es tratada teniendo en cuenta unos factores que pueden considerarse universales, tales como su relación estacional con clara referencia al alcohol en fines de semana y el uso de la motocicleta.
Se echa de menos la casuística precisamente en el grupo, desde mi punto de vista, más interesante, el de los niños, ya que aunque se ve que el grupo más relevante es entre 19 y 28 años, el estudio del grupo infantil revelaría el enorme cambio que está sufriendo nuestra sociedad, ya que desde edades muy tempranas el acceso al alcohol, las drogas, los vehículos de motor, las agresiones, etc. se ha incrementado mucho.
Realmente creo que el estudio tiene más valor desde el punto de vista sociológico que desde el punto vista clínico, y a través del mismo podemos apreciar que en general no estamos tan lejos unos de otros. La relación entre sexos es superponible dependiendo de la región geográfica, por ejemplo 8:1 en la muestra brasileña es significativa con la de 3:1 en la muestra de la India, y es que como antes indicaba, es frecuente en este último país que la familia entera (cuatro miembros de media) viaje en la misma moto por una autopista de cuatro carriles en sentido contrario y en la que tienen cabida, todos a una, camellos, elefantes, tractores, autobuses y camiones (por supuesto sin luces).
Es claro el enorme aumento del trauma facial originada por la violencia y su relación con el alcohol, aunque debemos considerar también la violencia de género y hacer notar que incluso ahora es complicado en muchos casos convencer a la agredida para que haga la denuncia.
La muestra indica una mayor incidencia en el maxilar superior superponible a la mayoría de los estudios, ya que la mandíbula se considera hueso único frente al tercio medio facial, incluidas las fracturas nasales. Con respecto a la mandíbula, llaman la atención los porcentajes de incidencia en su clasificación anatómica, con baja incidencia condílea frente al 2,7% de afectación de coronoides.
Del mismo modo, la incidencia de trauma dentoalveolar (7,5%) es significativamente baja en relación a otras series.
Llama la atención la estancia media de 16,8 días, aunque uno de los pacientes estuvo 125. Sería interesante comprobar la correlación con la estancia preoperatoria, la cual no está citada en el estudio.
En referencia a la discusión, es una enumeración de los datos obtenidos y prácticamente se elabora un perfil del paciente traumatizado facial, el cual independientemente de las variables socioeconómicas y culturales, podría ser universal tal como varón joven que en fin de semana, con medio de automoción mecánico, sale a divertirse durante horas y consume alcohol u otro tipo de drogas. Creo que con esto está dicho todo.
