




To evaluate, experimentally in cadavers, the effect of the motor muscles in the wrist in the kinetic behaviour of the carpal, under axial load, and the wrist in a neutral position.
Material and methodThe changes in the spatial orientation of the carpal bones were recorded with a movement trajectory gauge that functions with electromagnetic fields. A total of 30 fresh cadaver wrists were used, in which the principal motor tendons were isolated and subjected to loads proportional to the area of the physiological section of each muscle. The experiment was performed under isometric load conditions of all the tendons, and separately from each tendon.
ResultsThe simultaneous load of all the tendons studied caused a three-dimensional change of the carpal bones. The flexor carpi radialis led to supination of the scaphoids and pronation of the pyramidal. Conversely, the isolated load of the flexor carpi ulnaris, abductor pollicis longus and the extensor carpi radialis longus, caused a supination movement of the 2 carpal rows. Only the extensor carpi ulnaris led to a marked pronation of the carpal.
Comments and conclusionsThe forearm muscles, as well as the movements of the wrist, cause pronation/supination/supination, flexion/extension and radial/cubital inclination movements. It is proposed that the most important movements in the dynamic stabilisation of the carpal are the intercarpal pronation and supination movements provoked by these muscles. Depending on the carpal injury mechanism or instability, the stimulating of one muscle group or the other may be beneficial.
Valorar de forma experimental en cadáver el efecto de los músculos motores de la muñeca en el comportamiento cinético del carpo, bajo carga axial y en posición neutra de la muñeca.
Material y métodoSe registraron los cambios de orientación espacial de los huesos del carpo, con un registrador de trayectoria de movimiento que funciona con campos electromagnéticos. Se utilizaron 30 muñecas de cadáver fresco, cuyos principales tendones motores de la muñeca fueron aislados y sujetos a cargas proporcionales al área seccional fisiológica de cada músculo. El experimento se llevó a cabo en condiciones de carga isométrica de todos los tendones, y de forma aislada de cada tendón.
ResultadosLa carga simultánea de todos los tendones estudiados provocó una modificación de la posición tridimensional de los huesos del carpo. El flexor carpi radialis provocó supinación del escafoides y pronación del piramidal. En cambio, la carga aislada del flexor carpi ulnaris, abductor pollicis longus y extensor carpi radialis longus provocaron un movimiento de supinación de las 2 filas del carpo. Solo el extensor carpi ulnaris provocó una pronación marcada del carpo.
Comentarios y conclusionesLos músculos del antebrazo, además de los movimientos de la muñeca, provocan movimientos de pronación/supinación, flexión/extensión e inclinación radial/cubital. Proponemos que el movimiento más importante en la estabilización dinámica del carpo son los movimientos de pronación y supinación intercarpiana provocados por estos músculos. Según el mecanismo lesional o inestabilidad carpiana, puede ser beneficiosa la potenciación de un grupo muscular u otro.
Since the beginning of the study of carpal biomechanics, most efforts have focused on the description of those anatomical structures related to the stability of the carpus (ligaments, joint capsule and bone morphology), their function and the pathologies that cause lesions to these structures, in an attempt to know which are responsible for each specific instability pattern and what would be the most adequate treatment.
There is another very important, yet underrated, factor which is involved in joint stability, and which is linked to neuromuscular control mechanisms on joint stability. Unlike other joints such as the knee1 or shoulder,2 of which there are many studies focusing on proprioception and the effect of musculature, there are very few articles published on the carpus so far. The motor muscles of the wrist exert a dynamic effect on the carpal bones, increasing the stability of the joint.
In order to determine the mechanical effect of the main motor tendons of the wrist on the carpal bones and clarify their role as dynamic stabilisers, an experimental study was designed to evaluate the kinetic behaviour of the scaphoid, capitate and triquetrum (or pyramidal) bones under an axial load and in a neutral position of the wrist.
Material and methodThis study was conducted on 30 fresh cadaver arms. The anatomical specimens were used in accordance to current laws and regulations at our institution. The mean age of the specimens was 79 years (range: 55–95 years), of which 18 were males and 12 were females. The specimens included 18 left arms and 12 right arms, all with a type I lunate bone (with no medial facet, unlike type II in which there is an articular facet for the hamate bone3).
Preparation of the anatomical specimens consisted in complete removal of the skin and subcutaneous tissue, identification and isolation of the main motor tendons of the wrist at the level of the middle third of the forearm, whilst maintaining intact the retinaculum of the extensors and flexors: extensor carpi radialis longus (ECRL), abductor pollicis longus (APL), extensor carpi ulnaris (ECU), flexor carpi radialis (FCR) and flexor carpi ulnaris (FCU). Disarticulation of the fingers was performed at the metacarpophalangeal joint. We identified the dorsal ligaments of the carpus and conducted a limited capsular resection without damaging the dorsal radiotriquetral and dorsal intercarpal extrinsic ligaments, or the intrinsic ligaments. In this study we performed removal of the extensor carpi radialis, due to the interference of this tendon with placement of the nylon screw used to attach the scaphoid sensor.
Next, the anatomical specimens were placed in a support designed specifically for this study, in a vertical position and neutral pronosupination using 2 Steinmann nails on the radius and ulna (Fig. 1). The position of the wrist was controlled via an intramedullary Kirschner wire placed in the third metacarpal and connected to a semicircular device in the upper part of the support. This Kirschner wire almost completely blocked any flexion/extension movements and radial/ulnar inclinations of the distal carpal row, whilst allowing proximal migration and rotations. These movements were transmitted to the proximal carpal row when the ligaments were intact. Thus, in wrists with intact ligaments and under axial load, proximal migration and rotations of the distal carpal row were transmitted to the proximal row, causing a three-dimensional movement of the bones of the proximal carpal row.

Each tendon was connected to a system of pulleys with a nylon thread. This thread allowed the placement of weights to simulate the contraction of forearm musculature.
In order to record the changes of position of the carpal bones we used a 3D digitiser device and a Fastrak™ (Polhemus Inc., Colchester, Vermont, USA) motion path recorder. This apparatus used electromagnetic fields to provide a dynamic and real-time measurement of both position (in X, Y and Z Cartesian coordinates) and orientation (in Euler angles: azimuth, elevation and rotation), by locating the position and orientation of a small receiver as it moved through space. For this study we used 4 receptor sensors operating at a refresh rate of 30Hz and a short-range transmitter designed especially for the monitoring areas, covering a radius of 2.54–60.9cm. The static accuracy of this system was 0.08cm for the position and 0.15° for the spatial orientation. The sensors were firmly placed on the dorsal side of the radius and on the scaphoid, triquetrum and capitate bones using nylon screws. The nylon screw of the scaphoid was distally angled between 20 and 30°, so as to avoid contact with the radius during the extension movement of the scaphoid when conducting a load on the extensor carpi radialis longus and the ECU. The sensors in the proximal row were placed on the scaphoid and triquetrum, since these have opposite tendencies towards flexion or extension. The lunate is interposed and, therefore, it is dragged by the scaphoid towards flexion in case of lunotriquetral lesion and towards extension in case of scapholunate lesion.
The load applied to each tendon was based on previous research which suggested the use for such experiments of loads commensurate with the transverse sectional area of the muscle, along with the relative electromyographic activity of each muscle when an object was held with the wrist in a neutral position.4–6 In order to simulate muscle tone at rest we performed a load on each tendon with a weight equivalent to 1.5Newton (N). To simulate muscle contraction we used a weight equivalent to 9.8N for the APL, 24.5N for the ECRL, 14.7N for the ECU, 13.7N for the FCR and 21.5N for the FCU. The coordinate system of the transmitter and the 4 receivers was calculated according to the longitudinal axis of the radius. The Z-axis was defined along the longitudinal axis of the radius, the Y-axis was defined along the frontal plane perpendicular to the Z-axis and the X-axis in the sagittal plane, perpendicular to the Z and Y axes. Thus, rotation about the Z-axis (azimuth) corresponded to pronation and supination, rotation about the Y-axis (elevation) corresponded to flexion and extension, and rotation about the X-axis (rotation) corresponded to radial and ulnar inclination. Data collection was performed during 5 consecutive measurements and the mean value was used to determine changes of sensor position. These means were statistically analysed using the Wilcoxon test for paired data through the SPSS v15 software package. Differences were considered statistically significant when the value of P was <.05.
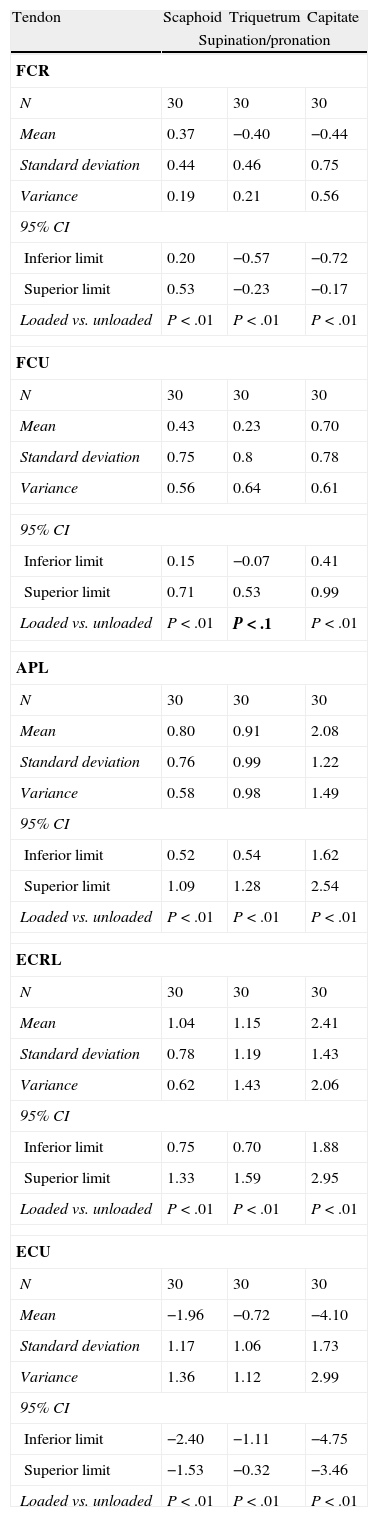
ResultsSimultaneous loading of all tendons studied caused a change in the three-dimensional position of the carpal bones. Loading of all the tendons caused a further carpal supination, in addition to flexion of the proximal row. Table 1 lists the data for the individual load of each tendon. In most cases, isolated load of the FCR caused scaphoid supination, as well as triquetral and capitate pronation. Meanwhile, isolated load of the FCU, ECRL and APL caused supination of both rows of the carpus. Only the ECU caused a marked pronation of the carpus, of both the proximal and distal rows.
Effect of isolated loads on the main motor tendons of the wrist in the transverse rotation plane.
| Tendon | Scaphoid | Triquetrum | Capitate |
| Supination/pronation | |||
| FCR | |||
| N | 30 | 30 | 30 |
| Mean | 0.37 | −0.40 | −0.44 |
| Standard deviation | 0.44 | 0.46 | 0.75 |
| Variance | 0.19 | 0.21 | 0.56 |
| 95% CI | |||
| Inferior limit | 0.20 | −0.57 | −0.72 |
| Superior limit | 0.53 | −0.23 | −0.17 |
| Loaded vs. unloaded | P<.01 | P<.01 | P<.01 |
| FCU | |||
| N | 30 | 30 | 30 |
| Mean | 0.43 | 0.23 | 0.70 |
| Standard deviation | 0.75 | 0.8 | 0.78 |
| Variance | 0.56 | 0.64 | 0.61 |
| 95% CI | |||
| Inferior limit | 0.15 | −0.07 | 0.41 |
| Superior limit | 0.71 | 0.53 | 0.99 |
| Loaded vs. unloaded | P<.01 | P<.1 | P<.01 |
| APL | |||
| N | 30 | 30 | 30 |
| Mean | 0.80 | 0.91 | 2.08 |
| Standard deviation | 0.76 | 0.99 | 1.22 |
| Variance | 0.58 | 0.98 | 1.49 |
| 95% CI | |||
| Inferior limit | 0.52 | 0.54 | 1.62 |
| Superior limit | 1.09 | 1.28 | 2.54 |
| Loaded vs. unloaded | P<.01 | P<.01 | P<.01 |
| ECRL | |||
| N | 30 | 30 | 30 |
| Mean | 1.04 | 1.15 | 2.41 |
| Standard deviation | 0.78 | 1.19 | 1.43 |
| Variance | 0.62 | 1.43 | 2.06 |
| 95% CI | |||
| Inferior limit | 0.75 | 0.70 | 1.88 |
| Superior limit | 1.33 | 1.59 | 2.95 |
| Loaded vs. unloaded | P<.01 | P<.01 | P<.01 |
| ECU | |||
| N | 30 | 30 | 30 |
| Mean | −1.96 | −0.72 | −4.10 |
| Standard deviation | 1.17 | 1.06 | 1.73 |
| Variance | 1.36 | 1.12 | 2.99 |
| 95% CI | |||
| Inferior limit | −2.40 | −1.11 | −4.75 |
| Superior limit | −1.53 | −0.32 | −3.46 |
| Loaded vs. unloaded | P<.01 | P<.01 | P<.01 |
APL: abductor pollicis longus; CI: confidence interval; ECRL: extensor carpi radialis longus; ECU: extensor carpi ulnaris; FCR: flexor carpi radialis; FCU: flexor carpi ulnaris.
All data are expressed in degrees.
Supination/pronation: positive values indicate supination and negative values indicate pronation.
Loaded vs. unloaded. Student t-test. Statistical significance P<.05.
Data in bold were not considered statistically significant.
Despite the importance of neuromuscular reflexes and forearm muscle action in carpal stability,7–10 to date very few articles have been published on this topic. In 1980, Kauer demonstrated that the extensor pollicis brevis, APL and ECU were in an isometric position during wrist flexion/extension movements. Along with the observation that these tendons practically do not move during such movements, this author described them as an adjustable, collateral system. However, no mention was made of the role of these muscles as carpal stabilisers.11 In 1992, Ruby suggested that all the tendons crossing the wrist could have a dynamic effect on carpal stability, but did not define the role of each muscle in the dynamic stabilisation of the carpus.12 The FCR is the only muscle that has been attributed a specific role as a stabiliser of the scaphoid. In 1994, Jantea et al. suggested that the FCR played a role as scaphoid dynamic stabiliser during carpal movement. This was based on the observation that the tendon of this muscle used the distal pole of the scaphoid as a reflection pulley, and therefore its contraction caused scaphoid extension, preventing a collapse during flexion of the scaphoid under a load.13 However, Salva Coll et al. demonstrated that in different degrees of flexion and extension of the wrist, the FCR always causes a scaphoid flexion movement.14 This is due to the oblique position of the scaphoid with respect to the longitudinal axis of the forearm. When performing an FCR tendon load, the force is transmitted through the scaphotrapeziotrapezoid joint, and this causes a scaphoid flexion.
Based on the findings of our study, it seems reasonable to divide the motor muscles of the wrist into 2 groups: those muscles that cause a pronation movement in the distal carpal row, namely the ECU and FCR, and those causing a supination movement, the ECRL, APL and FCU.
Clearly, if the carpal ligaments are intact, these movements in the distal carpal row are transmitted to the proximal row. Thus, a correct interaction and muscular balance are crucial in the dynamic stabilisation of the carpus. Under axial load, the scaphoid tends towards flexion and pronation. There are several theories which attempt to explain the compensatory mechanisms of this natural tendency. Kauer suggests that this tendency is countered by a tendency of the lunate to spread, due to its configuration as a palmar wedge.11 However, Weber suggests that this tendency is countered by the morphology of the triquetrohamate joint, which prevents flexion of the triquetrum.15 In fact, when there is a load of all tendons, the resultant movement is a flexion of the proximal row, but in supination. Therefore, this supination would counteract the tendency toward pronation of the scaphoid. Moreover, supination of the scaphoid and the proximal row could exert a protective effect on the scapholunate ligament, by decreasing the scapholunate space and reducing the loads to which it is subjected. Instead, the ECU, which is the only muscle causing scaphoid pronation, would act as a destabiliser of the scapholunate joint and could even worsen any preexisting scapholunate instability.
In summary, this study describes the effects of an isometric load of the 5 forearm muscles on the three-dimensional alignment of the scaphoid, triquetrum and capitate bones. In the transverse plane of rotation, the motor muscles of the wrist can be divided into pronators and supinators, depending on their effect on the proximal and distal rows of the carpus.
The supination movement, which is transmitted to the scaphoid and the proximal row, would counter the natural tendency of the scaphoid to rotate in pronation, thus acting as a “protector” of the scapholunate ligament, whilst the ECU, a powerful pronator, could worsen any preexisting scapholunate instability. These findings may be used as a basis for studies which develop a specific muscle strengthening protocol, depending on the type of carpal ligament reconstruction or lesion.
Level of evidenceLevel of evidence iii.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation did not require experiments on humans or animals.
Confidentiality of dataThe authors declare that this work does not reflect any patient data.
Right to privacy and informed consentThe authors declare that this work does not reflect any patient data.
FinancingThis study obtained a grant from Fundación SECOT for research projects in 2008, as well as a grant from “Societat Catalana de Cirurgia Ortopèdica i Traumatología” (Catalan Orthopaedic Surgery and Traumatology Society) for the completion of doctoral theses in 2008.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Salvà Coll G, et al. Mecanismos de estabilización dinámica del carpo. Estudio experimental. Rev Esp Cir Ortop Traumatol. 2013;57:129-34.
