



The management of Mason II fracture pattern assisted by arthroscopy is a valid technique that provides good results. The objective of this study was to draw attention to the usefulness of the location of the fracture in the head of the radius in defined quadrants with respect to the bicipital tuberosity through CT. This would help to plan the optimal forearm position to access each quadrant and foresee the specific difficulties of each one.
Material and methodWe dissected 4 specimens of cryopreserved cadaver. We divided the radial head into 4 quadrants with regard to the bicipital tuberosity, objectifying the change of position in pronation and maximum supination with respect to the sigmoid cavity and neurovascular structures.
ResultsThe head of the radio moves with pronosupination, so there are areas of convergence between the different quadrants. Quadrant 1 is approached in supination via an anteromedial portal. Quadrant 2 is approached in maximum pronation through a lateral portal. Quadrant 3 can be approached through lateral portals, with the forearm in neutral position and in pronation. Quadrant 4 is accessible with the forearm in a neutral position and in supination through a lateral portal.
ConclusionsDepending on the location of the fracture in the head of the radius with respect to the bicipital tuberosity, we will need access through a specific arthroscopic portal, with the medial quadrants (anteromedial and posteromedial) being the most technically demanding.
La reducción y fijación de la fractura de la cabeza del radio tipo Mason II asistida por artroscopia es una técnica válida que proporciona buenos resultados. El objetivo de este estudio es llamar la atención sobre la utilidad de la localización de la fractura en la cabeza del radio en cuadrantes definidos con respecto a la tuberosidad bicipital mediante la TC. Ello ayudaría a planificar la posición del antebrazo óptima para acceder a cada cuadrante y prever las dificultades específicas de cada uno.
Material y métodoSe ha procedido a la disección de 4 especímenes de cadáver criopreservado. Hemos dividido la cabeza del radio en 4 cuadrantes con respecto a la tuberosidad bicipital objetivando el cambio de posición en pronación y en supinación máxima con respecto a la cavidad sigmoidea menor y a las estructuras neurovasculares.
ResultadosLa cabeza del radio se desplaza con la pronosupinación, por lo que existen áreas de convergencia entre los distintos cuadrantes. El cuadrante 1 se aborda en supinación por un portal anteromedial. El cuadrante 2 se aborda en pronación máxima mediante un portal lateral. El cuadrante 3 se puede abordar a través de portales laterales, con el antebrazo en posición neutra y en pronación. El cuadrante 4 es accesible con el antebrazo en posición neutra y en supinación a través de un portal lateral.
ConclusionesSegún la localización de la fractura en la cabeza del radio con respecto a la tuberosidad bicipital, necesitaremos acceder por un portal artroscópico determinado, siendo los cuadrantes mediales (anteromedial y posteromedial) los más exigentes técnicamente.
The treatment of transverse pattern of Mason II radial head fractures is controversial, although basically they are considered to be a secondary fracture that can be reconstructed and treated surgically by reduction and internal fixation.1,2 Reduction is usually performed using an open approach. Nevertheless, thanks to improvements in specific instrumentation and familiarity with the technique, in cases where surgical treatment is indicated arthroscopy may be a useful resource with clear advantages. Some recent studies show that the arthroscopically assisted reduction and fixation of intrajoint fractures of the elbow is a valid technique that gives patients good functional results.
It is possible to obtain a better view of the joint surface, and this may help to gain greater understanding of fracture morphology, thereby facilitating a more exact and therefore anatomical reduction. Another of its advantages is that it allows us to better evaluate associated lesions in comparison with the open technique. It is possible to resect loose bodies, to resect osteophytes and to debride cartilage lesions. It is also possible to obtain additional benefits, such as gaining early rehabilitation due to having caused less damage to tissues, having eliminated the haematoma from within the joint during irrigation and aspiration, reducing intra-joint adherences, and lastly minimising scar size.3–5
Nevertheless, the authors of the papers cited above admit that this is a technically demanding procedure, so that surgeons must have sufficient previous experience. The number of portals described to access the elbow has gradually increased, although always taking into account the series of structures that surround the joint which we have to be aware of. The fact is that neurovascular complications are the most feared.5–10
The radial head is an ovoid structure which, depending on its degree of pronosupination, makes it possible to change the position of the same respecting the lesser sigmoid cavity of the cubitus. This permits movement in a 180° arch of an area of the head, in this case the fractured zone to be repaired.11–14 However, the fragment to be synthesised may only be accessible through certain portals, depending on the location of the fracture route and bone fragments.15
The difficulty in accessing and treating a Mason II radial head fracture arthroscopically varies depending on its location. This difficulty arises due to the lesser sigmoid cavity and the neurovascular structures of the elbow. The aim of this study is to underline the importance of the location of the radial head fracture, based on study of the transversal pattern detected by CT imaging. Likewise, given the closeness of the bicipital tuberosity of the radius, it is possible to establish the quadrants respecting the same and to use it as a reference point. This allows us to precisely locate the fracture respecting the lesser sigmoid cavity, and thereby achieve optimum preoperative planning. By knowing the location of the quadrants, we will be able to plan the forearm position that makes it possible to access the said quadrant, and this therefore indicates which portal should be used for osteosynthesis of the fracture. Given that technical demands and possible complications may vary considerably depending on the difficulty of a case, we believe that this may be useful by ensuring that surgeons are better prepared before an operation, and even that patients are better informed.
Materials and methodsFour cryopreserved cadaveric specimens were dissected after coloured latex was injected into the humeral artery at arm level, filling the vascular tree up to the level of the arterioles. A measured dissection was performed and the main muscle and neurovascular structures were studied at the distal level of the arm. More specifically the elbow structure was studied in transversal slices.
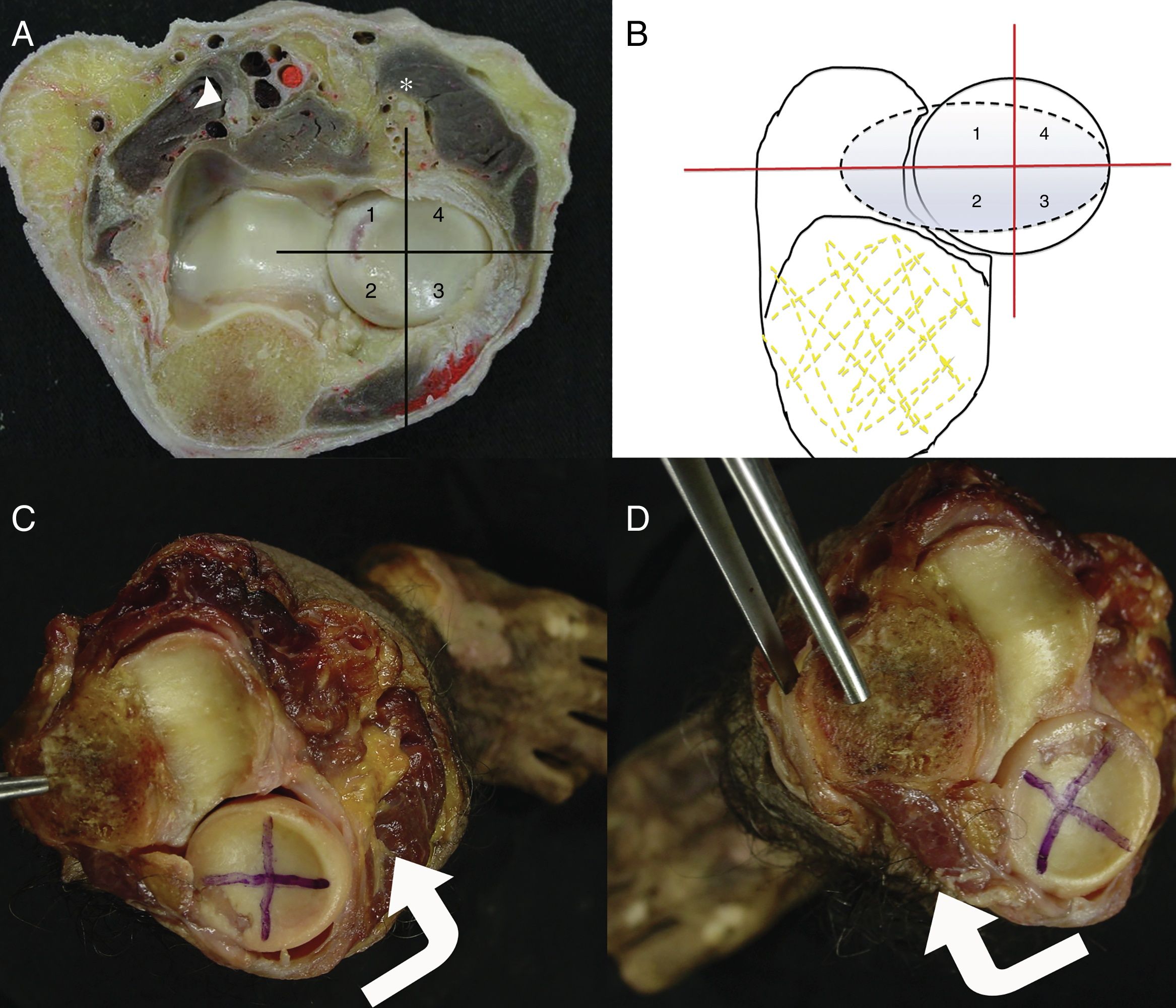
We divided the radial head into 4 quadrants: 1 (superomedial), 2 (posteromedial), 3 (posterolateral) and 4 (anterolateral), taking a plane that coincides with the largest diameter of the bicipital tuberosity as the first axis, while the second axis was perpendicular to the first (Fig. 1A and B). We took photographs of the proximal radiocubital joint in pronation and in maximum supination to detect displacement of the radial head respecting the lesser sigmoid cavity, together with the most important neurovascular structures at elbow level (Fig. 1C and D). Additionally, diagrams have been superimposed that aid comprehension of the position of each quadrant and how pronation and supination affect them.
 Proximal transversal slice of a right elbow, where it is possible to see the proximal radiocubital joint and the association with neurovascular structures. In the medial zone the median nerve (arrow head) is “protected” and separated from the joint capsule by the brachialis muscle, while the radial nerve (*) is very close to the joint capsule in the lateral zone of the elbow. (B) We have divided the radial head into 4 quadrants in this diagram: 1 (superomedial), 2 (posteromedial), 3 (posterolateral) and 4 (anterolateral), taking a plane that coincides with the greater diameter of the bicipital tuberosity (dotted line) as the first axis, and where the second axis is perpendicular to the first. (C and D) We took photographs of the proximal radiocubital joint in maximum pronation and supination to show the displacement of the head respecting the lesser sigmoid cavity and the most important neurovascular structures at the level of the elbow.")
(A) Proximal transversal slice of a right elbow, where it is possible to see the proximal radiocubital joint and the association with neurovascular structures. In the medial zone the median nerve (arrow head) is “protected” and separated from the joint capsule by the brachialis muscle, while the radial nerve (*) is very close to the joint capsule in the lateral zone of the elbow. (B) We have divided the radial head into 4 quadrants in this diagram: 1 (superomedial), 2 (posteromedial), 3 (posterolateral) and 4 (anterolateral), taking a plane that coincides with the greater diameter of the bicipital tuberosity (dotted line) as the first axis, and where the second axis is perpendicular to the first. (C and D) We took photographs of the proximal radiocubital joint in maximum pronation and supination to show the displacement of the head respecting the lesser sigmoid cavity and the most important neurovascular structures at the level of the elbow.
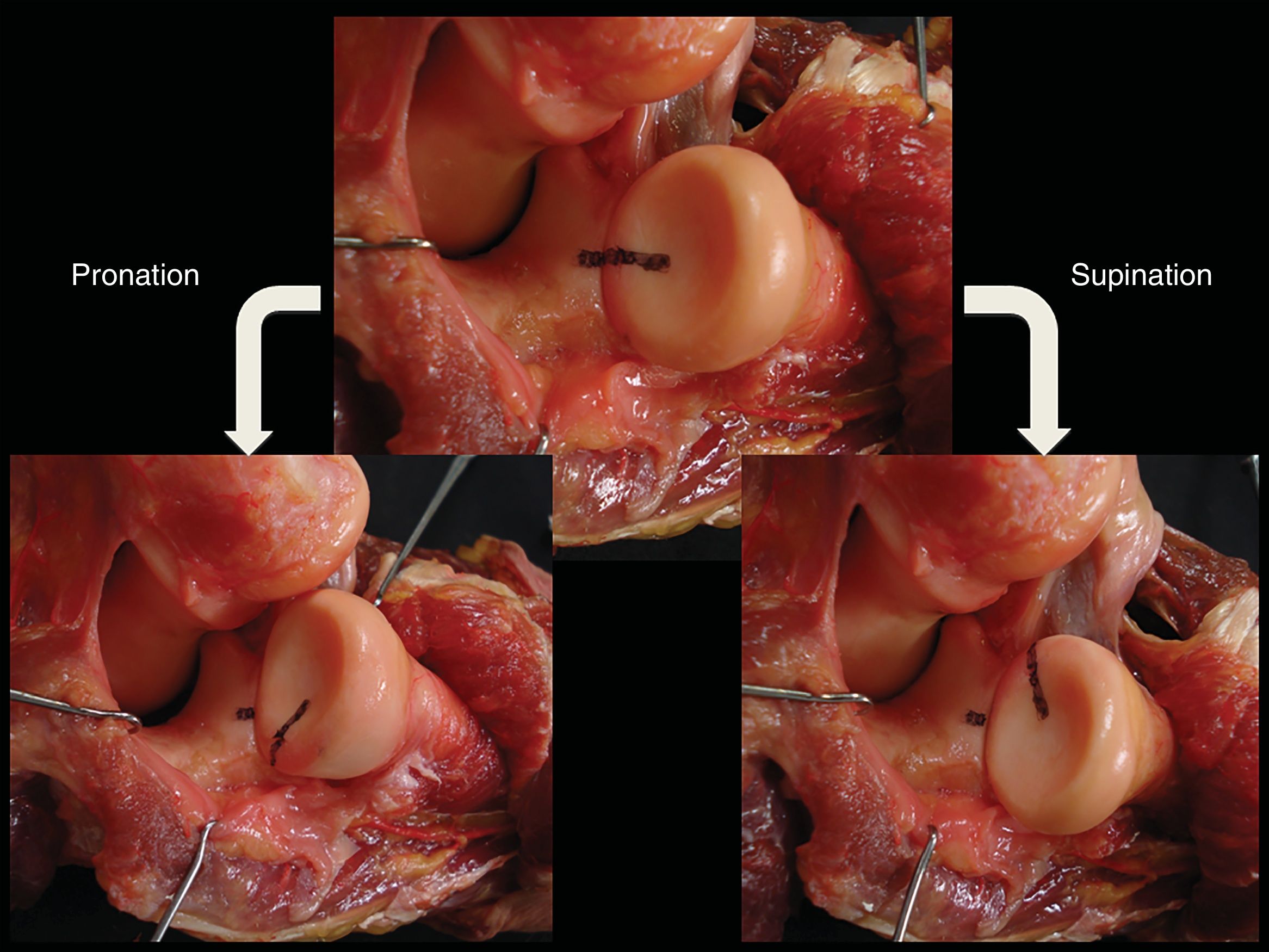
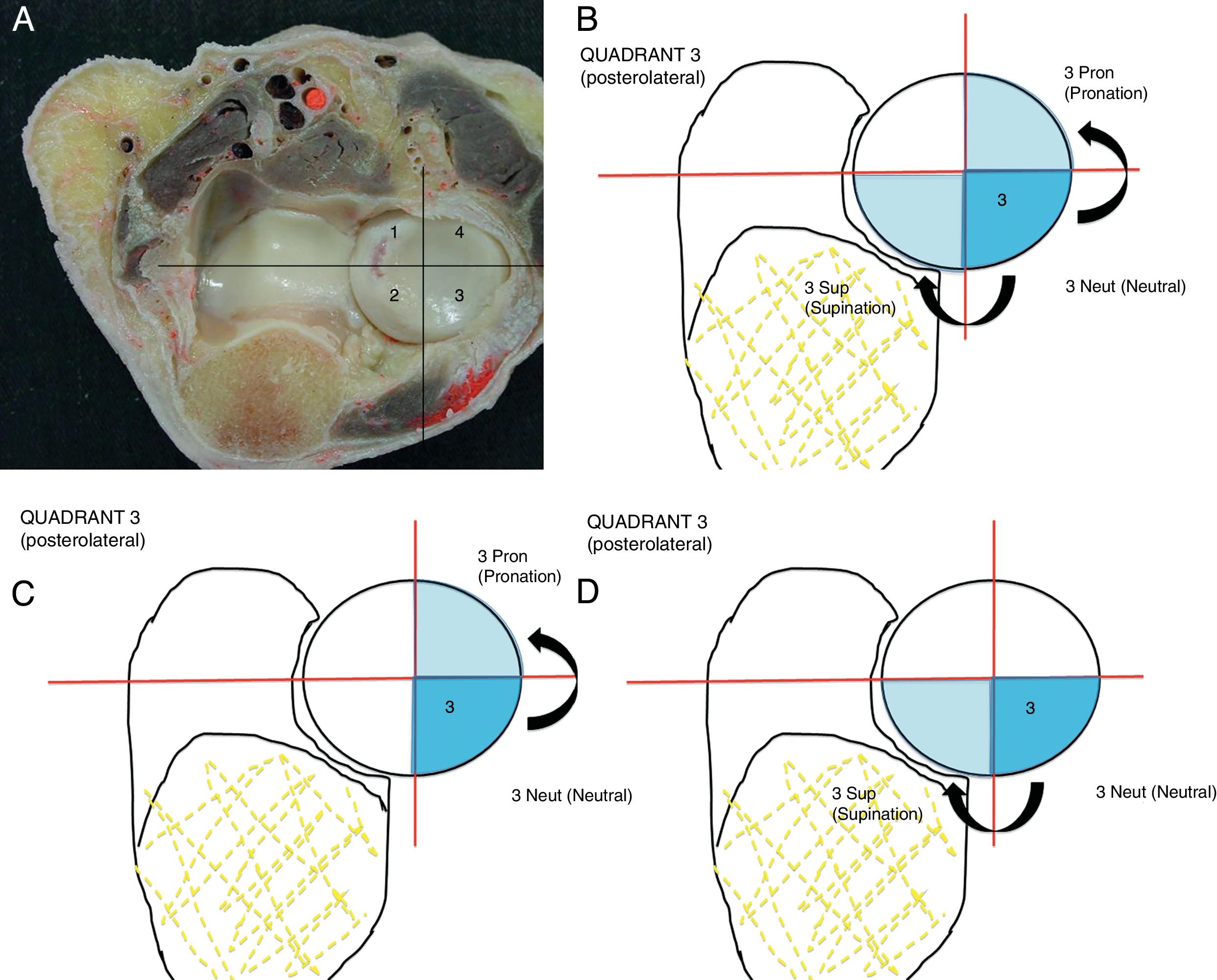
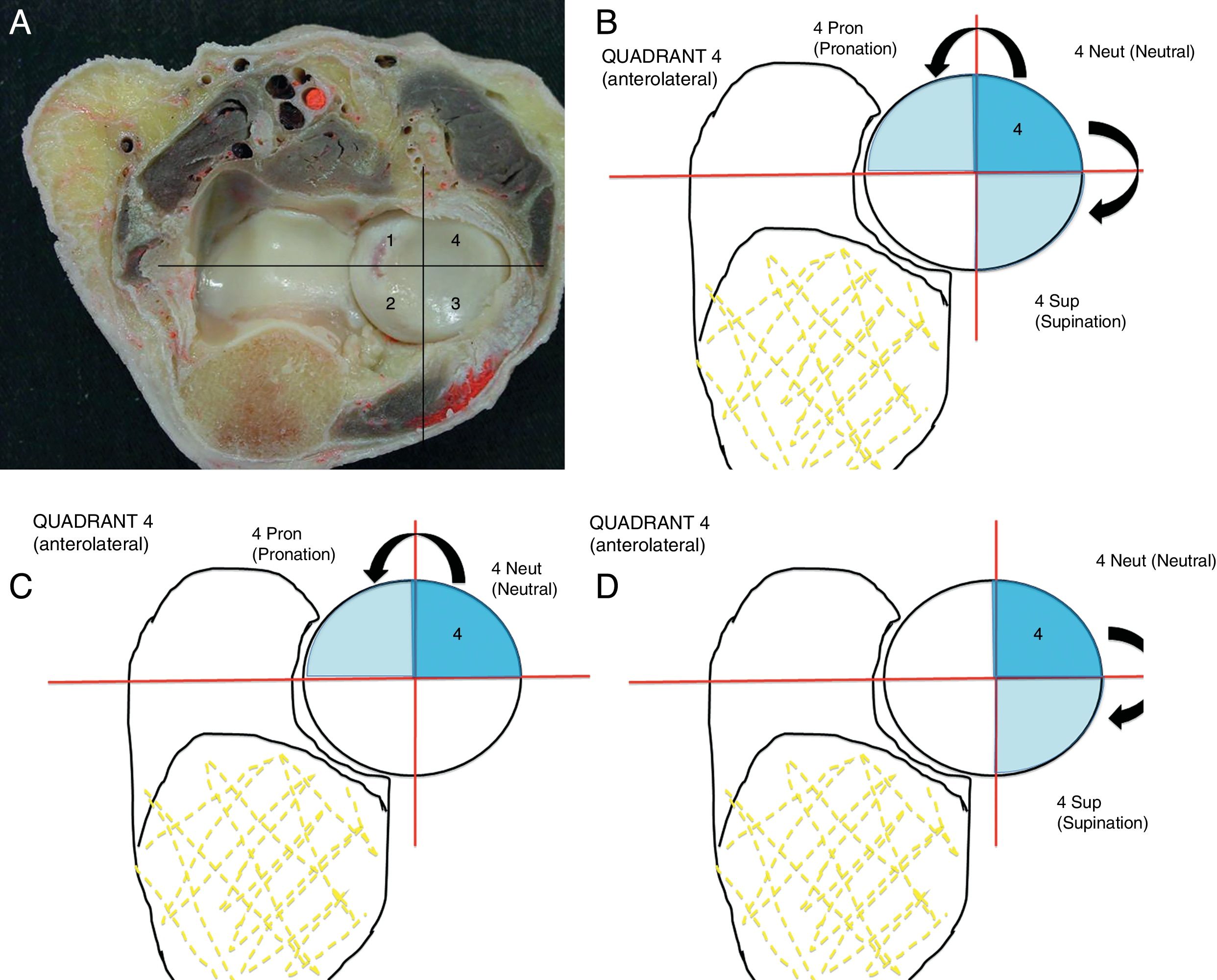
The radial head moves respecting the lesser sigmoid cavity due to pronosupination movements of the forearm, so that there are areas of convergence between the different quadrants (Fig. 2). This means that a quadrant may be approached from different portals. Fractures located in the anteromedial quadrant (1) require that forearm be in supination if they are to be approached through an arthroscopic portal. Quadrant 1 is inaccessible if the elbow is in neutral position or in pronation (Fig. 3A–D). The posteromedial quadrant (2) is very difficult to reach due to the lesser sigmoid cavity, which hides its exposure. It is necessary to work with the forearm in maximum pronation to access this quadrant. Quadrant 2 is inaccessible when the forearm is in neutral position or in supination (Fig. 4A–D). Fractures located in the posterolateral quadrant (3) may be approached through lateral portals, with the forearm in neutral position or in pronation. Nevertheless, this quadrant is not accessible in supination (Fig. 5A–D). Fractures located in the anterolateral quadrant (4) are accessible when the forearm is in neutral position or in supination. On the other hand, it is hard to access such fractures when the forearm is in pronation (Fig. 6A–D).

Right elbow, proximal and lateral view. The lateral musculoligamentous structures have been disinserted to better expose the proximal radiocubital joint. In this figure the horizontal axis that corresponds to the bicipital tuberosity has been marked with a felt-tip pen respecting the lesser sigmoid cavity of the cubitus. Note the displacement of the radial head respecting the lesser sigmoid cavity due to the pronosupination movement of the forearm. This means that a quadrant may be approached from different portals.
 Transversal proximal view of a right elbow, showing the proximal radiocubital joint and the association with neurovascular structures. (B) Location of the anteromedial quadrant (1) in neutral position respecting the lesser sigmoid cavity. (C) Fractures located in quadrant 1 require the forearm to be in supination for approach through an arthroscopic portal. (D) When in neutral position of the elbow and in pronation, quadrant 1 is inaccessible.")
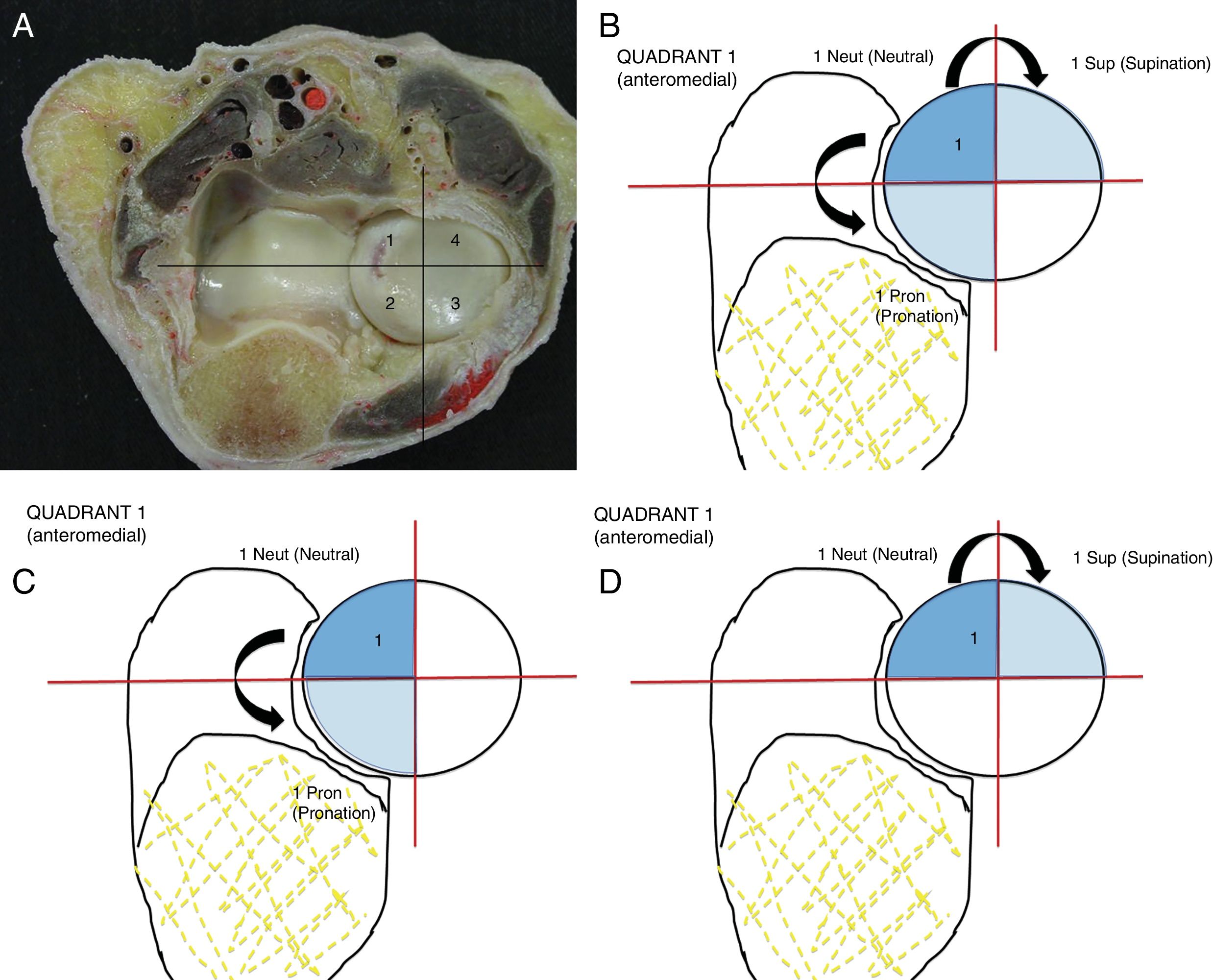
(A) Transversal proximal view of a right elbow, showing the proximal radiocubital joint and the association with neurovascular structures. (B) Location of the anteromedial quadrant (1) in neutral position respecting the lesser sigmoid cavity. (C) Fractures located in quadrant 1 require the forearm to be in supination for approach through an arthroscopic portal. (D) When in neutral position of the elbow and in pronation, quadrant 1 is inaccessible.
 Transversal proximal slice of a right elbow, showing the proximal radiocubital joint and the association with neurovascular structures. (B) Location of the posteromedial quadrant (2) in neutral position respecting the lesser sigmoid cavity. Quadrant 2 is very difficult to reach due to the lesser sigmoid cavity that hinders its exposure. (C) The forearm has to be in maximum pronation to access the quadrant. (D) Quadrant 2 is inaccessible when the forearm is in supination and in neutral position.")
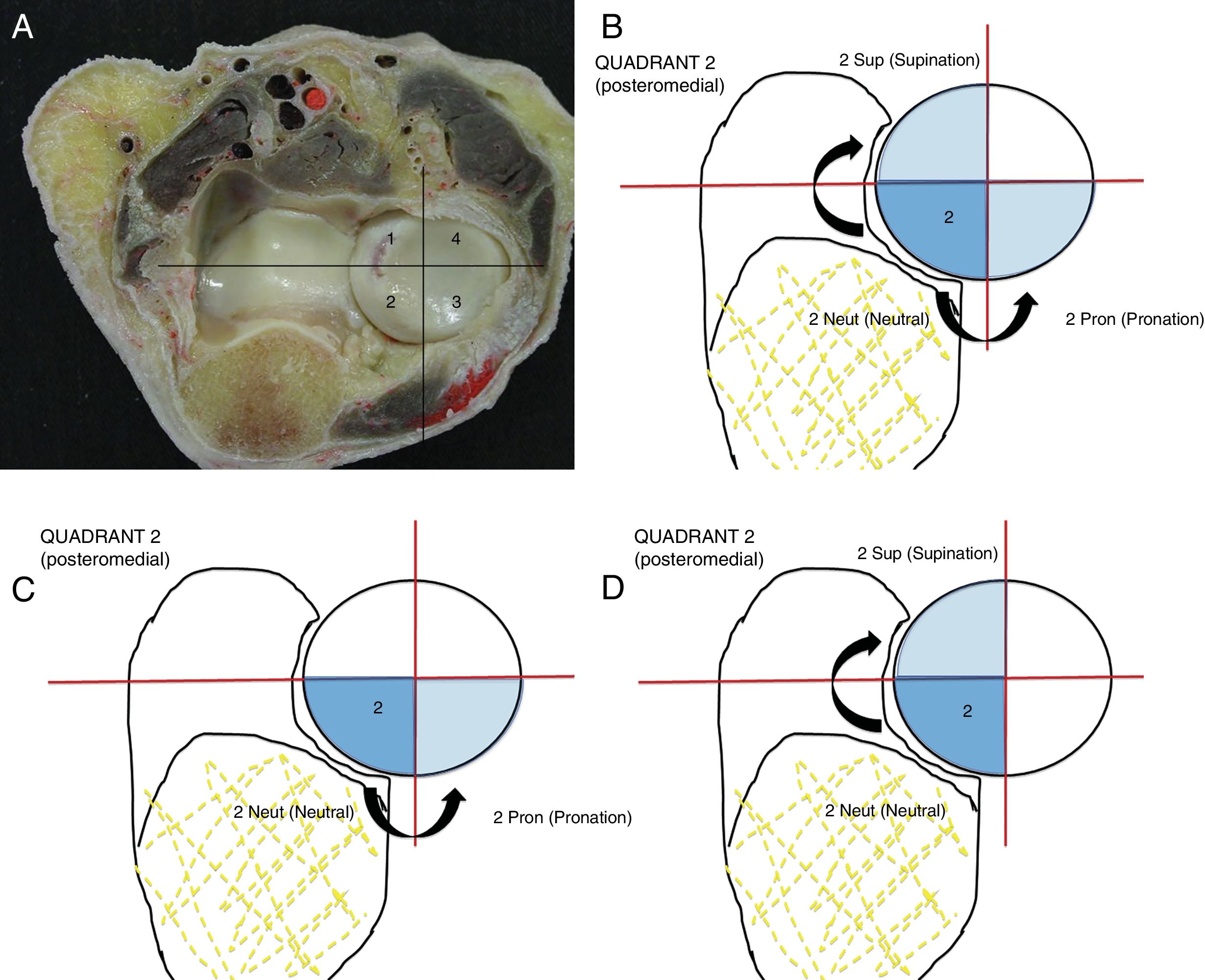
(A) Transversal proximal slice of a right elbow, showing the proximal radiocubital joint and the association with neurovascular structures. (B) Location of the posteromedial quadrant (2) in neutral position respecting the lesser sigmoid cavity. Quadrant 2 is very difficult to reach due to the lesser sigmoid cavity that hinders its exposure. (C) The forearm has to be in maximum pronation to access the quadrant. (D) Quadrant 2 is inaccessible when the forearm is in supination and in neutral position.
 Transversal proximal slice of a right elbow, showing the proximal radiocubital joint and the association with neurovascular structures. (B) Location of the posterolateral quadrant (3) in neutral position respecting the lesser sigmoid cavity. (C) The fractures located in quadrant 3 may be treated through lateral portals, with the forearm in neutral position and in pronation. (D) Nevertheless, in supination this quadrant is inaccessible.")
(A) Transversal proximal slice of a right elbow, showing the proximal radiocubital joint and the association with neurovascular structures. (B) Location of the posterolateral quadrant (3) in neutral position respecting the lesser sigmoid cavity. (C) The fractures located in quadrant 3 may be treated through lateral portals, with the forearm in neutral position and in pronation. (D) Nevertheless, in supination this quadrant is inaccessible.
 Transversal proximal slice of a right elbow, showing the proximal radiocubital joint and the association with neurovascular structures. (B) Location of the anterolateral quadrant (4) in neutral position respecting the lesser sigmoid cavity. (C) The fractures located in the anterolateral quadrant (4) are accessible with the forearm in neutral position and in supination. (D) Note how when the forearm is in pronation it is harder to access them.")
(A) Transversal proximal slice of a right elbow, showing the proximal radiocubital joint and the association with neurovascular structures. (B) Location of the anterolateral quadrant (4) in neutral position respecting the lesser sigmoid cavity. (C) The fractures located in the anterolateral quadrant (4) are accessible with the forearm in neutral position and in supination. (D) Note how when the forearm is in pronation it is harder to access them.
CT imaging of the elbow in cases of Mason II radial head fractures with an indication for surgery allows us to position the fracture in quadrants that are delimited respecting the bicipital tuberosity. The fact that a single imaging study of both structures is available (the radial head and bicipital tuberosity) makes the definition and location of the quadrants during preoperative planning more reliable than when we use a more distant reference element such as Lister's tubercle or the radial styloid. In these cases a CT image of the whole forearm may be taken to include the radial styloid or Lister's tubercle in the study, with the resulting unnecessary increase in patient exposure to X-rays, or it will be combined with a CT image restricted to the elbow with a clinically located external point of reference, with the consequent problematic lack of precision. We therefore believe that it is recommendable to take the bicipital tuberosity as the reference point when defining the areas of the radial head: they are very close and images of both may be obtained without increasing the radiological exposure of the patient.15
The results of this study show that fractures located in the anteromedial quadrant (1) require the forearm to be in supination if they are to be reached through an anteromedial arthroscopic portal. In neutral position of the elbow the quadrant is partially accessible, above all the most anterior part of the same; and in pronation quadrant 1 is inaccessible due to interposition of the lesser sigmoid cavity. It is very difficult to perform osteosynthesis in fractures located in the posteromedial quadrant (2) due to the lesser sigmoid cavity which hinders its exposure, as well as the proximity of the cubital nerve. It is necessary to work with the forearm at maximum pronation to access quadrant 2 from an anterolateral portal. Quadrant 2 is inaccessible when the forearm is in neutral position, while it is partially accessible in maximum supination: its most anterior part is exposed through an anteromedial portal. Fractures located in the posterolateral quadrant (3) may be treated through an anterolateral portal, with the forearm in neutral position or in pronation, increasing the risk of injuring the posterior interosseus nerve to the degree that we require more pronation. However, this quadrant is inaccessible with supination due to the interpositioning of the lesser sigmoid cavity. Fractures located in the anterolateral quadrant (4) are accessible when the forearm is in supination through an anteromedial portal as well as an anterolateral portal, and the forearm has to be in maximum supination. We could recommend that fractures in the most anterior part of quadrant 4 be treated through an anteromedial portal, and that fractures located predominantly in the most posterior zone of the said quadrant be treated through anterolateral portals. With the forearm in neutral position, the quadrant is in a hazardous position if an attempt is made to access it, given the proximity of the posterior interosseus nerve.
The treatment options for radial head fractures are usually conservative, with exeresis of the radial head, reduction and fixation of the fracture (using open or arthroscopy-guided reduction) and replacement with a prosthesis. Several classification systems have been described which have the aim of establishing a common language when describing the type of fracture, selecting the most unified possible treatment and also to give an idea of the prognosis for lesions. The fracture pattern classification used the most widely is the one by Mason, as modified by Hotchkiss.1,2 This classification is based on radiological aspects and clinical examination characteristics to seek associated lesions, and this improves the initial classification for decision-making. Hotchkiss recommends also performing CT imaging to obtain additional information about fragment size and displacement. A minimally displaced fracture (less than 2mm) without mechanical blockage may be treated conservatively, and it would correspond to type I. A fracture that can be reconstructed (that is not very comminuted, or which is in fewer than three parts) corresponds to type II, and it would have the indication of surgical treatment using reduction and internal fixation. A comminuted fracture that is impossible to reconstruct (more than three fragments) corresponds to type III, and it may be a candidate for prosthetic replacement or an exeresis, depending on its associated lesions and the patient.16
Depending on the Mason type II fracture pattern, in some cases it is necessary to use plates and screws, while in others only isolated screws are sufficient. Cannulated and headless screws have greatly facilitated the technique.17–19 Several authors have published good and excellent results of arthroscopically assisted internal fixation technique in Mason type II fractures, achieving similar results to those of the open reduction and internal fixation technique.4,20,21 The possibility of diagnosing and treating intra-joint pathology arthroscopically has significant advantages in comparison with open procedures. Close visualisation of the joint surface allows us to better comprehend the fracture pattern and facilitates highly accurate reduction.20,22 On the other hand, it allows us to evaluate associated lesions more exactly (capitellum or coronoid fracture, delaminations of the joint surface) while minimising lesions that an open approach may cause (disinsertion of the lateral ligament system or disinsertion of the extensosupinating musculature), which may improve postoperative evolution.23–25 The treatment of these fractures using arthroscopic fixation has other positive effects: shorter hospitalisation, reduced use of analgesia, lower radiological exposure of the patient and less need for secondary surgery in comparison with fixation by open reduction.7
Nevertheless, everybody knows that use of arthroscopic technique for fracture reduction and fixation generally involves a learning curve, and that it is technically demanding. Although fewer than 2% of complications are reported, neurovascular lesions are a complication that is greatly feared in elbow arthroscopy. The radial and poster interosseus nerves are structures which are exposed when the elbow is approached through anterolateral portals.26,27
The radial nerve runs almost adjacently to the joint capsule, anterior to the humeral-radial joint, and it changes position from medial to lateral depending on the movement from maximum pronation to maximum supination.11,28–30 This zone is one of the most exposed in arthroscopic procedures that treat radial head lesions. The median nerve and humeral vascular bundle are at risk in lesions approached through anteromedial portals, although it is also true that they are more “protected” anteriorly by the brachialis muscle.31,32 The cubital nerve is in danger when a medial proximal portal is made, above all in patients with surgery for previous elbow trauma, especially if the nerve has been transposed.33
ConclusionsIn Mason type II radial head fractures where surgery has been indicated as the best alternative, performing the osteosynthesis procedure assisted by arthroscopic technique leads to advantages for the patient. Preoperative classification of the type of fracture in the transversal plane by CT imaging study may be of great help, as we will be able to use the bicipital tuberosity as the reference point. With this study we show that each fracture pattern “requires” a certain arthroscopic portal, and therefore exposes certain neurovascular structures to different risks. The medial quadrants (anteromedial and posteromedial) are the most demanding in technical terms.
Level of evidenceLevel of evidence iv.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments took place for this research in human beings or animals.
Confidentiality of dataThe authors declare that no patient data appear in this paper.
Right to privacy and informed consentThe authors declare that no patient data appear in this paper.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Ballesteros-Betancourt JR, Lázaro-Amorós A, García-Tarriño R, Sastre-Solsona S, Combalia-Aleu A, Llusá-Pérez M. Clasificación del patrón transversal de las fracturas de la cabeza del radio tipo Mason II y su utilidad en la osteosíntesis mediante técnica artroscópica. Estudio anatomoquirúrgico. Rev Esp Cir Ortop Traumatol. 2019;63:12–19.
