




Onychomycosis denotes fungal infection of the nail characterized by thickening, splitting, roughening and discoloration of nail and accessory structures due to dermatophytes, non-dermatophyte moulds and few yeast genera.2 Onychomycosis can have a lasting adverse impact on patient's daily life, social functioning, physical and mental health; items collectively termed as “Quality of Life”.5 The predisposing factors range from advancing age, trauma, geo-climatic conditions, occupation, social class, immune status of the host and associated superficial mycoses like tinea pedis.1,3 Naildex score first applied by Warshaw et al.6 was used in this study to understand the burden of onychomycosis in agricultural workers in a rural community setting, and to assess the disease severity.
The study was conducted during October 2007 to October 2008 including three coastal villages in Karnataka, Southern India. 42 patients with clinical features of onychomycosis were screened for the disease. The nail and adjacent area was cleaned with 70% alcohol before collection with a nail clipper and tweezers onto pre-sterilized black kraft paper and portioned for KOH-calcofluor microscopy and fungal culture. The nail segments were briskly dipped in methanol to remove any bacterial contaminant and inoculated on Sabouraud dextrose agar with chloramphenicol and cycloheximide and Sabouraud dextrose agar with chloramphenicol and incubated at 28°C for 3 weeks. Identification of the filamentous/yeast fungi was done based on the macroscopic and microscopic features as per the standard mycological methods. A repeat sample was procured from all those patients who were both microscopy and culture positive case for confirmation of onychomycosis and Naildex score was recorded.
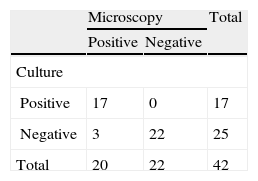
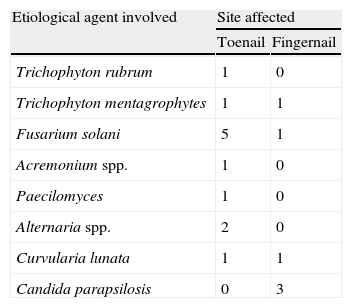
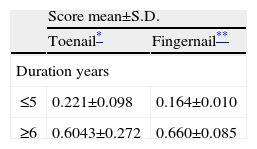
Among the 42 patients screened, 17 were positive by microscopy and culture, and 20 positive by microscopy alone. This included 13 females and 4 males. The results of microscopy and culture positive cases are shown in Table 1. The mean age of the females was 52 years and of the males was 49 years. Distal lateral subungual onychomycosis was seen in 9 patients, and 8 patients presented with total dystrophic onychomycosis. Toenails alone were affected in 10 patients, and fingernails only in 6 patients. Toenails and fingernails both were affected in 1 patient. The commonest isolate from the toenails was Fusarium solani, and that from the fingernails was Candida parapsilosis (Table 2). Naildex score was calculated for patients who yielded a positive microscopy and culture result. Mean of the scores – toenail and fingernail – was compared with the duration of the disease by the Independent Sample t-test, as depicted in Table 3.
Etiological agents involved with confirmed cases of onychomycosis
| Etiological agent involved | Site affected | |
| Toenail | Fingernail | |
| Trichophyton rubrum | 1 | 0 |
| Trichophyton mentagrophytes | 1 | 1 |
| Fusarium solani | 5 | 1 |
| Acremonium spp. | 1 | 0 |
| Paecilomyces | 1 | 0 |
| Alternaria spp. | 2 | 0 |
| Curvularia lunata | 1 | 1 |
| Candida parapsilosis | 0 | 3 |
Various scoring methods have been devised to study the disease severity like the Planimetry method and the Global evaluation method.4 The Planimetry method is tedious and time consuming and it cannot distinguish minimal residual disease from cure. Both methods are imprecise.6 An increase in the score with an increase in duration of the disease was also seen in study done by Warshaw et al.6
This study highlights the burden of onychomycosis among agricultural workers in a rural setting. The Naildex scoring method is rapid and inexpensive and may have a significant role for testing new drugs in clinical trials and also may be used to assess the response to treatment of onychomycosis.

