






As long as the neuromuscular stabilizers are intact, a lesion of the scapholunate ligament may or may not progress to a carpal instability. The mechanisms by which the muscles compensate this defect are not very well known. We designed an experimental study with the aim of clarifying these mechanisms.
Material and methodUsing 10 fresh wrists, with no pre-existing lesions, we studied the movements of the scaphoid, triquetrum and capitate produced by the isometrical loading of the muscles which move the wrist, each of them isolated or combined, before and after cutting off the scapholunate ligaments. To do this, we placed sensors in each of these bones and used the Fastrack® system to record these movements.
ResultsThe simultaneous loading of the muscles of the wrist produce rotational movements in flexion and supination of the proximal carpal row. After cutting off the scapholunate ligaments, the scaphoid rotates in pronation and flexion, while the triquetrum rotates in pronation and extension. In this situation of a scapholunate lesion, the muscles that worsen the carpal dexasation are the extensor carpi ulnaris and flexor carpi ulnaris. On the other hand, the isolated loading of the radial muscles reduces the scapholunate diastasis, thus improving the carpal alignment.
ConclusionIn dynamic scapholunate instabilities, isometric contraction of the ulnar carpal muscles must be avoided, as it promotes the scapholunate diastasis. The rest of the muscles have the opposite effect, stabilizing the carpus when primary stabilizers have failed.
Si los procesos de estabilización neuromuscular son adecuados, la lesión de los ligamentos escafolunares no siempre evoluciona hacia la desestabilización del carpo. Los mecanismos por los cuales los músculos logran compensar ese defecto son poco conocidos. Hemos diseñado un trabajo experimental encaminado a aclarar esos mecanismos.
Material y métodoEn 10 muñecas de cadáver, sin lesiones preexistentes, se han estudiado los cambios posicionales del escafoides, piramidal y hueso grande, producidos por la carga isométrica, aislada o conjunta, de los músculos motores de la muñeca, antes y después de seccionar los ligamentos escafolunares. Para ello, se han colocado sensores en la superficie de tales huesos, y se ha utilizado el sistema Fastrack® de rastreo de sensores.
ResultadosLa carga simultánea de los músculos motores de la muñeca induce a cambios rotacionales en flexión y supinación de los huesos de la hilera proximal. Tras la sección de los ligamentos escafolunares, el escafoides reacciona rotando en pronación y flexión, mientras que el piramidal prona y se extiende. En tales circunstancias, los músculos que empeoran la desaxación carpiana son el extensor carpi ulnaris y el flexor carpi ulnaris. En cambio, con la carga aislada de los músculos del lado radial, se reduce la diástasis escafolunar y mejora la alineación carpiana.
ConclusiónEn la inestabilidad escafolunar dinámica hay que evitar la contracción isométrica de los músculos cubitales del carpo, pues con ello se promueve una mayor diástasis escafolunar. Los demás músculos tienen un efecto contrario, estabilizando el carpo cuando han fracasado los estabilizadores primarios.
One of the most controversial aspects of carpal biomechanics is the so-called carpal stabilization mechanisms. When any of the elements collaborating in the stability of the wrist is altered, there may be changes in how its bone elements move (kinematic alteration) and/or in how these elements adapt to the loads traversing it (kinetic alteration). When this happens, the wrist usually tends towards widespread arthrosis, frequently associated with clinical manifestations in the form of pain, functional weakness, joint projections and creaking.1,2 Paradoxically, there are cases where the lesion in the ligament does not present with pain nor does it cause any great functional disability in the patient.3–5 Although this lack of correlation between pathology and symptoms is probably due to the presence of compensatory neuromuscular mechanisms, there is as yet no irrefutable evidence that this is the case. The present study is an attempt to advance our understanding of these secondary stabilization mechanisms of the carpus.
A lesion in the scapholunate ligament complex is the most frequent cause of carpal instability, with the potential to provoke a considerable degree of dysfunction and even seriously interfere with the activities of daily life.6 Several strategies have been proposed to avoid or detain the degenerative process, mostly aimed at re-establishing the continuity of the ligaments, and thus normalize carpal kinematics. For years, it has not been understood why some patients progress well, even without treatment, whereas others respond poorly despite having had the best possible reconstruction of their ligaments. Nowadays we know that the reconstruction of the ligaments (primary stabilization) is not sufficient and that, unless the secondary muscular stabilization mechanisms are normalized, such reconstructions are destined to failure, sooner or later.7
Since the presence of neural structures and sensorial corpuscles was demonstrated in the ligaments of the wrist, there has been speculation on the role of propioception in carpal stability.8,9 The presence of mechanoreceptors inside proves that the ligaments are functionally more complex structures than was believed.8 Apart from exercising a static primary control function in joint cohesion, they are able to provide information to the central nervous system so that it can organize the muscle responses necessary at each moment for the proper dynamic stability of the joint.10–12
Carpal stability therefore depends on adequate interaction between the form and the alignment of the joint surfaces, the tension in the ligaments and the action of the muscles controlling joint posture.11,13 The anatomical structures participating statically in the existence of a correct transmission of loads through the wrist are well known. On the other hand, we are ignorant of many of the dynamic neuromuscular mechanisms modulating this transmission. In recent years, quite a lot of work has been done to find out how muscles can stop the carpus from collapsing when there are major defects in the ligaments. In this sense, articles have been published on the effect of combined or individual contraction of certain muscles on the position and alignment of the bones in the carpus.14–17 All of the studies performed so far have been performed on normal wrists, without ligamentous lesions. In the present study, we have analysed the differences that exist between the kinetic effects produced by individual or combined muscle contraction in normal wrists and those produced in the same wrists after sectioning the scapholunate ligaments.
Material and methodIn order to carry out this study, 15 frozen forearms were obtained and, after thawing at room temperature, we completely resected the skin and superficial fascia. The fingers, including the thumb, were amputated at the level of the metacarpophalangeal joint and the flexor and extensor tendons were extracted, preserving both retinacula. Without detaching them distally, the tendons of the main motor muscles in the wrist [namely abductor pollicis longus (APL), extensor carpi radialis longus (ECRL), extensor carpi ulnaris (ECU), flexor carpi ulnaris (FCU) and flexor carpi radialis (FCR)] were severed at the level of the medial third of the forearm. The tendon of the extensor carpi radialis brevis was completely removed because it interfered with the placement of the sensor on the scaphoid.
In order to verify the integrity of the intrinsic and extrinsic ligaments of the wrist and to enable the subsequent insertion of the sensors onto the dorsal face of the scaphoid and the triquetrum, a triangular capsule was resected between the dorsal radiocarpal ligament and the dorsal intercarpal ligament avoiding damage to these structures. Of the 15 specimens assigned to this study, 5 had to be discarded through the presence of some kind of intracarpal lesion that might have altered the results. The mean age of the 10 specimens included in this series was 77.3 years (range 65–91). There were 7 forearms from males and 3 from females, all unmatched; 5 were from the left arm and 5 from the right. After careful dissection at the conclusion of these experiments, all 10 specimens were considered normal.
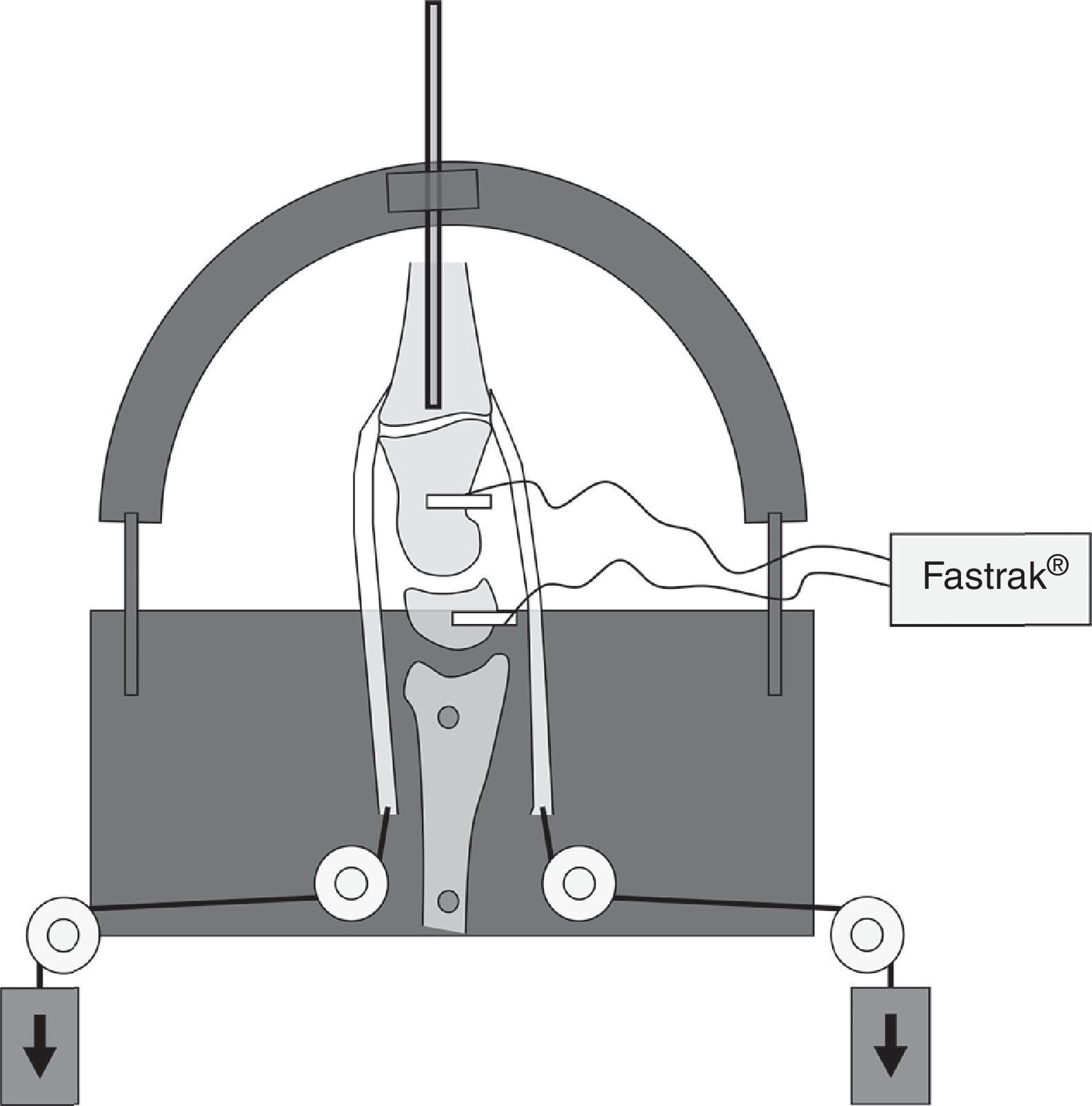
The specimens were placed vertically into a specially designed stand and fixed to it by means of 2 Steinman pins through the diaphyses of the radius and cubitus in a neutral rotation. In order to keep the hand aligned with the diaphysis of the radius in the sagittal and coronal planes, a needle was inserted in the medullary canal of the 3rd metacarpal and it was distally attached to the semi-circular guide on the stand in a neutral position of the wrist. This system prevented all sagittal and coronal movement of the carpus, although it did allow total freedom to migrate proximally and rotate in the axial plane (pronation-supination) without any restriction. This was an attempt to reproduce the conditions that exist when the fist is tightly clenched after blocking the wrist in a neutral position (Fig. 1).
. The Fastrack® system is used to determine changes in spatial alignment of the bones of the carpus under study by inserting sensors into the bones to be studied.")
Diagram of the stand used in these experiments. Muscle contraction is simulated by means of the application of weights to the motor tendons in the wrist severed at the level of the middle third of the forearm (arrows). The Fastrack® system is used to determine changes in spatial alignment of the bones of the carpus under study by inserting sensors into the bones to be studied.
By means of very strong nylon string, the proximal tip of the tendons was connected to a pulley system that enabled the tendons to be loaded with a variable number of weights. All of the tendons were placed under a constant load of 1.5Newtons (N) to imitate muscle tone. In order to simulate muscle contraction, the tendons were subjected to loads in proportion to their physiological cross-sectional area and the relative electromyographic activity exhibited by each muscle when holding an object with the wrist in neutral position.14 Following these criteria, the weights attached to the end of the different tendons were equivalent to the following forces: APL: 9.8N; ECRL: 24.5N; ECU: 14.7N; FCR: 13.7N and FCU: 21.5N.
In order to monitor the displacements and the spatial rotations in the scaphoid and the triquetrum, the Fastrack® system (Polhemus Inc., Colchester, VT, USA) was used. This system creates an electromagnetic field in which it is possible to calculate the position and alignment of certain specific movement markers (sensors) in connection with a fixed co-ordinate system (transmitter). The sensors work at a 30Hz refresh frequency, within an operational radius of action of 2.54–60.9cm around the transmitter. The static precision of the system was 0.8mm in translation and 0.15° in rotation. The sensors were attached to the dorsal face of the scaphoid, triquetrum and capitate by means of nylon screws so as not to interfere in the electromagnetic field. The magnetic field generator was fixed to the apparatus holding the specimen. It was decided not to apply a sensor on the lunate bone because, in neutral position, there was barely any bone surface left on which to attach a sensor without being supported on the dorsal edge of the radius.
In order to determine the spatial position of each sensor, a system of co-ordinates was defined by taking the radius as the reference. The Z axis corresponded to the longitudinal axis of the radius, the Y axis was aligned on the coronal plane, perpendicular to the Z axis, and the X axis was placed along the sagittal plane, perpendicular to the plane formed by the Y and Z axes (Fig. 2).

The spatial position of each sensor was determined in 14 different situations: with the wrist intact and without load, with the wrist intact and under a simultaneous load on all the tendons at the same time, with the wrist intact under an isolated load on each of the 5 tendons, and then repeating all the measurements again after having severed the scapholunate ligaments. Each determination was effected 5 consecutive times and the mean of the 5 determinations was used for the subsequent calculations.
The changes in position of the carpal bones secondary to the application of the different loads were assessed by comparing their position without load with the position adopted after applying load. In order to facilitate understanding, the displacements were broken down into their 3 rotational components (Euler angles): rotation around the Z axis (“azimuth” angle) indicates pronation-supination, rotation around the Y axis (“elevation” angle) indicates flexion-extension, and rotation around the X axis (“rotation” angle) indicates radial–cubital deviation.
After effecting the kinetic analysis of the normal carpus, we proceeded to provoke scapholunate instability. To this end, not only are the 3 components of the scapholunate ligament complex (dorsal, proximal and palmar portions) severed, but the long radiolunate ligament and the dorsal intercarpal ligament were also cut. Sufficient scapholunate instability was deemed to exist when the joint allowed diastasis in excess of 6mm. Once we were sure the suitable level of instability was present, we proceeded to repeat all the determinations and compare them with those obtained when the carpus was normal.
Each of the 3 components (azimuth, elevation and rotation) involved in the movement determined for each sensor by applying to them each of the 6 types of load with the wrist intact was statistically compared with the same determination effected after severing the scapholunate ligaments, using Wilcoxon's non-parametric test of ranges. When the p value was less than 0.05, the difference was considered to be statistically significant.
ResultsTable 1 reflects the displacements recorded by the scaphoid and triquetrum when applying simultaneous loads to all the tendons before and after severing the scapholunate ligaments. With the wrist intact, the muscle load causes rotation in supination, flexion and radial inclination in the first row of carpal bones. After severing the scapholunate ligaments, there is a significant change in the kinetic behaviour of both the scaphoid and the triquetrum: under a load on all the tendons together, the 2 bones under study do not supinate but undergo a rotation in pronation; this change is statistically significant (scaphoid p=0.049, triquetrum p=0.037). Equally noteworthy is the change in behaviour of both bones in the sagittal plane: following the severing of the scapholunate ligaments, the combined muscle load causes an increase in the flexion of the scaphoid, whereas the triquetrum is extended slightly.
Mobility presented by the bones in the proximal row of the carpus with load on all the tendons, before and after creating scapholunate instability.
| Scaphoid | Triquetrum | ||
| Normal | Unstable | Normal | Unstable |
| Azimuth | |||
| Supinatesa (7/10)b | Pronates (6/10) | Supinates (4/10) | Pronates (7/10) |
| M 0.49 | M 0.54° | M 0.65 | M 0.04° |
| SD±1.65° | SD±1.68° | SD±1.36 | SD±1.18 |
| Elevation | |||
| Flexes (10/10) | Flexes (10/10) | Flexes (7/10) | Extends (6/10) |
| M 2.22° | M 3.53° | M 0.27° | M 0.04° |
| SD±1.64° | SD±3.42° | SD±3.05° | SD±2.05° |
| Rotation | |||
| Radial (6/10) | Radial (8/10) | Radial (5/10) | Radial (6/10) |
| M 0.39° | M 0.70° | M 0.48° | M 0.66° |
| SD±1.13° | SD±1.31° | SD±1.36° | SD±1.85° |
Statistically significant changes are shown in bold.
M: mean; SD: standard deviation.
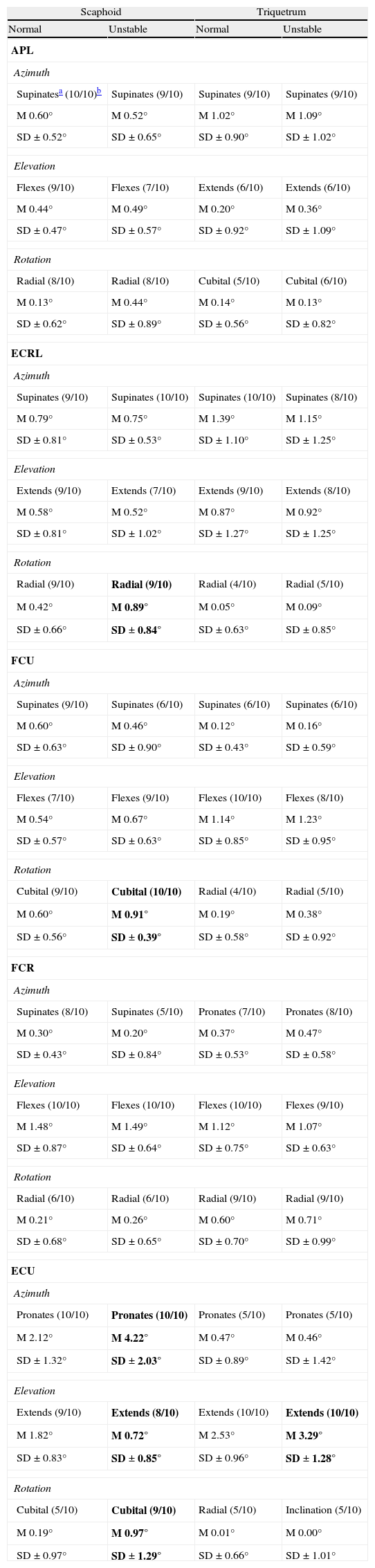
Table 2 shows the response of the scaphoid and the triquetrum when each of the tendons studied is placed under load individually, before and after creating scapholunate instability. As we can see, the muscle producing the most alterations on mobility of the scaphoid is the ECU: its action increases pronation (p=0.002), reduces extension (p=0.020) and significantly increases cubital inclination (p=0.037), producing the rotating instability typical of the scaphoid. As for the triquetrum, this muscle causes greater extension and this, together with the trend towards flexion shown by the scaphoid, will favour greater dissociation and a progressive deterioration in the joint.
Mobility presented by the bones in the first row of the carpus, with individual muscle load before and after creating scapholunate instability.
| Scaphoid | Triquetrum | ||
| Normal | Unstable | Normal | Unstable |
| APL | |||
| Azimuth | |||
| Supinatesa (10/10)b | Supinates (9/10) | Supinates (9/10) | Supinates (9/10) |
| M 0.60° | M 0.52° | M 1.02° | M 1.09° |
| SD±0.52° | SD±0.65° | SD±0.90° | SD±1.02° |
| Elevation | |||
| Flexes (9/10) | Flexes (7/10) | Extends (6/10) | Extends (6/10) |
| M 0.44° | M 0.49° | M 0.20° | M 0.36° |
| SD±0.47° | SD±0.57° | SD±0.92° | SD±1.09° |
| Rotation | |||
| Radial (8/10) | Radial (8/10) | Cubital (5/10) | Cubital (6/10) |
| M 0.13° | M 0.44° | M 0.14° | M 0.13° |
| SD±0.62° | SD±0.89° | SD±0.56° | SD±0.82° |
| ECRL | |||
| Azimuth | |||
| Supinates (9/10) | Supinates (10/10) | Supinates (10/10) | Supinates (8/10) |
| M 0.79° | M 0.75° | M 1.39° | M 1.15° |
| SD±0.81° | SD±0.53° | SD±1.10° | SD±1.25° |
| Elevation | |||
| Extends (9/10) | Extends (7/10) | Extends (9/10) | Extends (8/10) |
| M 0.58° | M 0.52° | M 0.87° | M 0.92° |
| SD±0.81° | SD±1.02° | SD±1.27° | SD±1.25° |
| Rotation | |||
| Radial (9/10) | Radial (9/10) | Radial (4/10) | Radial (5/10) |
| M 0.42° | M 0.89° | M 0.05° | M 0.09° |
| SD±0.66° | SD±0.84° | SD±0.63° | SD±0.85° |
| FCU | |||
| Azimuth | |||
| Supinates (9/10) | Supinates (6/10) | Supinates (6/10) | Supinates (6/10) |
| M 0.60° | M 0.46° | M 0.12° | M 0.16° |
| SD±0.63° | SD±0.90° | SD±0.43° | SD±0.59° |
| Elevation | |||
| Flexes (7/10) | Flexes (9/10) | Flexes (10/10) | Flexes (8/10) |
| M 0.54° | M 0.67° | M 1.14° | M 1.23° |
| SD±0.57° | SD±0.63° | SD±0.85° | SD±0.95° |
| Rotation | |||
| Cubital (9/10) | Cubital (10/10) | Radial (4/10) | Radial (5/10) |
| M 0.60° | M 0.91° | M 0.19° | M 0.38° |
| SD±0.56° | SD±0.39° | SD±0.58° | SD±0.92° |
| FCR | |||
| Azimuth | |||
| Supinates (8/10) | Supinates (5/10) | Pronates (7/10) | Pronates (8/10) |
| M 0.30° | M 0.20° | M 0.37° | M 0.47° |
| SD±0.43° | SD±0.84° | SD±0.53° | SD±0.58° |
| Elevation | |||
| Flexes (10/10) | Flexes (10/10) | Flexes (10/10) | Flexes (9/10) |
| M 1.48° | M 1.49° | M 1.12° | M 1.07° |
| SD±0.87° | SD±0.64° | SD±0.75° | SD±0.63° |
| Rotation | |||
| Radial (6/10) | Radial (6/10) | Radial (9/10) | Radial (9/10) |
| M 0.21° | M 0.26° | M 0.60° | M 0.71° |
| SD±0.68° | SD±0.65° | SD±0.70° | SD±0.99° |
| ECU | |||
| Azimuth | |||
| Pronates (10/10) | Pronates (10/10) | Pronates (5/10) | Pronates (5/10) |
| M 2.12° | M 4.22° | M 0.47° | M 0.46° |
| SD±1.32° | SD±2.03° | SD±0.89° | SD±1.42° |
| Elevation | |||
| Extends (9/10) | Extends (8/10) | Extends (10/10) | Extends (10/10) |
| M 1.82° | M 0.72° | M 2.53° | M 3.29° |
| SD±0.83° | SD±0.85° | SD±0.96° | SD±1.28° |
| Rotation | |||
| Cubital (5/10) | Cubital (9/10) | Radial (5/10) | Inclination (5/10) |
| M 0.19° | M 0.97° | M 0.01° | M 0.00° |
| SD±0.97° | SD±1.29° | SD±0.66° | SD±1.01° |
Statistically significant changes are shown in bold.
SD: standard deviation; M: mean.
Isolated contraction of the FCU may also impair scapholunate stability, in this case due to the tendency to force the maximum cubital inclination of the scaphoid, thus producing an increase in the scapholunate diastasis. On the contrary, the isolated load on the 3 tendons on the radial side of the wrist induces supination of the scaphoid to a greater or lesser extent and this would be beneficial as it would close the diastasis typical of scapholunate instability.
DiscussionThe idea of muscles participating in the stabilization of joints is not a new concept. Reviewing the literature, we find articles referring to this notion as early as 1980, when Kauer18,19 hypothesized that the extensor pollicis brevis, the APL and the ECU played a specific role in the stability of the carpus, acting as a dynamic collateral system providing stability in flexion-extension and radiocubital inclination movements. In 1992, Ruby20 suggested that all the tendons crossing through the wrist have a dynamic effect on joint stability.
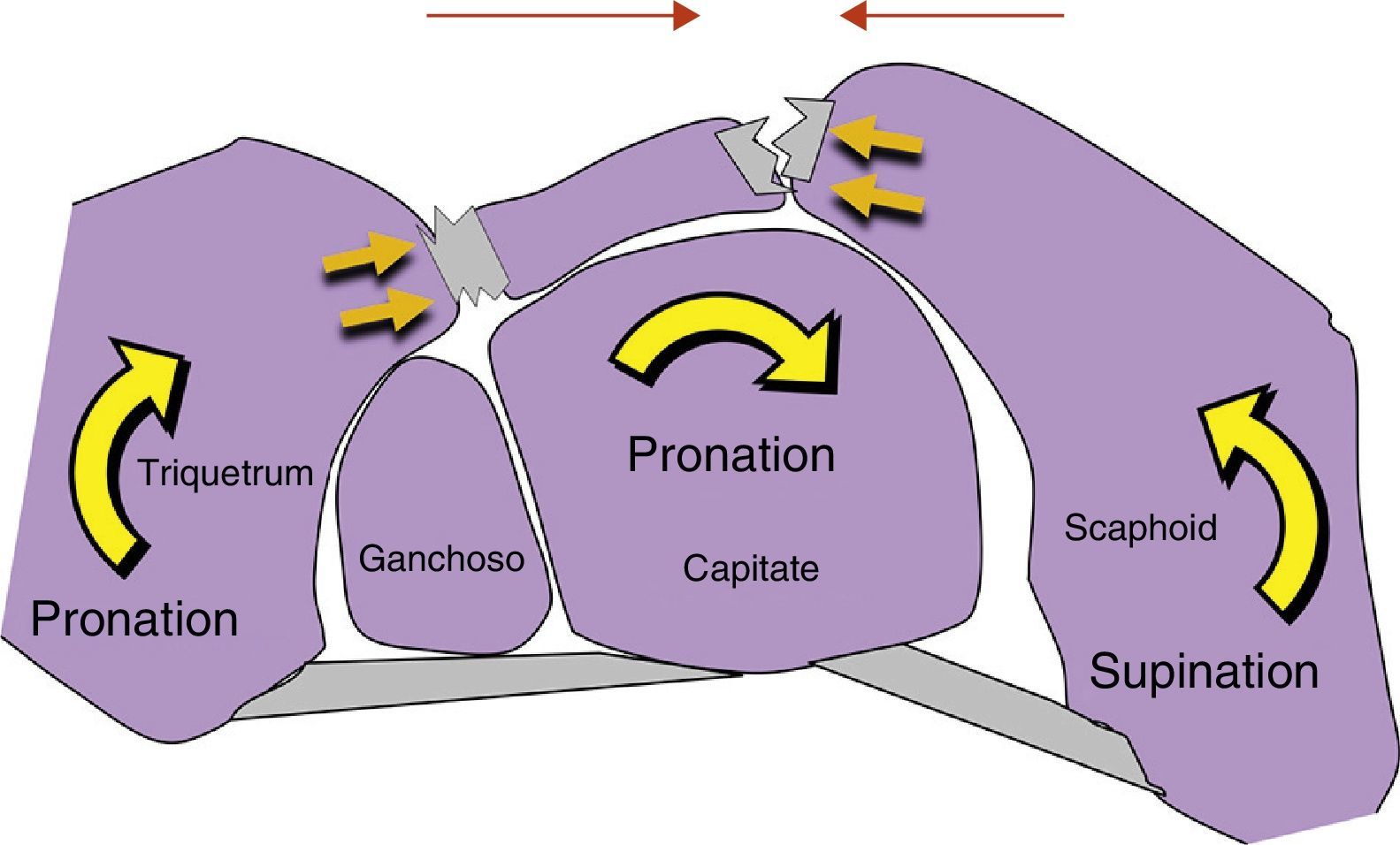
In 1994, Jantea et al.21 attributed to the FCR a specific role in dynamic stabilization of the wrist, based on the fact that this tendon uses the tuberosity of the scaphoid to increase the distance separating it from the wrist's centre of rotation and thus its mechanical performance. Based on this observation, it was suggested that the isometric contraction of the FCR might generate an extensor moment on the scaphoid that would balance the opposing trend of the scaphoid to flex under load. This hypothesis was repeated in several other bibliographical citations, although never proved.13,21–24 Contradicting that hypothesis, Salvà-Coll et al.17 observed that the isolated isometric load on the FCR did not produce extension in the scaphoid, but rather the opposite effect regardless of the wrist's position when the load is applied. Although the hypothesis defended by Jantea et al.21 has lost verisimilitude, it was still true that boosting the FCR usually improves the symptoms in cases of dynamic instability of the scaphoid.12–14 According to Salvà-Coll et al.,16 the mechanism leading to that improvement would have to do with the fact that the FCR, apart from pronating the distal row and the triquetrum, supinates the scaphoid. Therefore, if the scaphoid is supinated and the triquetrum pronated, it is logical for converging forces to appear on the scapholunate joint to ensure its stability (Fig. 3).

Since mechanoreceptors were shown to be present in the ligaments of the wrist,8–12 a good number of experimental papers have attempted to correlate propioception to the muscle mechanisms controlling the carpus. Using a complex biplanar stereoradiographic method, Kobayashi et al.14 studied the kinetic behaviour of the proximal row of the carpus when isometric loads are applied to the motor muscles in the wrist. The results of the present study coincide to a large extent with those of Kobayashi et al.14 in showing that an intact carpus, under axial load, tends to rotate towards supination. Subsequently, Salvà-Coll,15 using an experimental model similar to the preceding one, studied the effect of individual muscle contraction on the alignment of certain bones in the carpus. On the basis of these studies, it was proposed to classify the motor muscles in the wrist into 2 groups: those pronating the mediocarpal joint (ECU and FCR) and those supinating it (FCU, ECRL and APL). These movements would be transmitted to the proximal row through the ligaments crossing through the mediocarpal joint.16 Following on from all this, it was inferred that the action of the supinating muscles would protect the scapholunate space, whereas the action of the pronating muscles would have a protective effect on the lunotriquetral space.21
All the experimental papers mentioned so far were carried out on stable carpi; our study is the first to assess the effect of the musculature in the forearm on an unstable carpus. Under normal conditions, when the anatomically intact carpus receives a load through all the tendons at the same time, the proximal row tends towards supination. On the other hand, if the carpus already has a scapholunate lesion, a joint load on all the tendons produces the contrary effect: the scaphoid collapses in flexion and pronation, while the triquetrum pronates and extends.25 The present study has also assessed the effects of an individual load on a carpus with a scapholunate lesion. The results seem to indicate that the muscles causing pronation and cubital inclination of the carpus are those that add the most instability to an already unstable carpus due to scapholunate disruption. The muscles on the radial side, on the other hand, promote scapholunate coaptation and thus its stability (Fig. 4B). All this leads us to show that, where there is already a lesion in the scapholunate ligaments, the individual or combined action of the supinating muscles of the scaphoid (FCR, APL and ECRL) may neutralize carpial instability and make the wrist asymptomatic. On the contrary, the individual or combined action of the muscles causing cubital inclination in the carpus (FCU and ECU), and particularly the action of this last muscle due to its ability to pronate the scaphoid, may very probably end up de-stabilizing even more an already unstable wrist.
 Dorsal view of a specimen in which scapholunate dissociation has been effected prior to subjecting it to any muscle load. (B) Here we can observe a slight increase in the coaptation of the scapholunate space with an individual load on the ECRL. (C) With an individual load on the ECU, there is an increase in scapholunate dissociation.")
(A) Dorsal view of a specimen in which scapholunate dissociation has been effected prior to subjecting it to any muscle load. (B) Here we can observe a slight increase in the coaptation of the scapholunate space with an individual load on the ECRL. (C) With an individual load on the ECU, there is an increase in scapholunate dissociation.
The conclusions reached in the present experimental paper are congruent with the in vivo experiments by Hagert et al.12 After electrically stimulating the dorsal scapholunate ligament in normal volunteers, the appearance of a nociceptive reflex was seen to provoke the contraction of certain muscles and the inhibition of others. This first group included the 3 supinating muscles of the scaphoid on the radial side of the wrist, whereas the second group included the ECU. In fact, when scapholunate ligaments are injured, the isometric contraction of the ECU may worsen the initial instability.
From a practical standpoint, each muscle group must be strengthened or inhibited depending on the type of ligament that is damaged. If a mistaken muscle group is exercised, we may increase the symptoms in patients with a ligament problem. Specifically, our paper suggests that, in the presence of dynamic scapholunate instability (when carpal collapse has not yet occurred), either in an acute phase or following the repair of the ligaments, it is necessary to use immobilization ferules that force intracarpal supination in order to relax the scapholunate ligaments and the cubital deviation of the wrist to inhibit the negative effect of the ECU. Secondarily, it is necessary to insist on specific physiotherapy for this kind of instability, aimed at boosting the muscles on the radial side that supinate the scaphoid (FCR, APL and ECRL), and at inhibiting the muscles on the cubital side (ECU and FCU).
Level of evidenceLevel of evidence I.
Ethical responsibilitiesProtection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Confidentiality of Data. The authors declare that no patient data appears in this article.
Right to privacy and informed consent. The authors declare that no patient data appears in this article.
Conflict of interestThe authors have no conflict of interests to declare.
Please cite this article as: León-López MM, García-Elías M, Salvà-Coll G, Llusá-Perez M, Lluch-Bergadà A. Control muscular de la inestabilidad escafolunar. Estudio experimental. Rev Esp Cir Ortop Traumatol. 2014;58:11–18.
