






A 19 year-old man presented with a 10-day history of painful erythematous tumefaction on the left groin, with pustules, bald areas and erythematous-desquamative plaques on the pubis (Fig. 1). The patient had low-grade fever, general malaise and bilateral adenopathy. He had recently had unprotected sexual intercourse, and he remembered that the woman had a cutaneous lesion in the genital area. Serology for syphilis, HCV, HBV, HIV, and HSV were negative.

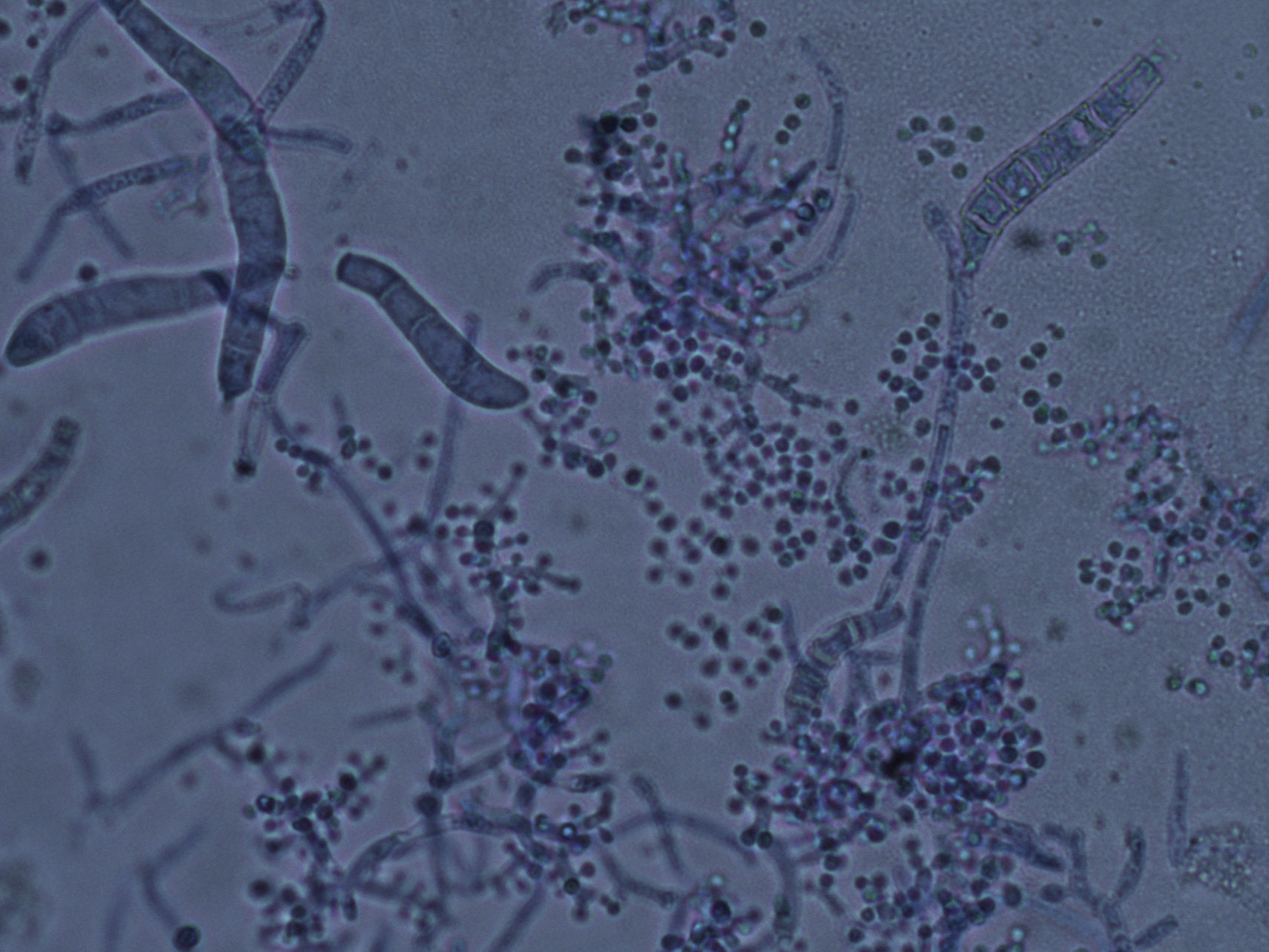
Microscopic examination of the purulent exudate was undertaken, revealing the presence of multiple hyphae (KOH, 400×) (Fig. 2). Trichophyton mentagrophytes was isolated in culture (Figs. 3 and 4). Colonies on Sabouraud dextrose agar had a granular texture, with a white to cream color on the front and a yellowish one on the reverse. Microconidia were round and organized in closely rebranched clusters; macroconidia were multiseptate with thin and small walls. Urease test was positive. Hair perforation test was positive. On Potato dextrose agar the colonies were white on the reverse.
.")
.")
.")
The patient was treated with a 6-week course of oral terbinafine, 250mg/day, with complete remission of the symptoms and no recurrences during the following year. Kerion Celsi is an inflammatory variant of tinea capitis or tinea barbae which is usually caused by zoophilic species.2 It is often confused with bacterial abcesses and its course may be favored by wrong treatments.1 The gold standard—fungal culture—plays a crucial role in the early recognition of any dermatophyte infection. Kerion Celsi on the genital area1,4–6,8,10 or on the pubis1,5,8 is an exceptional location and it may represent a rare sexually transmitted condition, requiring early diagnosis. The involvement of pubic and/or genital areas in dermatophytoses is usually linked to the spreding of tinea cruris lesions.3,7 However, recently published case series by Luchsinger et al. described tinea genitalis as a new entity of sexually transmitted infection.8 Connubial tinea gladiatorum9 have been reported recently among commercial sex workers.8 On the basis of the patient's history, an indirect route of transmission can be hypothesized in our case.
Dermatophytic suppurative lesions may be easily misdiagnosed as bacterial infections. Differential diagnosis of adenopathy and tumefaction on the groin should include chancroid, lymphogranuloma venereum, and granuloma inguinale. However, suppurative lesions, fever, adenopathies and alopecia in the pubic area should lead to the suspicion of Kerion Celsi (Fig. 1). In the distinction with Majocchi's granuloma it is useful the intradermal reaction with trichophytin, which is strongly positive in the Kerion Celsi and weak in the Majocchi's granuloma. The histology shows granulomatous inflammation, with few fungal elements in Majocchi's granuloma, and abundant fungal elements in Kerion Celsi.
Oral administration of terbinafine for 4–6 weeks is the preferred treatment in immunocompromised and non-immunocompromised patients. Systemic administration of antifungal agents is mandatory because topical application alone is usually ineffective. In order to avoid irreversible scarring alopecia, prompt initiation of antifungal treatment is essential along with an adequate isolation and identification of the pathogen.8
Conflict of interestThe authors have not conflict of interest

