




Disseminated invasive aspergillosis is an exceptional finding in immunocompetent hosts. As in immunocompromised patients, it has high mortality rates. Early diagnostic methods are required in order to properly manage the patient. Bis(methylthio)gliotoxin (bmGT) is a novel biomarker, useful in onco-hematological patients.
Case reportA 70-year-old male, with non-insulin dependent type II diabetes mellitus and a past surgery history of aortic valve replacement with coronary by-pass five years ago, was seen in the emergency department with blurred vision. Three days later, endogen endophthalmitis was diagnosed in the ophthalmology clinic. During admission for the vitrectomy, he suffered an ischemia of the right lower limb. A thoracic computed tomography revealed a mycotic aneurysm of the ascending thoracic aorta and parietal thrombus. The ascending aorta was replaced and abundant brittle material of infectious appearance, found between the aortic valve graft and the aneurysm, was removed. Aspergillus fumigatus sensu stricto grew in both vitreous and aorta cultures. BmGT was detected in two serum samples obtained prior to intravenous antifungal treatment, which was then reduced after voriconazole treatment was started.
ConclusionsDisseminated invasive aspergillosis is a severe disease regardless of the immune status of the patient. This case report suggests that bmGT could be a suitable early diagnostic biomarker, not only in neutropenic patients, but also in immunocompetent hosts.
La aspergilosis diseminada invasiva es un hallazgo excepcional en pacientes inmunocompetentes, y al igual que en los pacientes inmunodeficientes, alcanza valores de mortalidad elevados. Para el correcto manejo del paciente son necesarios métodos diagnósticos precoces. La bis(metiltio)gliotoxina es un nuevo biomarcador de gran utilidad en pacientes oncohematológicos.
Caso clínicoVarón de 70 años de edad con diabetes mellitus tipo II no dependiente de insulina y antecedente de recambio valvular aórtico con by-pass coronario cinco años antes, que acude al Servicio de Urgencias por visión borrosa. Tres días después se le diagnosticó endoftalmitis endógena en la consulta de Oftalmología. Durante su ingreso para la vitrectomía presentó una isquemia del miembro inferior derecho. La tomografía computarizada de tórax reveló un aneurisma micótico en la aorta torácica ascendente y un trombo parietal. Se reemplazó la aorta ascendente y se eliminó abundante material friable de aspecto infeccioso entre la prótesis valvular aórtica y el aneurisma. En los cultivos de humor vítreo y aorta creció Aspergillus fumigatus sensu stricto. Se detectó bis(metiltio)gliotoxina en dos muestras de suero obtenidas antes del tratamiento antifúngico intravenoso, marcador que disminuyó tras comenzar el tratamiento con voriconazol.
ConclusionesLa aspergilosis diseminada invasiva es una enfermedad grave independientemente del estado inmune del paciente. Este caso clínico evidencia que la bis(metiltio)gliotoxina podría ser un marcador diagnóstico precoz no solo en pacientes neutropénicos, sino también en huéspedes inmunocompetentes.
Invasive aspergillosis (IA) is the most frequent filamentous fungal disease in immunocompromised patients. Immunosuppressed hosts get infected by conidial inhalation, and pulmonary aspergillosis is the most frequent clinical presentation. Dissemination occurs from the lungs by hyphal invasion.3 Although IA generally occurs in immunosuppressed patients, it may also rarely be diagnosed in immunocompetent individuals.2 In these cases pathogenesis usually occurs by direct conidial inoculation after trauma. Nosocomial acquisition can also occur due to airborne contamination during operation.11 IA is associated with high mortality rates (around 80%) in immunosuppressed and immunocompetent patients.6,11 Diagnosis is difficult in both populations but while serum galactomannan (GM) detection has demonstrated to be a useful tool in neutropenic patients, it seems to be less sensitive in the case of immunocompetent individuals.10 Our group has previously found that bis(methylthio)gliotoxin (bmGT), the inactive derivative of the virulence factor gliotoxin (GT), can be detected in serum samples from immunosuppressed patients at risk of IA.5,13 Here we report the first case of disseminated (aorta and vitreous) invasive aspergillosis in an immunocompetent patient with detectable serum bmGT. Pending larger studies, this case is the first example that reveals the utility of bmGT in the diagnosis of IA regardless of the immune status of the patient.
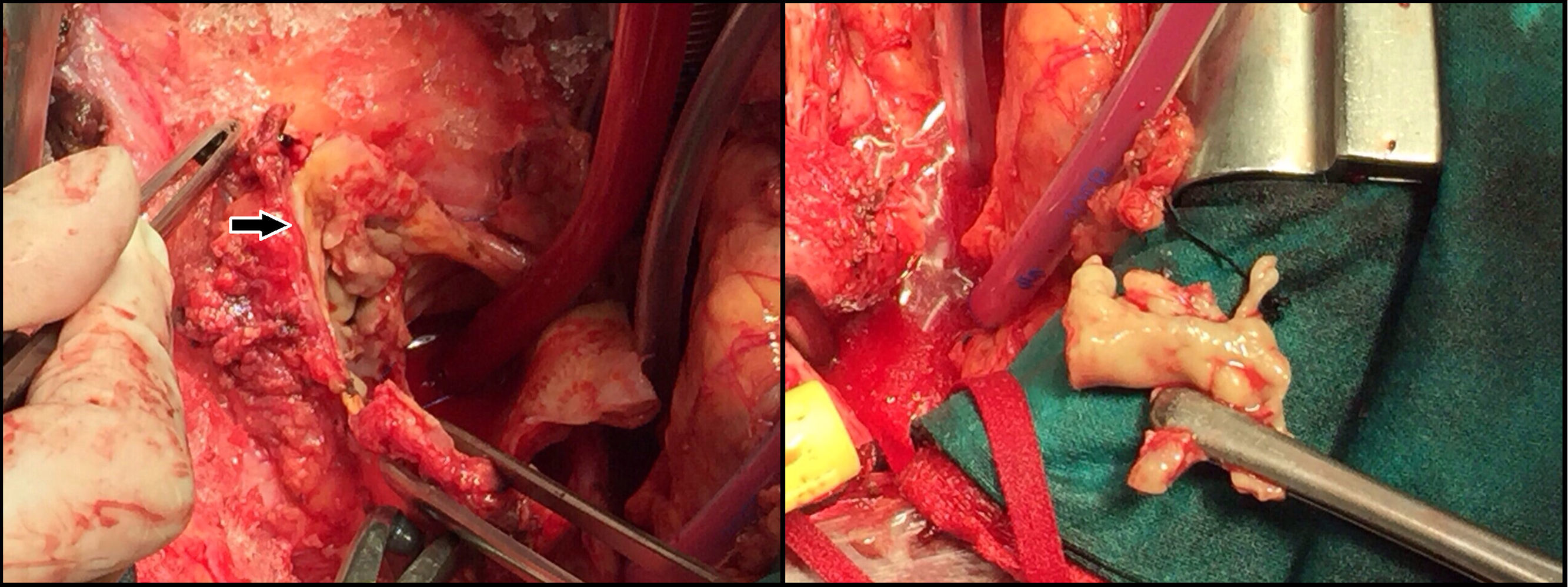
Case reportA 70-year-old male with non-insulin dependant type II diabetes mellitus and a surgery history of aortic valve replacement with a coronary by-pass five years before and hip replacement three years before, presented to the emergency department with blurred vision. Ophthalmological examination of the left eye showed positive Tyndall effect and turbid vitreous. Uveitis was diagnosed and topic corticosteroids were prescribed. Three days later he was re-evaluated in ophthalmology consultation where endogen endophtalmitis was diagnosed and vitrectomy was planned. During the intervention, vitreous was sent for microbiological examination and intravitreous therapy with vancomycin and voriconazole (VOR) was administered. Intravenous vancomycin (1g/12h) was also administered. During his admission for the surgery, the patient suffered an ischemia of the right low member. Computed tomography (CT) and an angiography of peripheral arteries and thorax showed a right pedis artery occlusion and a thrombus in aortic arch associated to a small dissection. The patient received intraarterial fibrinolytic treatment, and the aortic lesion study continued. Infectious endocarditis was then ruled out by transesophageal echocardiography. A thoracic CT revealed mycotic aneurysm of the ascending thoracic aorta, including mural thrombus. Antibiotic treatment was empirically initiated with daptomycin (10mg/kg/d), cloxacillin (4g/4h) and gentamicin (240mg/12h), and graft replacement of the ascending aorta was carried out. During the surgery abundant brittle material of infectious aspect, found between the aortic valve graft and the aneurysm, was removed (Fig. 1). Samples were sent for histological and microbiological examination. The same day the microbiological report revealed the presence of hyphal elements on the Gram stain, a new treatment with caspofungin (70mg/d on day 1, followed by 50mg/d) started. The next day, Aspergillus fumigatus was isolated and VOR (6mg/kg every 12h on the first day, followed by 4mg/kg every 12h) was added to the treatment.

After the surgery, the clinical state of the patient was stable and extubation was possible. He only presented a mild renal impairment. Later on, the patient developed severe respiratory failure and intubation was needed again. He gradually got worse, with severe renal impairment requiring continuous venovenous hemodiafiltration and vasoactive drugs. The patient developed finally a septic shock with respiratory, renal and hepatic failure, and died.
Histopathological examination demonstrated an abscessified aortic wall with fungal structures. A. fumigatus grew in both vitreous and aorta cultures. The isolates were sent for their identification and antifungal susceptibility testing to the National Microbiology Center (NMC). A. fumigatus sensu stricto identification was informed; minimum inhibitory concentration to VOR was 1μg/ml (sensible). Despite fungal isolation in vitreous, a complete toxoplamosis investigation was carried out. Serology showed positive Ig M and Ig G, with a positive Ig G avidity test. Vitreous was also sent to the NMC and Toxoplasma gondii PCR was performed with a negative result.
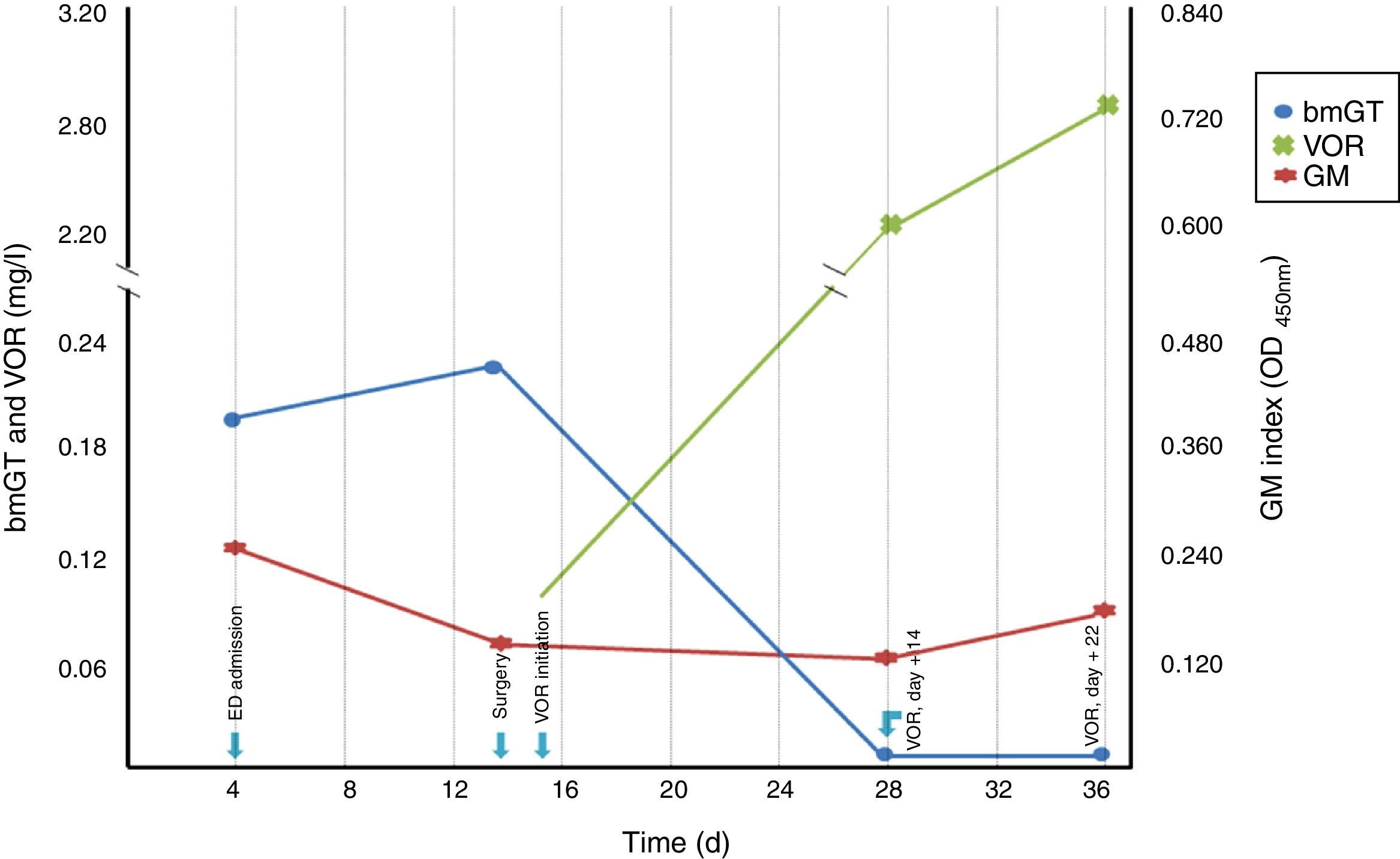
Four serum samples were analyzed for GM, bmGT, GT and VOR detection: (i) a serum obtained for toxoplasmosis investigation, (ii) the serum obtained prior to aortic surgery, (iii) a serum obtained after 14 days of correct antifungal treatment, and (iv) a serum obtained after 22 days of treatment. Results are shown in Figure 2. GM index was below 0.5 in all the four sera collected. GT was also undetectable in the four sera. Conversely, bmGT was detected in the two samples obtained prior to intravenous antifungal treatment.
Conclusionsgliotoxin (bmGT) concentration, voriconazole (VOR) concentration and GM index throughout time.")
Disseminated invasive aspergillosis is a rare entity among immunocompetent patients. In a recent literature review performed by Cheon et al., the most frequently reported port of entry was the lungs.2 In our case, the most probable focus of infection was the aortic valve replacement performed five years before. Pasqualotto et al., in an excellent literature review, reported that post-operative aspergillosis is an under-appreciated problem.11 Both authors highlighted the need of rapid diagnostic methods and antifungal therapy instauration. It is well known that GM is an early biomarker of IA in neutropenic patients8 and can guide antimould treatment.9 However, its utility among immunocompetent hosts has been questioned as Aspergillus antibodies can interfere with this immunoassay and GM can be uptaken by cells of the reticuloendothelial system.10 Thus, better diagnostic methods are required11; this could be the case of bmGT. BmGT is an inactive derivative of GT, a well known virulence factor of the genus Aspergillus. GT has been proposed as an IA biomarker.1,7,12 Nevertheless, the disulphite bridge present in its structure makes it very unstable and it is rapidly cell associated and removed from body fluids.14 Conversely, bmGT is a more stable inactive metabolite produced by the blockage of the disulphide bond present in GT by methylation.4 It can be reliably detected in serum of patients at-risk of IA and has a good diagnostic performance.5,13 However, its utility in other populations is unknown. In light of the above described case in which bmGT was early detected before patient was treated, then decreased after VOR treatment, it seems that bmGT could be a useful diagnostic tool regardless of the immune status of the patient. Even if conclusions cannot be drawn from a single case, this finding significantly advances our knowledge about potential markers for IA and supports further research.
Conflict of interestM.P. Domingo, J. Pardo and E.M. Gálvez are coinventors of a patent licensed to Blackhills Diagnostics Resources S.L. that protects the use of bmGT to diagnose IA (PCT/EP2012/058247). All the other authors declare that they have no competing interests.

