


The histological classification of the World Health Organization (WHO), along with improved imaging studies, provide relevant information for the management of parotid carcinomas. However, the prognosis depends on factors other than histology and tumor extension. This article evaluates the usefulness of a prognostic classification of parotid cancers, including these factors in patients in a hospital area.
MethodsA follow-up was conducted on 19 patients with parotid carcinomas, excluding lymphoid tumors or intra-parotid metastases, between 1998 and 2012. The prognostic index was obtained from the formulas proposed by Vander Poorten, with factors including age, tumor size, lymph node involvement, skin invasion, facial nerve involvement, perineural growth and margins of resection, before surgery (PS1) and after (PS2). Overall survival was related to 5 years for each patient based on their inclusion in any of the 4 risk groups defined.
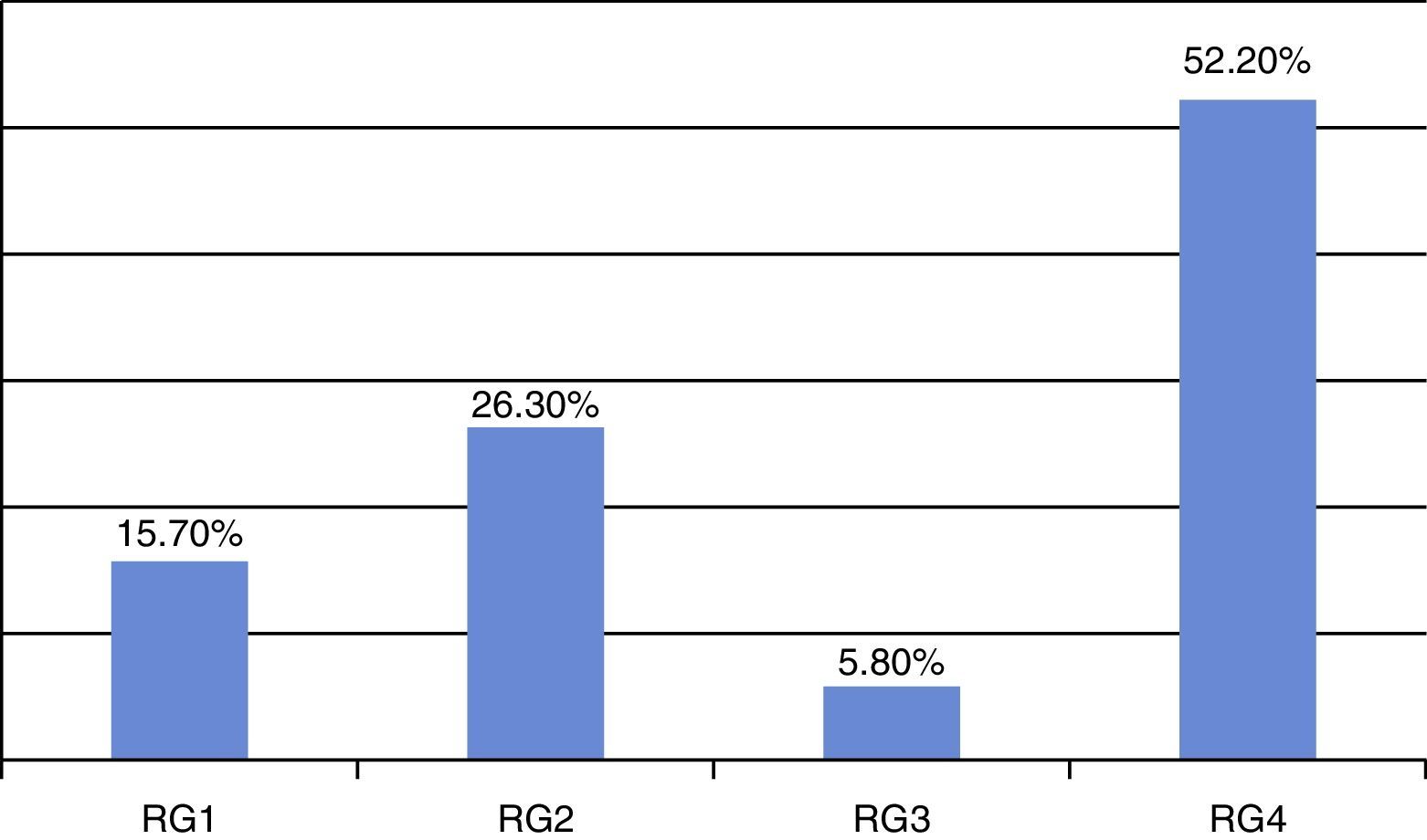
ResultsRisk stratification based on the results Vander Poorten PS2 was distributed into Risk Groups (GR) 1 (3 patients, 15.7%), 2 (5 patients, 26.3%), 3 (1 patient, 5.8%) and 4 (10 patients, 52.2%). The 6 patients who died during follow-up belonged to GR4. Only one of the 4 patients belonging to GR4 has exceeded the 5-year survival up to the current time.
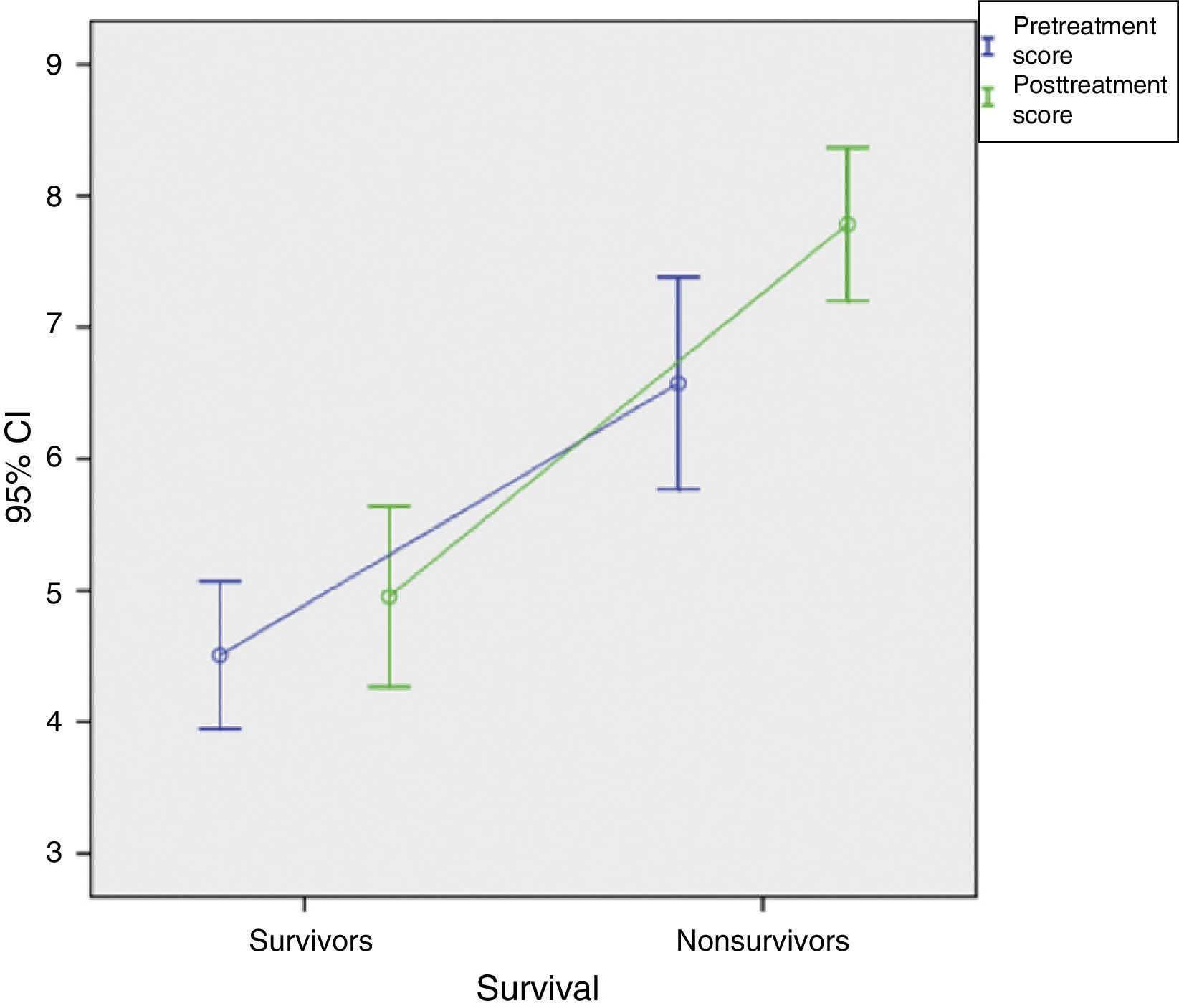
The comparison of the values that relate the pretreatment (PS1) and after treatment (PS2) results showed overall survival in patients with PS1<4.5 and PS2<4.9, whereas mortality was greater with indices of PS1>6.5 and PS2>7.7.
ConclusionsVander Poorten index can be applied in hospital areas with small numbers of parotid carcinomas. It enables a more accurate prognosis for individual patients.
La clasificación histológica de la Organización Mundial de la Salud (OMS) junto con mejores estudios de imagen aportan información relevante para el manejo de los cánceres de parótida. Sin embargo, su pronóstico depende de otros factores diferentes de la histología y la extensión tumoral. El presente trabajo valora la utilidad de la clasificación pronóstica de Vander Poorten creada en 1999 de los cánceres parotídeos que incluye todos estos factores en los pacientes de nuestro medio.
Mèc)todosSeguimiento de 19 pacientes con carcinomas de parótida distintos de tumores linfoideos o metástasis intraparotídeas entre los años 1998 y 2012. Se obtuvo su índice pronóstico a partir de las fórmulas propuestas por Vander Poorten, que incluyen los factores de edad, tamaño tumoral, afectación ganglionar, invasión cutánea, afectación del nervio facial, crecimiento perineural y márgenes de resección, antes de la cirugía (PS1) y despuèc)s (PS2). Se relacionó la supervivencia global a los 5 años de cada paciente a partir de su inclusión en alguno de los 4 grupos de riesgo definidos.
ResultadosLa estratificación de riesgo de Vander Poorten según los resultados PS2 se distribuyó en grupos de riesgo (GR) 1 (3 pacientes, 15,7%), 2 (5 pacientes, 26,3%), 3 (un paciente, 5,8%) y 4 (10 pacientes, 52,2%). Los 6 pacientes que fallecieron durante el seguimiento pertenecían al GR4. De los 4 supervivientes del GR4 solo uno ha superado el seguimiento de 5 años.
La comparación de las medias que relacionan las variables de resultado pretratamiento (PS1) y postratamiento (PS2) mostró una mejor supervivencia global en los pacientes con valores de PS1<4,5 y PS2<4,9, mientras que la mortalidad fue mayor a partir de los índices de PS1>6,5 y PS2>7,7.
ConclusionesEl índice de Vander Poorten es aplicable en áreas hospitalarias con escaso número de carcinomas de parótida. Permite establecer un pronóstico de supervivencia más certero sobre pacientes individuales.
Malignant tumors of the parotid gland are characterized by a low incidence (1•3% of all head and neck cancers) and a marked histopathological heterogeneity.1 Approximately 70% of the malignant tumors of the major salivary glands are located in the parotid glands.2
Initially, the diagnosis is clinical, and requires fine-needle aspiration biopsy (FNAB) to determine the nature of the tumor. Computed tomography (CT) and magnetic resonance imaging (MRI) are key elements in the anatomical study, preoperative evaluation and determination of the extension.3
The treatment of choice is always parotidectomy, with preservation of the facial nerve whenever possible.4,5 The need for radiotherapy,6 chemotherapy or cervical lymph node dissection will depend on the stage, aggressiveness and histological type of the tumor.
At the present time, there is no standardized approach to the management of cancer of the major salivary glands because of the many subtypes, each with a unique molecular background and variable clinical behavior.7 Even so, locoregional control of the cancer is satisfactory and the most common cause of treatment failure is the development of distant metastasis.8 Although the control of the disease continues to be variable, it would be possible to predict the prognosis in individual patients using multivariate analysis. The ability to predict the prognosis in these cancers would make it possible to know what course the disease will take.
The risk stratification model proposed by Vander Poorten et al.9 as a predictive index could prove to be useful, as it interrelates many of the variables that influence prognosis and survival in patients with parotid carcinomas: age at diagnosis, tumor size, lymph node involvement, skin invasion, facial nerve involvement, perineural growth and resection margins. In this approach, all these factors are examined before and after the proposed treatment.
MethodsFor this study, we chose to use the prognostic index devised by Vander Poorten et al.,4,9 which establishes 2 numerical values to estimate the probability of survival according to the results of the formulas, expressed as the prognostic score (PS) before treatment (PS1) and afterwards (PS2).
In this case, we divided the results into 4 groups, going from lower risk to higher based on the posttreatment scoring system described by Vander Poorten et al.4,9 in their original study: risk group [RG]1: <3.99; RG2: 3.99•4.80; RG3: 4.81•5.67 and RG4: >5.67. In accordance with the data obtained, the numerical result was used to establish the prediction for the population-based overall survival in our regional health area among patients diagnosed from 1998 to 2012 and having undergone a maximum follow-up of 5 years. We also compared the mean scores obtained with the Vander Poorten index to relate the outcome variables, PS1 and PS2, to overall survival.
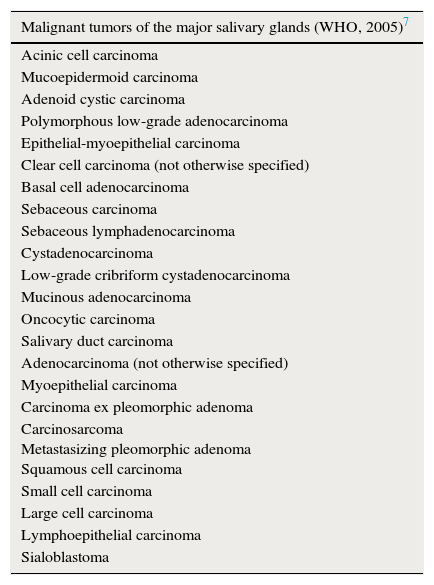
We conducted a retrospective cross-sectional study involving the patients in the area covered by our hospital (population 551,856) who had been diagnosed with any of the malignant parotid tumors included in the 2005 classification of the World Health Organization (WHO)7 (Table 1) and had undergone surgery, surgery plus radiotherapy, or surgery plus radiotherapy and chemotherapy. The patients also had to have undergone proper clinical staging according to the 2010 TNM classification of the American Joint Committee on Cancer (AJCC), where T refers to the size of the lesion, N to the existence of cervical lymph node metastases and M to distant metastases. We excluded patients with malignant tumors of the major salivary glands not located in the parotid gland, with malignant parotid tumors not included in the 2005 WHO classification (Table 1) or with nonepithelial parotid metastases, as well as those who did not meet the inclusion criteria.
Malignant tumors of the major salivary glands.
| Malignant tumors of the major salivary glands (WHO, 2005)7 |
|---|
| Acinic cell carcinoma |
| Mucoepidermoid carcinoma |
| Adenoid cystic carcinoma |
| Polymorphous low-grade adenocarcinoma |
| Epithelial-myoepithelial carcinoma |
| Clear cell carcinoma (not otherwise specified) |
| Basal cell adenocarcinoma |
| Sebaceous carcinoma |
| Sebaceous lymphadenocarcinoma |
| Cystadenocarcinoma |
| Low-grade cribriform cystadenocarcinoma |
| Mucinous adenocarcinoma |
| Oncocytic carcinoma |
| Salivary duct carcinoma |
| Adenocarcinoma (not otherwise specified) |
| Myoepithelial carcinoma |
| Carcinoma ex pleomorphic adenoma |
| Carcinosarcoma Metastasizing pleomorphic adenoma Squamous cell carcinoma |
| Small cell carcinoma |
| Large cell carcinoma |
| Lymphoepithelial carcinoma |
| Sialoblastoma |
Malignant tumors of the major salivary glands, updated by the World Health Organization (WHO) in 2005.
The patients with parotid carcinomas diagnosed from 1998 to 2012 were identified by searching the database of the pathology department of our hospital (Microsoft Excel). The clinical review was carried out using electronic information systems and electronic health records (Medicx, Medicx 3 and Diraya), and resorting to the manual review of the medical records in specific cases.
The statistical analysis for the descriptive study and multivariate comparison of arithmetic means was performed with the Statistical Package for the Social Sciences (SPSS) software. For the statistically significant variables, both the hazard ratio and its 95% confidence interval were determined, with a p value<0.05.
The prognostic score for each patient was calculated in accordance with the Vander Poorten indices.4,9 The PS1 prognostic score corresponded to the preoperative values and PS2 to the postoperative findings (Table 2).
Vander Poorten prognostic indices.
| PS1: 0.024A+0.62P+0.44T+0.45N+0.63S+0.91F |
| PS2: 0.018A+0.39T+0.34N+0.7S+0.56F+0.78PG+0.65PM |
The prognostic index of Vander Poorten et al.,4,9 calculated according to the pretreatment (PS1) and posttreatment (PS2) scores, depends on patient age, pain, TNM classification, skin invasion, facial nerve dysfunction, perineural invasion and surgical margin status.
A: age; F: facial nerve dysfunction; N: clinical N classification; P: pain at presentation; PG: perineural invasion; PM: surgical margins; S: skin invasion; T: clinical T classification.
Of the 30 cases of malignant parotid tumor recorded in our hospital from 1998 to 2012, we included the 19 patients who had had carcinomas, excluding 6 lymphoid tumors and 5 parotid metastases.
The age range at diagnosis was 20•84 years, with a mean age of 61.7 years and a standard deviation of 16.8. Eleven of the 19 patients were men.
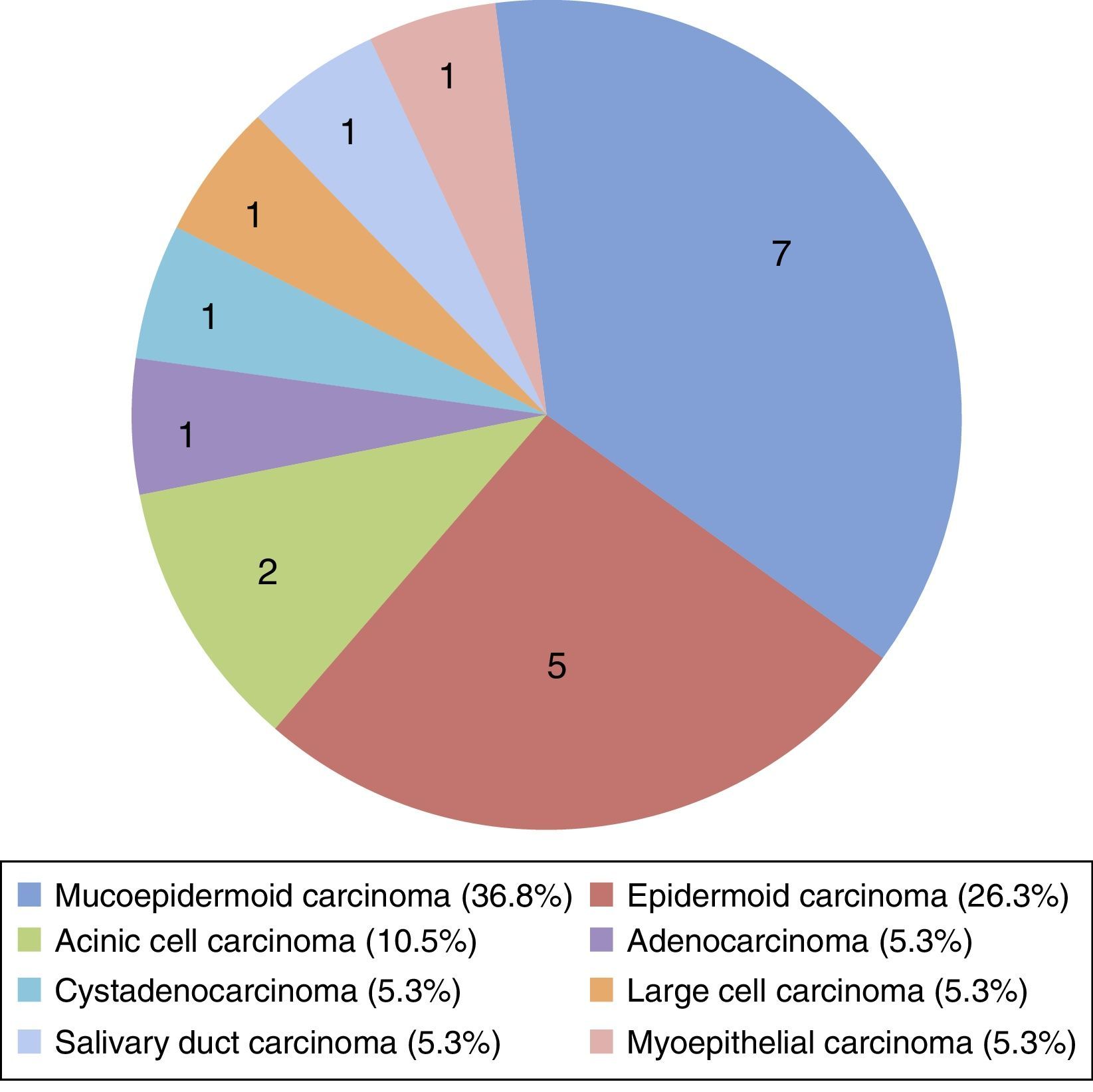
When the cancers were grouped according to the histological classification of malignant major salivary gland tumors (WHO, 2005),7 there was a predominance of mucoepidermoid carcinomas (36.8%) and of epidermoid carcinomas (26.3%), which was surprising, as the latter are uncommon in our patient population (Fig. 1).

At the time of diagnosis, pain was recorded in 6 patients (31.6%), 42.1% presented with skin evasion, 4 patients (21.05%) reported some degree of facial paresis or paralysis prior to surgery and surgical margin involvement was observed in 11 (57.8%).
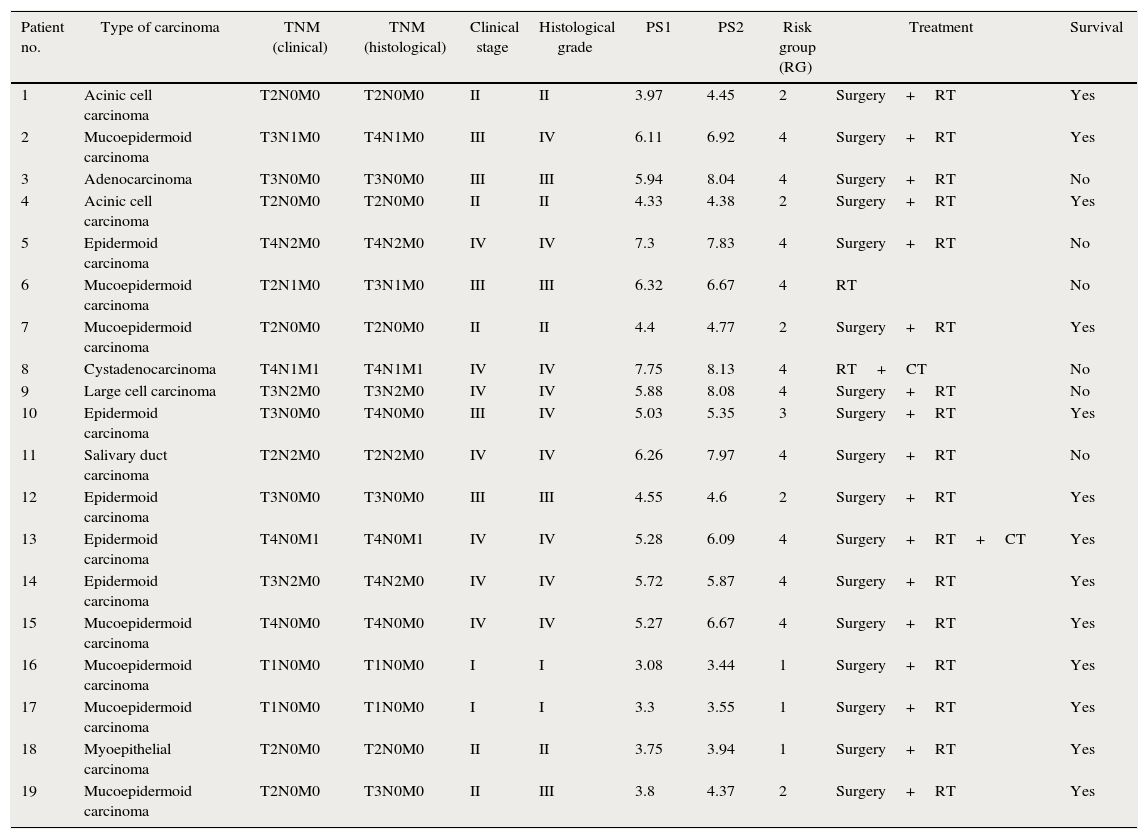
The distribution according to the 2010 TNM classification of the AJCC differed depending on whether it was clinical or histopathological (Table 3). According to clinical TNM staging, 2 patients (10.5%) were T1, 7 (36.8%) T2, 6 (31.5%) T3 and 4 (21.2%) T4. In 12 cases (61.5%), there were no lateral cervical lymph node metastases (N0); 3 patients (15.7%) were N1 and 4 (21.2%) were N2). Distant metastases were recorded in 2 patients (10.5%). In the pathological TNM, 2 patients (10.5%) were T1, 5 (26.35%) T2, 5 (26.35%) T3 and 7 (36.8%) T4. Twelve patients (61.5%) were N0, 3 (15.7%) were N1 and 4 (21.2%) were N2. Distant metastases were found in 2 patients (10.5%).
Classification, outcome and characteristics of the study patients.
| Patient no. | Type of carcinoma | TNM (clinical) | TNM (histological) | Clinical stage | Histological grade | PS1 | PS2 | Risk group (RG) | Treatment | Survival |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Acinic cell carcinoma | T2N0M0 | T2N0M0 | II | II | 3.97 | 4.45 | 2 | Surgery+RT | Yes |
| 2 | Mucoepidermoid carcinoma | T3N1M0 | T4N1M0 | III | IV | 6.11 | 6.92 | 4 | Surgery+RT | Yes |
| 3 | Adenocarcinoma | T3N0M0 | T3N0M0 | III | III | 5.94 | 8.04 | 4 | Surgery+RT | No |
| 4 | Acinic cell carcinoma | T2N0M0 | T2N0M0 | II | II | 4.33 | 4.38 | 2 | Surgery+RT | Yes |
| 5 | Epidermoid carcinoma | T4N2M0 | T4N2M0 | IV | IV | 7.3 | 7.83 | 4 | Surgery+RT | No |
| 6 | Mucoepidermoid carcinoma | T2N1M0 | T3N1M0 | III | III | 6.32 | 6.67 | 4 | RT | No |
| 7 | Mucoepidermoid carcinoma | T2N0M0 | T2N0M0 | II | II | 4.4 | 4.77 | 2 | Surgery+RT | Yes |
| 8 | Cystadenocarcinoma | T4N1M1 | T4N1M1 | IV | IV | 7.75 | 8.13 | 4 | RT+CT | No |
| 9 | Large cell carcinoma | T3N2M0 | T3N2M0 | IV | IV | 5.88 | 8.08 | 4 | Surgery+RT | No |
| 10 | Epidermoid carcinoma | T3N0M0 | T4N0M0 | III | IV | 5.03 | 5.35 | 3 | Surgery+RT | Yes |
| 11 | Salivary duct carcinoma | T2N2M0 | T2N2M0 | IV | IV | 6.26 | 7.97 | 4 | Surgery+RT | No |
| 12 | Epidermoid carcinoma | T3N0M0 | T3N0M0 | III | III | 4.55 | 4.6 | 2 | Surgery+RT | Yes |
| 13 | Epidermoid carcinoma | T4N0M1 | T4N0M1 | IV | IV | 5.28 | 6.09 | 4 | Surgery+RT+CT | Yes |
| 14 | Epidermoid carcinoma | T3N2M0 | T4N2M0 | IV | IV | 5.72 | 5.87 | 4 | Surgery+RT | Yes |
| 15 | Mucoepidermoid carcinoma | T4N0M0 | T4N0M0 | IV | IV | 5.27 | 6.67 | 4 | Surgery+RT | Yes |
| 16 | Mucoepidermoid carcinoma | T1N0M0 | T1N0M0 | I | I | 3.08 | 3.44 | 1 | Surgery+RT | Yes |
| 17 | Mucoepidermoid carcinoma | T1N0M0 | T1N0M0 | I | I | 3.3 | 3.55 | 1 | Surgery+RT | Yes |
| 18 | Myoepithelial carcinoma | T2N0M0 | T2N0M0 | II | II | 3.75 | 3.94 | 1 | Surgery+RT | Yes |
| 19 | Mucoepidermoid carcinoma | T2N0M0 | T3N0M0 | II | III | 3.8 | 4.37 | 2 | Surgery+RT | Yes |
CT: chemotherapy; RT: radiotherapy.
A total of 17 patients (89.5%) underwent total or partial parotidectomy and adjuvant radiotherapy (Table 3) with curative intent; 6 of them (35.2%) had some type of postoperative facial nerve dysfunction. At the time of writing, 1 patient (5.8%) was receiving palliative treatment with chemotherapy due to inoperable disease recurrence. The 2 patients (10.5%) who had not undergone either surgical treatment or radiotherapy were treated with radiation and chemotherapy with palliative intent (Table 3).
The overall 5-year survival rate was 60% (only 15 of the 19 carcinomas were taken into account, as 4 of the 13 survivors had not yet completed 5 years of follow-up at the time of writing). Histological grades 1 and 2 were associated with 100% survival and grades 3 and 4 with a rate of 33%.
The distribution among the risk group (RG) defined by the PS2 scores (Table 3) were as follows: RG1, 3 patients (15.7%); RG2, 5 patients (26.3%); RG3, 1 patient (5.8%); and RG4, 10 patients (52.2%) (Fig. 2). The 6 deaths corresponded to RG4 (100%).
. Bar graph showing the distribution of the patients according to the risk group to which they belonged, expressed as percentages.")
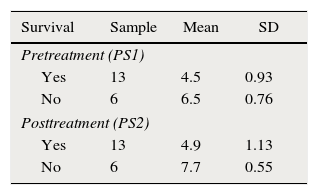
The data of the 19 patients were introduced into the formulas provided for the Vander Poorten index,4,9 and the mean scores were compared to enable us to relate the pretreatment outcome variables (PS1) and the posttreatment findings (PS2) to patient survival. We found that there were differences in the survival rate that favored those patients with PS1<4.5 and PS2<4.9 over those with PS1>6.5 and PS2>7.7 (Table 4). Moreover, there was a linear correlation between the results (Fig. 3), since the patients with the lowest scores survived, whereas an increase in the score was accompanied by a higher mortality rate.
Results applied to Vander Poorten prognostic indices.
| Survival | Sample | Mean | SD |
|---|---|---|---|
| Pretreatment (PS1) | |||
| Yes | 13 | 4.5 | 0.93 |
| No | 6 | 6.5 | 0.76 |
| Posttreatment (PS2) | |||
| Yes | 13 | 4.9 | 1.13 |
| No | 6 | 7.7 | 0.55 |
The application of the Vander Poorten indices enabled the calculation of the pretreatment (PS1) and posttreatment (PS2) scores. The table shows the relationship between the mean scores and survival.
PS: prognostic score; SD: standard deviation.

In 1991, Frankenthaler et al.10 conducted studies on the prognosis of malignant parotid tumors. They carried out a retrospective analysis of 178 patients, 59.9% of whom had been treated surgically, and the remaining 40.1% had undergone surgery and radiotherapy. The mean follow-up was 7.5 years from the time of diagnosis. They concluded that the prognosis depended on the tumor stage, tumor grade, histological type, lymph node and perineural invasion, tumor size, extension beyond the parotid fascia, resection margin status, patient age and the presence of metastases. On the basis of that study, measures were proposed for the analysis of the optimal surgical procedure and the reasons for choosing combined treatment. Hocwald et al.11 established the prognostic factors for major salivary gland carcinomas and determined the 5-year survival in a retrospective study of 78 patients. All of the patients had been treated surgically, regardless of the tumor type; 56% had also received radiotherapy and 13%, chemotherapy. The 5-year disease-free survival was 65%. On the examination of the clinical and histopathological outcomes, they observed that the presence of cervical lymph node metastases and perineural invasion were factors indicative of poor prognosis, independent of the survival. They suggested that adjuvant chemotherapy and radiotherapy may improve survival. In their study, “Prognostic indicators for malignant tumors of the parotid gland”,12 Harbo et al. established a prognostic relationship between the tumors, their stage and the histological classification. They carried out a retrospective study in a sample of 152 patients with parotid carcinomas, measuring the overall survival 5 years after the diagnosis of the disease (50%). They found statistically significant differences in survival depending on the stage, favoring those patients in whom the disease was less advanced, with a survival rate of 65% in stage I and of 50% in stage II, whereas in stage IV, it was reduced to 9%. The prognosis for survival in histologically well differentiated tumors (52%) was also better than that associated with poorly differentiated lesions (19%). The authors concluded that the TNM system was a good predictor of the results of treatment and that the use of a combination of clinical and histological factors would aid in the design of treatment strategies. In 2005, members of the department of otorhinolaryngology of Hospital Gregorio Marañón in Madrid, Spain, conducted a study13 of the outcomes of the diagnosis and treatment of parotid cancer in their hospital between 1991 and 2002. They reported an overall 5-year survival in their patient population of 56% (60% in our series) • 68% for stages I and II and 43% for stages III and IV • and concluded that, in this disease of low incidence and high mortality, staging and histological study were highly valuable prognostic factors.
The importance of the prognostic index described by Vander Poorten et al.4,9 lies in the combination of multiple variables including age, tumor size, perineural invasion, resection margin involvement, pain, etc. These predictive factors had never been combined to establish a given prognosis. The incorporation of a tool that related these adverse factors would improve the prediction of overall survival in patients with parotid carcinomas. The prognostic score (PS) classified patients according to 4 subgroups ranging from lower to higher risk. In the subgroups formed on the basis of the postoperative prognostic score, the 5-year disease-free survival rate ranged between 95% (RG1) and 42% (RG4). Thus, the Vander Poorten prognostic score4,9 provided a system for grouping variables as an aid in the treatment and the prediction for survival of patients with parotid carcinomas. The study of Takahama et al.14 compared the prognostic scores and risk stratification of Vander Poorten et al.4,9 with those of Carrillo et al.15 The authors pointed out that proponents tend to confirm the validity of their own models, but that other researchers are less successful in doing so. Takahama et al.14 found that the group of Carrillo et al. was more similar to theirs, and concluded that the scores calculated with the system of Carrillo et al. generated more distinct survival curves, although the determination of the groups with a more favorable prognosis was not easy with either of these scoring systems. Therefore, the results were not totally reproducible in their group of patients.
The findings of our study fit the prognoses resulting from the trial reported by Vander Poorten et al.4,9 Although we are aware of the statistical limitations inherent in a small sample (19 patients), when our results were stratified according to subgroup, we observed that all 6 (100%) of the patients who had died belonged to RG4 (PS>5.67), and that there may be more deaths in that group, as 3 of the remaining 4 patients had not yet completed 5 years of follow-up at the time of writing.
A study of the comparison of the means yielded a mathematical relationship that showed that those patients with a PS1<4.5 or a PS2<4.9 have greater probabilities of survival that those with a PS1>6.5 or a PS2>7.7, either of which considerably reduces their life expectancy. Although this is merely a numerical datum in a small sample size, these results could be taken into account in the evaluation of survival rates.
Our sample group fits description of the clinical and histopathological characteristics of malignant parotid tumors, as well as the distribution by sex and age, the TNM and the treatment received.
The key point that determines a poor prognosis for patient outcome according to Vander Poorten et al.9 is recurrence of the disease at 5 years of survival. Of the 19 patients in our study, 6 died; of the latter group, only 1 was still alive 5 years after being diagnosed. For this reason, we have considered the factor “death” as a key point of our study, taking into account the fact that all of the deaths were due to the patient's cancer.
ConclusionsDespite the heterogeneity of parotid cancer in terms of the histological features and risk factors, the Vander Poorten index enables the accurate risk stratification, according to individual prognoses, of parotid cancer patients in hospitals located in health areas with a low incidence or that are not referral centers for the management of this disease.
Studies need to be carried out with a sufficient number of patients to validate our finding that the comparison of the mean scores corresponding to PS1 and PS2 enabled us to make finer distinctions when using the Vander Poorten prognostic index.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors declare they have no conflicts of interest.
Please cite this article as: Maza-Solano JM, Sánchez-Gómez S, Herrero-Salado T, Benavente-Bermudo G, Ventura-Díaz J, de Mingo Fernández EJ. Clasificación pronóstica de los tumores malignos de glándula parótida. Rev Esp Cir Oral Maxilofac. 2015. http://dx.doi.org/10.1016/j.maxilo.2015.01.005
