



To determine the influence of the pre-operative cognitive impairment on results of the total knee arthroplasty according to a doctor and patient perspective.
Materials and methodsA prospective study was conducted on patients from the surgical waiting list who had undergone a primary total knee arthroplasty. The sample initially included 265 patients, but 50 were subsequently excluded. Cognitive impairment was assessed pre-operatively by the Mini Cognitive Examination (MEC-35). The Visual Analog Scale (VAS), the Knee Society Score (KSS), the Western Ontario and McMaster Osteoarthritis Index (WOMAC), and the Hospital Anxiety and Depression Scale (HADS) were used pre-operatively and one year later post-operatively.
ResultsA total of 215 patients were assessed (57 men and 158 women). Cognitive impairment had no influence on the results of total knee arthroplasty. In fact, there was no statistical significance in any of the scales analyzed. Preoperatively, and one year later, the patients with cognitive impairment showed higher levels of anxiety and depression, with these differences being statistically significant.
DiscussionAll of the patients experienced an improvement in the specific outcomes and quality of life after the total knee arthroplasty procedure, regardless of the presence of preoperative cognitive impairment.
Determinar la influencia del deterioro cognitivo preoperatorio en los resultados de la artroplastia total de rodilla, no solo desde la perspectiva del médico sino también del paciente.
Material y métodoEstudio prospectivo de pacientes procedentes de la lista de espera quirúrgica, sometidos a artroplastia total de rodilla primaria. De los 265 pacientes de la muestra inicial, 50 fueron excluidos. El deterioro cognitivo fue valorado preoperatoriamente mediante el Mini Examen Cognoscitivo (MEC-35). Tanto preoperatoriamente como al año postoperatorio se utilizó la Escala Analógica Visual (EVA), la Knee Society Score (KSS), el Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), y el Hospital Anxiety and Depression Scale (HADS).
ResultadosSe analizaron 215 pacientes (57 varones y 158 mujeres). El deterioro cognitivo no influyó en los resultados de la artroplastia total de rodilla, no alcanzando significación estadística en ninguna de las escalas analizadas. Los pacientes con deterioro cognitivo presentaron niveles más elevados de ansiedad y depresión, preoperatoriamente, y al año de intervención, siendo estas diferencias estadísticamente significativas.
DiscusiónTodos los pacientes experimentaron una mejoría de los resultados tanto específicos como de calidad de vida tras un procedimiento como la artroplastia total de rodilla independientemente de la presencia de deterioro cognitivo preoperatorio.
Population aging has led to an increase in the prevalence of chronic degenerative diseases like osteoarthritis (or arthrosis), with the knee being one of the most widely studied areas. The impact of this disease goes beyond physical disability, affecting the social, psychological and work environments of patients. These aspects comprise what we know as health-related quality of life (HRQoL).
Knee joint replacement surgery has become increasingly common as an effective procedure to improve quality of life. The assessment of its results requires the use of specific questionnaires,1 which have demonstrated that this technique offers notable benefits for octogenarian patients.2–5
The Knee Society Score (KSS)6,7 includes 2 subscales: the function subscale, which collects information provided by the patient, and the subscale for the knee itself, which collects data provided by the physician. In addition to parameters measuring the performance of the prosthesis, it provides an assessment centered on the point of view of the physician, which does not always coincide with that of the patient.
The use of instruments that assess quality of life is necessary in any current clinical research project. The adequacy of using a double scoring system – KSS and Western Ontario And McMaster Universities Osteoarthritis Index (WOMAC)8–10 – is based on the need to obtain an assessment of the results from the perspective of both the physician and the patient.
The search for tools which predict the results of total knee arthroplasty (TKA) has led to studying biological parameters, such as age and gender, physical parameters, like the body mass index (BMI), and psychological factors, like distress. Nevertheless, cognitive impairment related to natural human aging has remained scarcely studied.
There are some studies11–13 on cognitive impairment in the immediate postoperative period, but little is known about the influence of preoperative cognitive impairment on the results of a surgical procedure.
The objective of this study was to determine whether preoperative cognitive impairment among patients undergoing TKA affected the functional and quality of life results following the procedure.
Materials and methodsWe conducted a longitudinal, observational, prospective, follow-up study of a cohort of patients undergoing primary TKA, obtained from the surgery waiting list of Ciudad Real General Hospital, over the period between October 2004 and July 2007. We obtained an initial cohort of 265 patients.
The study was approved by the Ethics Committee of the hospital and patients completed an informed consent form prior to their voluntary inclusion in the project.
Study populationAll patients were implanted a Duracon® (Stryker, Kalamazoo, MI, USA) total knee prosthesis. The exclusion criteria for the study were: age equal to or under 65 years (45 cases); severe psychiatric disorder (0 cases); reinterventions or fractures in the same limb during the follow-up period (2 cases); and death (3 cases). None of the deaths were related to the procedure being studied.
Patients with bilateral arthroplasty had covered a period of at least 12 months between both procedures, thus being considered as different patients.
Data collectionPatients were assessed preoperatively and 1 year after the intervention. The preoperative assessment collected epidemiological data (age, gender, weight, size), diagnosis, laterality, and comorbidities.
In each of the assessments, patients completed the following questionnaires:
- 1.
Mini-Examen Cognoscitivo (MEC-35),14 a version of the Mini Mental State Examination by Folstein15 adapted to Spanish to detect patients with cognitive impairment. It considers as cases scores of 23 or less among patients aged over 65 years. None of the patients presented a score under 10, which is considered as severe dementia.
- 2.
Hospital Anxiety and Depression Scale (HADS),16 a scale for the self-assessment of anxiety and depression which detects states of anxiety and depression in non-psychiatric hospital outpatient consultation services. It includes 2 subscales with 7 questions each. Each item is assessed through a Likert-type response scale with 4 points (range 0–3), thus configuring values between 0 and 21 for each subscale. The score is interpreted according to the following criteria: 0–7 (range of normality), 8–10 (probable or doubtful case), and 11–21 (case of anxiety or depression).
- 3.
Analog Visual Scale (VAS) to assess the subjective intensity of pain. It measures the perception of pain using a continuous, horizontal, straight, 10-cm line, in which the left end “0cm” represents “no pain”, and the right end “10cm” represents “the worst pain imaginable”.
- 4.
Knee Society Score6,7, with its 2 subscales (knee and function), to assess the specific results of the total knee prosthesis, mainly from the perspective of the physician. The 2 subscales are assessed separately, with the maximum score being 100 points for each of them. The higher the score, the better the functional result.
- 5.
WOMAC8–10 self-administered questionnaire, specific to the hip and knee, to assess quality of life. It is comprised by 24 questions grouped into 3 domains, of which 5 measure pain, 2 measure joint rigidity and 17 assess the difficulty to carry out everyday physical activities. The responses to each question range between 0 for “none” and 4 for “extreme”, and the total score may range between 0 and 96 points. Lower scores correspond to a better quality of life.
- 6.
Level of satisfaction with the result of the intervention, which was asked of patients during the annual review, and was categorized into poor, average, good and very good.
We assessed the normality of quantitative variables through the Kolmogorov-Smirnov test. The descriptive analysis of qualitative variables was defined through distribution frequency tables and sector graphs. Quantitative variables were studied through central tendency statistics (mean, mode, median), dispersion (standard deviation) and graphic representation of histograms.
For the inferential analysis we used comparison of means through the Student's t test.
We considered statistically significant differences with values of P<.05.
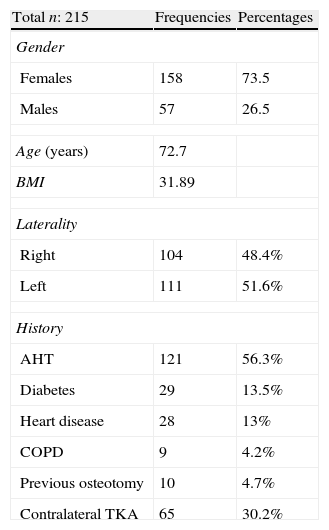
ResultsAs previously mentioned, we excluded 50 cases out of an initial cohort of 265 patients. The final sample analyzed was of 215 patients. In total, 71% of the samples were females and 29% were males. The mean age was 71.52 years and the mean BMI was 31.81. A total of 14.5% of patients lived alone, either at home or in a care residence, 44.5% lived with their families and 41% lived only with their spouse (Table 1).
Main clinical characteristics.
| Total n: 215 | Frequencies | Percentages |
| Gender | ||
| Females | 158 | 73.5 |
| Males | 57 | 26.5 |
| Age (years) | 72.7 | |
| BMI | 31.89 | |
| Laterality | ||
| Right | 104 | 48.4% |
| Left | 111 | 51.6% |
| History | ||
| AHT | 121 | 56.3% |
| Diabetes | 29 | 13.5% |
| Heart disease | 28 | 13% |
| COPD | 9 | 4.2% |
| Previous osteotomy | 10 | 4.7% |
| Contralateral TKA | 65 | 30.2% |
AHT: arterial hypertension; BMI: Body mass index; COPD: chronic obstructive pulmonary disease; TKA: total knee arthroplasty.
Out of the 215 patients in the sample, 43 (20%) presented preoperative cognitive impairment, whilst 172 (80%) did not. The mean score obtained in the MEC-35 was 26.44 points and the standard deviation was 4.02.
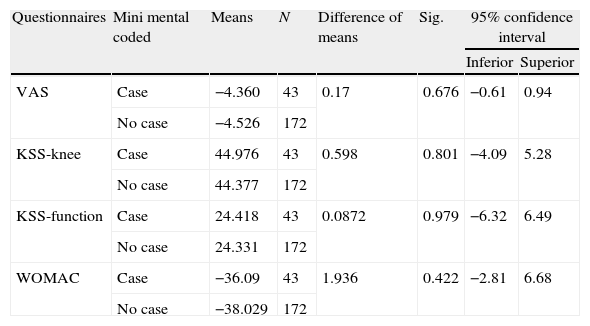
The differences in mean scores (annual minus preoperative) in the various scales, VAS, KSS-knee, KSS-function and WOMAC, were very similar in both groups, with and without cognitive impairment (Table 2).
Difference in mean scores (annual minus preoperative) in the different scales. Analysis of the differences of means of the various questionnaires and their connection with the presence of cognitive impairment.
| Questionnaires | Mini mental coded | Means | N | Difference of means | Sig. | 95% confidence interval | |
| Inferior | Superior | ||||||
| VAS | Case | −4.360 | 43 | 0.17 | 0.676 | −0.61 | 0.94 |
| No case | −4.526 | 172 | |||||
| KSS-knee | Case | 44.976 | 43 | 0.598 | 0.801 | −4.09 | 5.28 |
| No case | 44.377 | 172 | |||||
| KSS-function | Case | 24.418 | 43 | 0.0872 | 0.979 | −6.32 | 6.49 |
| No case | 24.331 | 172 | |||||
| WOMAC | Case | −36.09 | 43 | 1.936 | 0.422 | −2.81 | 6.68 |
| No case | −38.029 | 172 | |||||
KSS: Knee Society Score; Sig: statistical significance; VAS: analog visual scale; WOMAC: Western Ontario McMaster Universities Osteoarthritis Index.
We analyzed the differences between the mean results of the various questionnaires and the relationship with the presence of cognitive impairment using the Student's t test for independent samples and did not obtain statistically significant differences: VAS P=.676; KSS-knee P=.801; KSS-function P=.979; WOMAC P=.422 (Table 2).
Out of the 43 patients with cognitive impairment, 79.1% reported a good or very good result after surgery (24 good and 10 very good). In the group without cognitive impairment, 82.6% considered the result as good or very good (82 good and 60 very good), with these results being notably superior but not statistically significant.
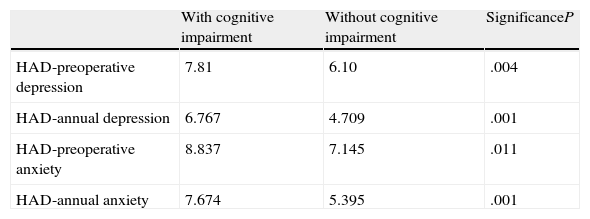
Patients with cognitive impairment presented mean scores of 8.83 for preoperative anxiety and 7.81 for preoperative depression. These scores were higher than those obtained by patients without cognitive impairment, which were 7.14 and 6.10, respectively. The mean scores for anxiety and depression 1 year after the intervention improved in both groups but were also higher among patients with cognitive impairment (7.67 and 6.76) than among the group without cognitive impairment (5.39 and 4.70). The statistical analysis through the Student's t test for comparison of means (Table 3) showed that differences in the levels of anxiety and depression between both groups, with and without cognitive impairment, were statistically significant.
Differences in the levels of anxiety and depression between both groups, with and without cognitive impairment.
| With cognitive impairment | Without cognitive impairment | SignificanceP | |
| HAD-preoperative depression | 7.81 | 6.10 | .004 |
| HAD-annual depression | 6.767 | 4.709 | .001 |
| HAD-preoperative anxiety | 8.837 | 7.145 | .011 |
| HAD-annual anxiety | 7.674 | 5.395 | .001 |
HAD: hospital anxiety and depression; P: statistically significant (P<.05).
Knee arthroplasty has been proven effective to improve quality of life, even in octogenarian patients,2–5 and this improvement is achieved both among those who suffer cognitive impairment in the preoperative period and those who do not.
The assessment of results in any study requires the use of specific questionnaires1; however, the literature features a scarce use of cognitive tests in works where a coherent response by patients should be considered essential to avoid introducing bias. Mental health is increasingly more relevant, due to its influence on the results of studies on surgical techniques in general, and prosthetic surgery in particular.17–19 Gandhi20 reported that patients with lower mental health scores had a higher probability of being unsatisfied with the results and, for Serra-Sutton,21 low baseline perceived mental health scores were associated to worse quality of life scores, assessed by the WOMAC index.
In the present study, patients with cognitive impairment also presented lower satisfaction, although the differences were not statistically significant and, as in the work by Gandhi,20 an improvement in mental health scores was observed 1 year after the intervention.
Different works have studied the influence of aspects, such as age, anesthetic technique and surgical procedures, on the development of cognitive impairment in the postoperative period,11–13 but little is known about the influence which this cognitive impairment could have as a predictive factor of the results when patients present it in the preoperative period. Ritter22 analyzed the evolution of 13 arthroplasties on patients with dementia and observed an increase in the number of complications, particularly disorientation, although both patients and their relatives reported a high level of satisfaction.
In the present study, the analysis of the influence of preoperative cognitive impairment on the results found that it did not affect the specific results of the total knee prosthesis, as assessed using the KSS, and that patients with cognitive impairment presented similar quality of life results, as assessed using the WOMAC index, to those of patients who did not suffer cognitive impairment. Van Dijk23 also observed that joint mobility and pain were factors with a decisive influence on the limitations of activity in patients with knee and hip osteoarthritis, whereas cognitive impairment played a less relevant role.
We also observed that the levels of anxiety and depression, as measured using the HADS tool, were higher among the group of patients with preoperative cognitive impairment, and that these differences were statistically significant. The analysis of this result indicates that the high prevalence of depressive symptoms among patients aged over 64 years,24 coupled to the increase in joint diagnosis of depression-dementia after the age of 80,25 has led to a confusion factor when these two conditions are studied together. This close relationship between depression and cognitive impairment was studied by Apostolos26 through biological-structural neuroimaging techniques. This author established that both pathologies shared common cortical and subcortical areas of the brain. Moreover, he also observed a decrease in the levels of anxiety and depression in the review conducted 1 year after the TKA, with statistically significant differences. In a study including knee and hip arthroplasties, Duivenvoorden27 obtained similar results after 12 months, adding a lower satisfaction index among patients with preoperative anxiety and depression.
The design of this study only enables us to refer to levels of anxiety and depression, rather than clinical diagnoses. Therefore, even though we consider the improvement interesting, we can only draw conclusions in those terms. Other limitations include not assessing cognitive impairment 1 year after the intervention and not carrying out a stratification into mild, moderate and severe (dementia), although, as indicated in ‘Material and methods’ section, none of the patients included in the series obtained a score under 10 points in the MEC-35, which means that none of the cases in the series suffered dementia. The fact that the differences in the scales studied between both groups were limited, coupled to the low number of patients with cognitive development (20%), has a negative impact on the statistical power. It would be necessary to conduct further works which addressed these limitations in order to affirm that cognitive impairment should not be a contraindication for prosthetic joint replacement.
ConclusionsCognitive impairment does not have an influence on the functional and quality of life results of patients undergoing TKA.
Patients suffering cognitive impairment present higher levels of anxiety and depression than those who do not suffer it, both preoperatively and 1 year after the intervention.
Level of evidenceLevel of evidence II.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation did not require experiments on humans or animals.
Confidentiality of dataThe authors declare that they have followed the protocols of their workplace on the publication of patient data.
Right to privacy and informed consentThe authors declare having obtained written informed consent from patients and/or subjects referred to in the work. This document is held by the corresponding author.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Jiménez M, Zorrilla P, López-Alonso A, León A, Salido J. ¿Influye el deterioro cognitivo preoperatorio en los resultados de la artroplastia total de rodilla?. Rev Esp Cir Ortop Traumatol. 2014;58:364–369.
