




Infantile flexible flatfoot does not require treatment in most cases. Symptomatic flexible flat feet are treated orthopaedically and surgery is only indicated when orthosis fails.
Material and methodsCases who underwent surgical treatment with the stop screw technique at the 12 de Octubre Hospital between 1995 and 2002 are reported. Patient progress is also analysed. Six angles are measured on the X-ray prior to surgery and those same X-ray angles are measured again before material extraction. They are then compared to see if the correction achieved is statistically significant. A more reduced sample is currently being assessed with the same radiological measurements and two clinical assessment scales: Lickert, and Smith and Millar. The latest X-rays are analysed by two radiologists to determine if there is subtalar arthrosis.
ResultsIn the short term, statistically significant differences are observed in all angles. The comparison between the post-surgery angles and the current angles does not show differences, except for the Giannestras angle, which has statistically significantly worsened. Clinical results and patient satisfaction is good. Incipient subtalar arthrosis is present in 68.5% of current patient X-rays.
ConclusionsStop screw method is a cheap, simple and effective technique to correct symptomatic flexible flatfoot that has not improved with conservative treatment. This technique provides short-term foot correction which can be maintained over time.
El pie plano valgo flexible infantil no requiere tratamiento en la mayoría de los casos. Cuando son sintomáticos se tratan de manera ortopédica y si no se consigue mejoría se procede a la cirugía.
Material y métodosSe describen los casos operados en el Hospital 12 de Octubre con la técnica de calcáneo stop entre los años 1995 y 2002. Se valora también cómo están actualmente estos pacientes. Hemos medido 6 ángulos en la radiografía antes de la cirugía y en la radiografía posterior a esta, y se comparan los ángulos para sabre si la corrección conseguida es estadísticamente significativa. En el momento actual se valora una muestra más reducida de pacientes con las mismas mediciones radiológicas y escalas de valoración clínica: de Lickert, y de Smith y Millar. Las últimas radiografías son valoradas por 2 radiólogos para ver si existe artrosis subastragalina.
ResultadosA corto plazo se observan diferencias estadísticamente significativas en todos los ángulos. Comparando los ángulos poscirugía con los actuales se concluye que no hay diferencias, excepto en el ángulo de Giannestras, que ha empeorado de manera estadísticamente significativa. Los resultados clínicos y la satisfacción de los pacientes es buena. En las radiografías actuales hay artrosis subastragalina muy incipiente en el 68,5% de los pacientes.
ConclusionesEl calcáneo stop es una técnica barata, sencilla y eficaz para corregir el pie plano flexible infantil sintomático y que no haya respondido a medidas conservadoras. La técnica corrige el pie a corto plazo y esta corrección se mantiene en el tiempo.
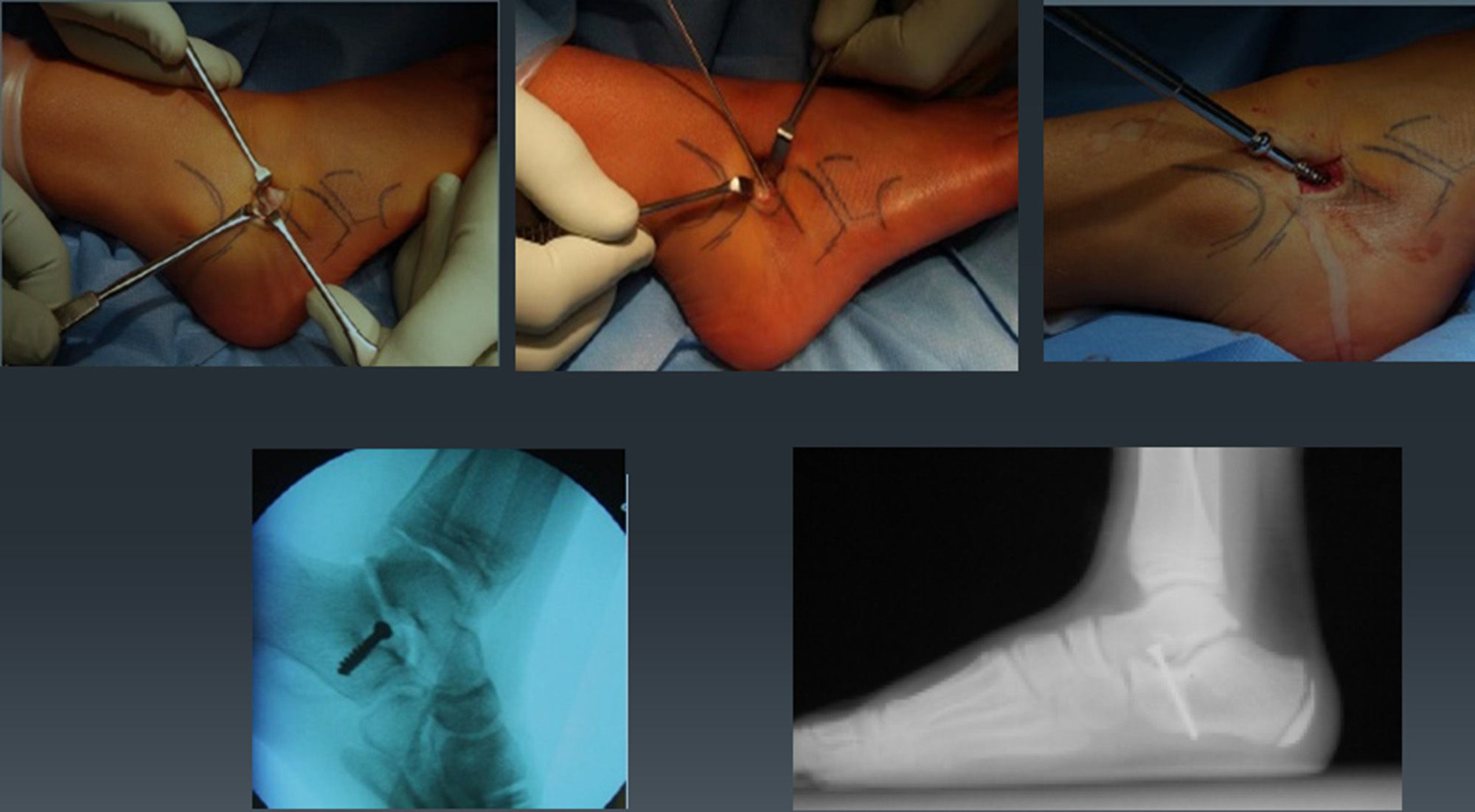
In 1976, Doctor Recaredo Álvarez described the calcaneal stop screw technique for the surgical treatment of symptomatic infantile flexible flatfoot. It is a simple technique, involving an arthroereisis, whereby a cancellous screw is introduced at the level of the tarsal sinus, in the posteroexternal subtalar (or subastragalar) aspect. About 1cm of the screw is allowed to protrude in the upper part, in order to act as a stop which passively blocks calcaneal pronation.
Infantile flexible flatfoot is physiological; it can be considered as a normal stage in the evolution of the foot which disappears spontaneously with growth.1
Several surgical techniques have been developed to treat this foot condition, but they are reserved for symptomatic feet causing pain and fatigue.2
The objective of this study is to evaluate the results obtained with the calcaneal stop screw technique in the short and medium-long term (over 10 years follow-up).
Material and methodsA total of 79 patients were intervened using the calcaneal stop screw technique at 12 de Octubre Hospital, in Madrid, between 1995 and 2002. Due to clinical and radiographic losses, only 52 histories could be reviewed, with a total of 103 idiopathic and flexible flat feet. We defined as flexible flat feet those presenting a decrease in the height of the plantar arch associated to forefoot supination and valgus hindfoot. It is called flexible because the foot regains the arch when standing on tiptoe or passively extending the first toe (Jack test).
All patients had both feet flat, except for 1 patient who only had 1. The symptoms reported were foot pain or fatigue. Initially, all patients followed a conservative treatment with insoles for at least 6 months.
The gender distribution was 20 girls and 32 boys. They were intervened at a mean age of 11.6 years (range: 7.11 to 14.8 years).
All patients had the screw extracted after a mean period of 23 months. The screw was extracted by protocol, as the aim was for the limitation of subtalar mobility to be temporary.
Flexible flatfoot is occasionally associated with short Achilles tendon and 3 of the patients required an extension of the Achilles tendon through a percutaneous Hooke technique.
Radiographic measurements were taken before and after the procedure, and patients were clinically and radiographically evaluated at the moment of measurement. All radiographs used for assessment were obtained under weight load.
Due to changes of address and telephone number, only 28 patients could be contacted. They underwent a telephone interview to know their level of satisfaction. A total of 18 patients (35 feet) also attended the hospital, after a mean period of 15 years and 8 months, and were examined clinically and radiographically.
The mean long-term follow-up period of these patients was 15.66 years (range: 13.61–17.72 years). The minimum follow-up period was 12 years and 1 month, and the maximum was 18 years and 9 months.
The angles measured in the radiographs were (Fig. 1):
- –
Internal Costa-Bartani: from the lowest point of the talar head, 2 lines are traced in 2 directions, one to the lowest point of the calcaneus and another to the lowest point of the head of the first metatarsal.
- –
Plantar flexion of the astragalus: axis of the astragalus and horizontal.
- –
Calcaneal-ground: tilt angle of the calcaneus with respect to the plane of the ground.
- –
Meary: formed by the intersection of the axes of the first metatarsal and the astragalus.
- –
Giannestras or talar-scaphoid: axis of the astragalus and line prolonging the joint interline between the scaphoid-2nd wedge.
- –
Talar-calcaneal or Kite: longitudinal axis of the astragalus and axis of the hindfoot.

We measured 6 angles in the radiographs obtained before the intervention.
Those same angles were then measured in the postoperative radiographs obtained before extracting the screw.
The current situation was clinically and radiographically evaluated. The clinical assessment was carried out by telephone, applying the Lickert satisfaction scale. This consists in assigning an overall score to the feet (aesthetics, pain, etc.), through a numerical value ranging from 1 to 4 to represent:
- 1.
Very satisfied
- 2.
Satisfied
- 3.
Mildly satisfied
- 4.
Dissatisfied
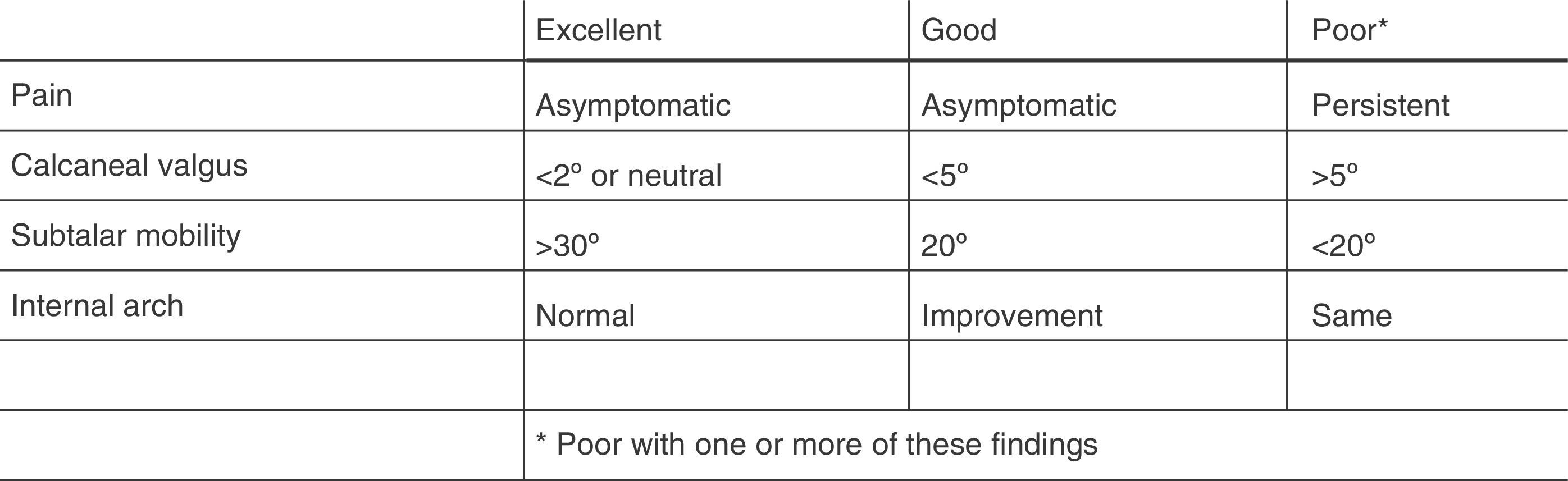
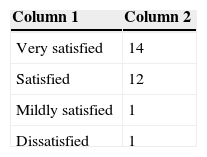
A total of 28 patients responded to this telephone survey. Of these, 14 were very satisfied, 12 were satisfied, 1 was mildly satisfied and 1 was dissatisfied (Table 1). The dissatisfied patient also presented developmental hip dysplasia and the telephone survey was responded by his mother. In contrast, he did present adequate angle correction. After responding to the telephone survey, patients were asked to attend the clinic for a new clinical and radiographic evaluation. A total of 18 patients did attend the hospital, and their current situation was assessed by means of the Smith and Millar scale, which measures pain, calcaneal valgus, subtalar mobility and internal arch (Fig. 2). According to this scale 8 patients reported an excellent result, 9 a good result and 1 a poor result (Table 2). This poor result was due to the fact that the patient reported suffering pain almost daily (the same patient whose mother gave a score of 4 in the Lickert scale). A new radiograph was also obtained, in which the same angles were measured once again.

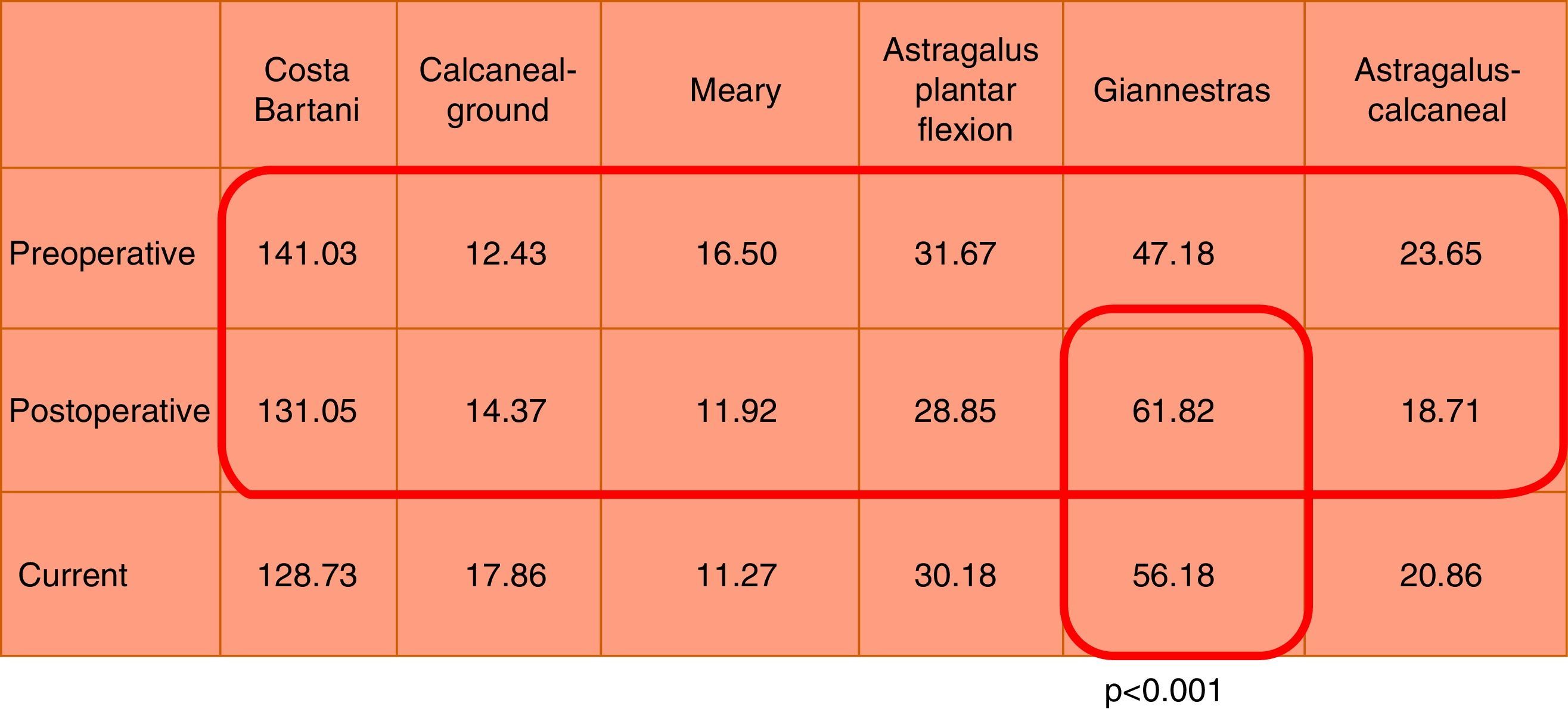
The radiographic angles of the 103 feet (52 patients or histories) measured were compared with the angles measured in the postoperative radiographs, prior to extracting the screw (also 103 feet). These latest measurements were compared with the measurements in the current radiograph (a total of 35 feet, from 18 patients). The statistical assessment was carried out by means of a nonparametric Wilcoxon t test, which detected statistically significant differences (P<.001) between all the angles before and after the procedure. The test compared the angles obtained after the surgery (103 feet) with the angles measured at the current moment (18 patients, 35 feet). This last assessment did not detect statistically significant differences, except in the Giannestras angle, which did display them (Fig. 3). The Giannestras angle decreased in a statistically significant manner, which meant that some of the correction was lost over time. In other words, the feet currently had more talar valgus than after the surgery. Given that the remaining angles did not display any statistically significant differences, it can be said that the correction was maintained over time.

The current radiographs (18 patients, 35 feet) were passed to 2 paediatric radiologists who evaluated the existence or absence of subtalar osteoarthritis. Based on the Kellgren and Lawrence radiographic classification of osteoarthritis, the specialists concluded that 11 feet had osteoarthritis grade 0, 12 feet had osteoarthritis grade 1 and 12 feet had osteoarthritis grade 2.
The complications described in the histories were 10 reinterventions: 4 due to a change in the location of the screw, which was not in the expected position when the postoperative control radiograph was obtained, and 6 due to excessively long screws. There was 1 case of superficial infection, which was resolved with antibiotic treatment. There were no cases of screw tear or screw extractions due to intolerance.
DiscussionFlexible flatfoot in children is physiological. It can be considered as a normal stage in the evolution of the foot, which disappears spontaneously with growth. Coll3 demonstrated that 85% of these feet become normalised spontaneously between the ages of 5 and 7 years. About 10–15% of cases persist into adulthood and the majority are asymptomatic. Moreover, Rao and Joseph4 conducted a study comparing children who wore closed shoes or sandals with another group that went barefoot, and observed a higher prevalence of flat feet in children wearing shoes compared to those who went barefoot.
Orthopaedic treatment with insoles is more functional than corrective, but most authors coincide in applying orthopaedic treatment for a certain period of time in an attempt to correct the deformity and, especially, to reduce the pain.
Surgical treatment is rarely indicated in true flexible flatfoot.
Surgical techniques are reserved for symptomatic feet causing pain and fatigue, and which have not improved with orthopaedic treatment.5
Surgical treatment offers 3 possibilities: arthroereisis, arthrodesis and osteotomy. There is no clear method available to ensure an adequate correction of flatfoot in children.6 Arthroereisis is a technique used to limit valgus movement of the subtalar joint, maintaining the astragalus in a corrected position.7 It should be associated to a percutaneous extension of the Achilles tendon if this is retracted. The calcaneal stop screw technique entails creating a 2–3cm incision in the tarsal sinus and forcing supination until reaching the posteroexternal subtalar aspect, where a cancellous screw is introduced, crossing 2 calcaneal cortices at an angle of 35° in the sagittal plane and 45° in the coronal plane.2–8 This screw is left to protrude by 1cm in order to act as a stopper to block calcaneal pronation (Fig. 4). Arthroereisis corrects the foot in all 3 spatial planes, but the most significant improvement is in the frontal plane.9 Arthroereisis has gained popularity because it eliminates excessive pronation whilst preserving preoperative inversion and adaptation of the forefoot and hindfoot to uneven terrains.10 There are different variations in the application of this concept: Judet fixed the talar head with the calcaneus after reducing the deformity, Giannini used an expansible Teflon prosthesis, whilst Smith and Millar used a polyethylene implant and Viladot a Silastic prosthesis.11

The Kalix-type endorthesis yielded similar results to those obtained in this study in terms of angle correction and patient satisfaction. Fernández de Retana et al. had to remove certain endorthesis due to intolerance.12
The short term results obtained with the calcaneal stop screw technique are similar to those observed with other arthroereisis methods.13
This procedure is indicated at ages between 9 and 13 years, as there has been sufficient joint remodelling and because there still exists a potential for growth and joint modification which allows the relationship between the astragalus and calcaneus to be restored.14 Operating on excessively young patients may lead to the development of cavovarus foot deformity.
The screw is removed after a mean period of 2 years, as this is the necessary period for remodelling of the astragalus, calcaneus and subtalar joint. Patients operated after an age of 12 years may not have sufficient time for the remodelling of the hindfoot.12 The calcaneal stop screw technique is economical, simple and effective to correct symptomatic flexible flatfoot in children who have not responded to conservative measures.15
In our study we were able to demonstrate that the correction obtained is maintained over time, even though some of the initial talar valgus correction was lost. During a period of over 15 years, the Giannestras angle went from an initial mean value of 61.82° (measured in 103 feet) to a mean current value of 56.18° (measured in 35 feet).
De Pellegrin et al.16 observed an improvement, albeit not a statistically significant one, in the calcaneal-ground angle after a follow-up period of 2.9 years compared to the calcaneal-ground angle after the surgery, thus concluding that the correction obtained was progressive, effective and maintained over time.
In our study we observed low grade subtalar osteoarthritis in the current radiographs in 22 patients (68.5%), although this was not observed at a clinical level. Further studies with a longer follow-up period would be required in order to verify if the level of osteoarthritis evolved and whether it manifested clinically.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation does not require experiments on humans or animals.
Confidentiality of dataThe authors declare that this work does not reflect any patient data.
Right to privacy and informed consentThe authors declare that this work does not reflect any patient data.
Conflict of interestsThe authors have not received any financing to carry out the present work and have no conflict of interests to declare.
Please cite this article as: Calvo Calvo S, Marti Ciruelos R, Rasero Ponferrada M, González de Orbe G, Viña Fernández R. Más de 10 años de seguimiento de la técnica de calcáneo stop. Rev Esp Cir Ortop Traumatol. 2015;60:75–80.
