


There are multiple congenital structural abnormalities that affect male urogenital tract which could affect either the male external genitalia, internal genitalia or both. Congenital anomalies of the vas deferens may be unilateral or bilateral that could be complete or segmental and include (agenesis, atresia, duplication, ectopy or diverticulum). Anomalies of the vas deferens may be isolated or may be associated with other congenital anomalies especially in the male urogenital tract. These rare vas anomalies may be discovered during genital examination (either clinically or radiologically) or even accidentally during inguinal surgeries as in varicocelectomy, hernia repair, vasectomy or orchiopexy. We hereby reported the first case of triple vas deferens in a 35-year-old male that was felt on spermatic cord examination and confirmed by trans-rectal ultrasonography. Thus, proper evaluation should be made for the cases of multiple vas deferens to avoid the accidental injury during the operation and to exclude other associated congenital anomalies.
Hay múltiples anormalidades estructurales congénitas que afectan al tracto urogenital masculino y que pueden afectar a los genitales externos masculinos, a los genitales internos o a ambos. Las anomalías congénitas de los conductos deferentes pueden ser unilaterales o bilaterales, que pueden ser completas o segmentarias e incluyen: agenesia, atresia, duplicación, ectopia o divertículo. Las anomalías de los conductos deferentes pueden ser aisladas o estar asociadas con otras anomalías congénitas, especialmente en el tracto urogenital masculino. Estas raras anomalías de los conductos deferentes pueden descubrirse durante el examen genital (ya sea clínica o radiológicamente) o incluso accidentalmente durante cirugías inguinales, como en la varicocelectomía, la reparación de hernias, la vasectomía o la orquiopexia. Por la presente comunicamos el primer caso de triple conducto deferente en un varón de 35 años que fue sometido a palpación en el examen del cordón espermático y se confirmó mediante ecografía transrectal. Por lo tanto, debe hacerse una evaluación adecuada de los casos de conductos deferentes múltiples para evitar la lesión accidental durante la operación y excluir otras anomalías congénitas asociadas.
Testosterone stimulates the embryologic development of the vas deferens from the Wolffian (Mesonephric) duct. It is a thick fibromuscular tube about 45cm in length and 3–5mm in diameter that is lined by pseudostratified columnar epithelium with stereo-cilia that convoys spermatozoa from the epididymis to the ejaculatory ducts during ejaculation. There are three main parts; intrascrotal, inguinal and intrapelvic where it passes retroperitoneal in the pelvis and finally it joins the duct of the seminal vesicle to make the ejaculatory duct.1 Reportedly, vas deferens anomalies affect less than 0.05% of the general population.2 Duplication of the vas deferens is a very rare congenital anomaly with only a few cases reported worldwide.2–6 It is known that duplication of the vas deferens is associated with genitourinary anomalies such as unilateral renal agenesis.7 The term duplication of the vas deferens refers to the identification of two separate vasa deferentia within the spermatic cord.7 The embryologic etiology of duplicated vas deferens has not yet been clearly established but it is assumed that duplication of the vas deferens is caused by duplication of the fetal mesonephric system or transverse division of mesonephric duct.8 Consistently, the following two theories are the most supported. The first theory suggests that the duplication of the vas deferens may be due to duplication of the fetal mesonephric system.4,7 According to this theory, the vas deferens develops from the central portion of the mesonephric (Wolffian) duct, which is termed the proximal vas precursor. Duplication of the proximal vas precursor presumably gives rise to the duplication of the vas deferens. Another potential theory suggests that transverse division of the mesonephric duct during organogenesis causes the duplication of the vas deferens.9 We assume that triple vas deferens may develop in the same way like duplicate vas deferens.
If duplicated vas deferens is not detected during surgery, iatrogenic injury to the vas deferens and other complications may develop.5 The presence of such anomaly can also lead to inadvertent failure of vasectomy.10 According to most case reports, duplication of the vas deferens is accidentally identified during varicocelectomy, hernia repair, vasectomy or orchiopexy. Therefore, surgeons performing inguinal procedures should be well aware of the duplication and even triplication like ours to reduce vas deferens injury and vasectomy failure. We hereby firstly reported a case of triplication of the vas deferens.
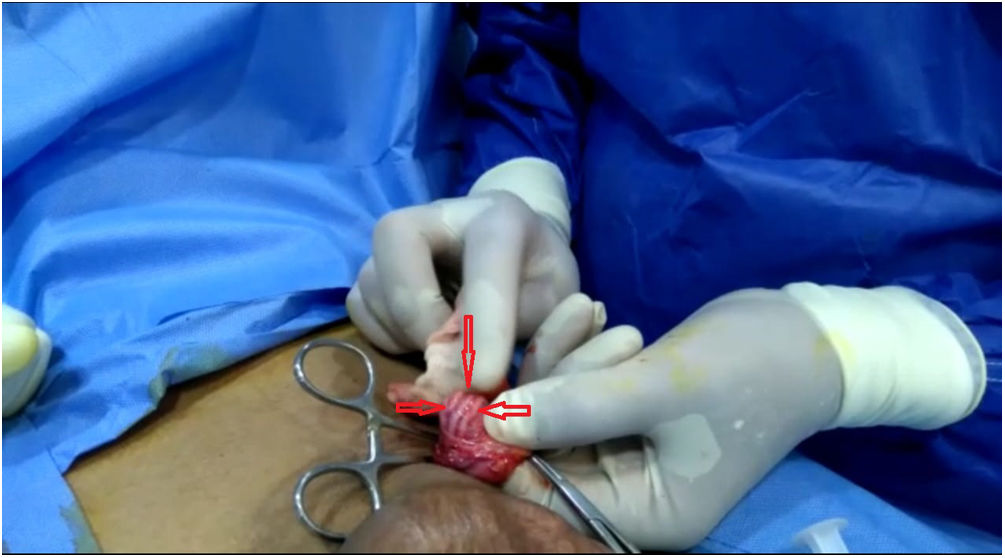
MethodsA 35 year gentleman presented to a specialized in vitro fertilization center complaining of 1ry infertility for 6 years. His past medical history and family history were irrelevant. After proper counseling, the patient was assigned for bilateral varicocelectomy hoping to improve semen parameters and to achieve spontaneous conception. Using a sub-inguinal approach, varicocelectomy was performed under loupe magnification through a small skin incision under general anesthesia. The left spermatic cord was delivered and dissected exposing the contents of the spermatic cord; three white cord-like structures were identified in the spermatic cord (Fig. 1). They were dissected and isolated and triple vas deferens was identified. The dilated internal and external spermatic veins were carefully dissected, ligated by silk 3/0 sutures and divided. Finally, haemostasis was performed and the spermatic cord was placed back in its course and the wound was closed in layers using Vicryl 4/0 by subcuticular technique. Right varicocelectomy was done in the same steps but on exploration we found single vas deferens. Finally, the patient was discharged on the same day without any complications.
Results that were identified in the dissected spermatic cord intraoperative.")
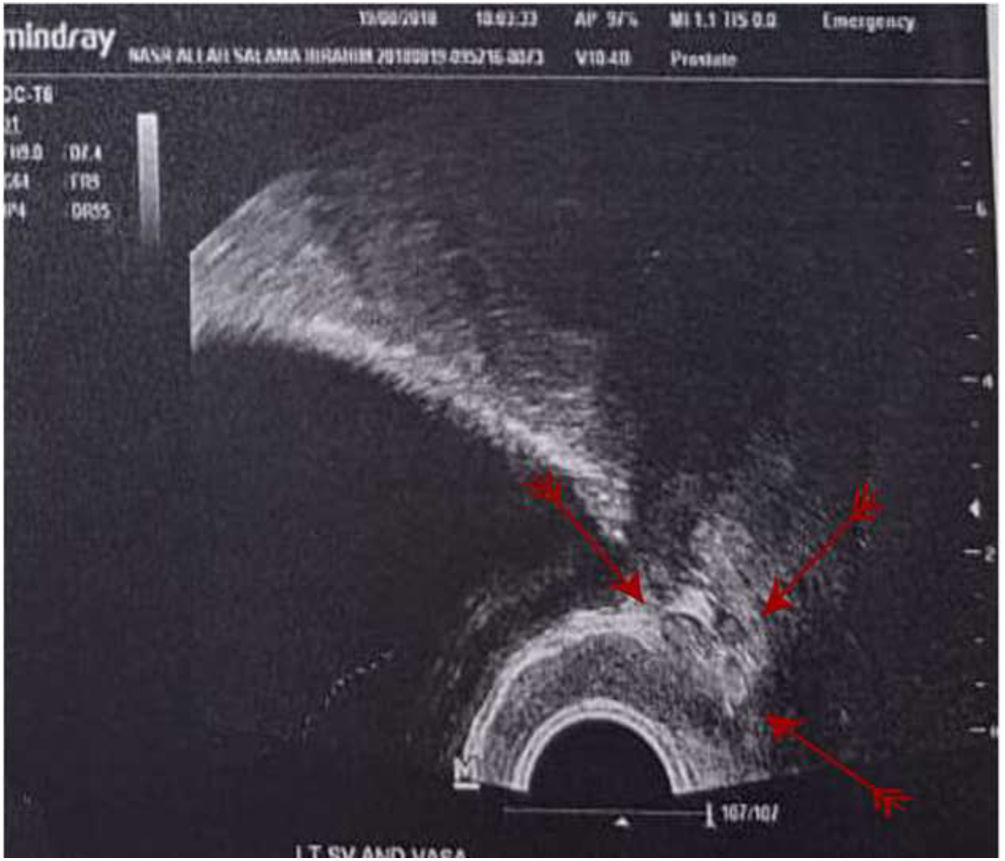
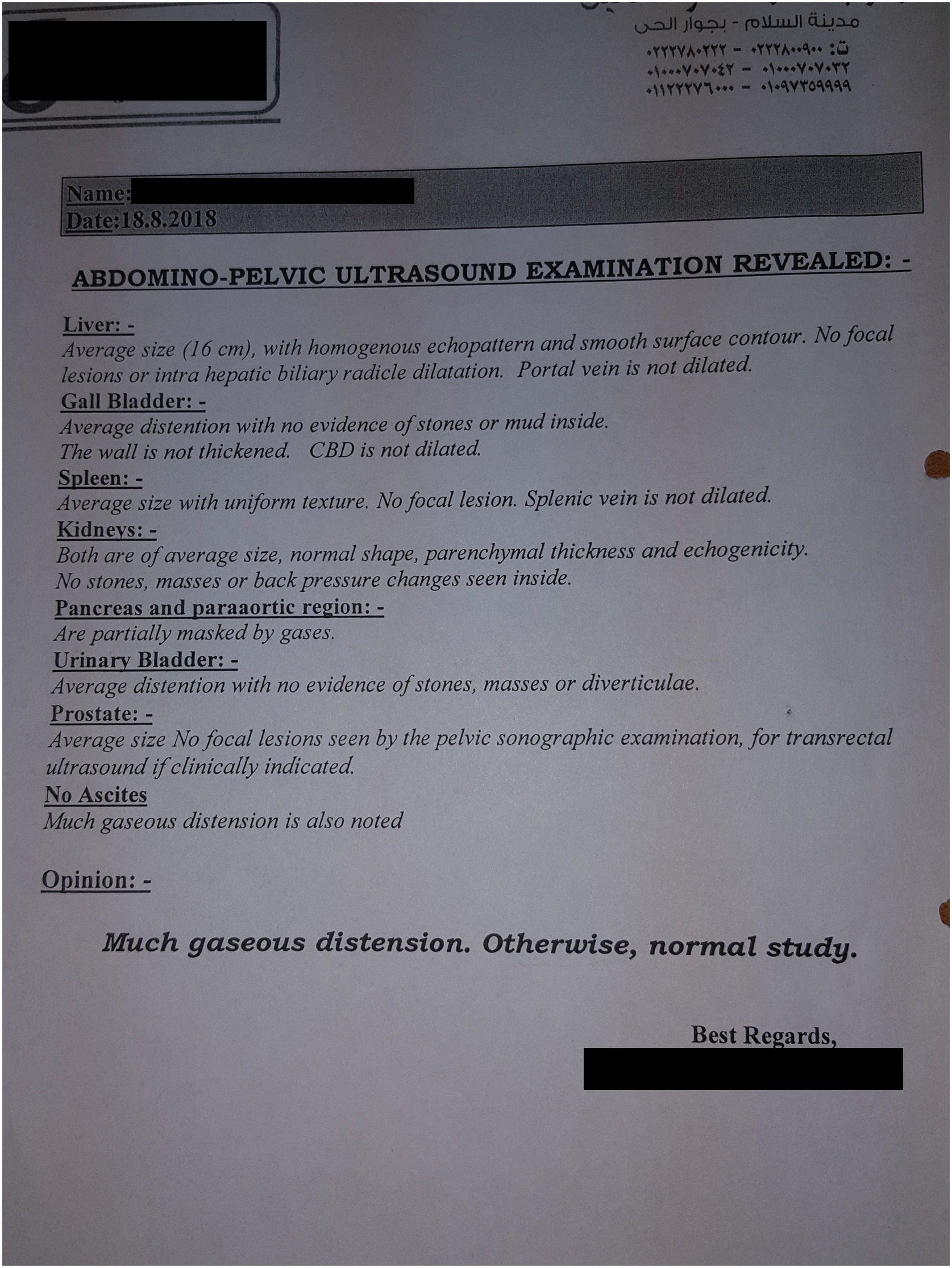
Pre-operative clinical examination revealed normal secondary sex characters, no gynaecomastia, bilateral moderate-sized testes and bilateral varicocele (left grade II, right grade I). His semen analysis showed teratozoospermia (98%), abnormal SDF index (49%) upon which he received medical treatments mainly antioxidants. On palpation of the spermatic cord 3 vasa differentia were felt on the left side while only 1 vas deferens was felt on the right side. Unfortunately, scrotal duplex study did not show the presence of 3 vasa differentia on the left side. Even though, it confirmed the presence of bilateral dilated pampini form plexus of veins with maximum diameters that were 2.7mm and 3.3mm on the right and left sides, respectively, together with bilateral positive continuous regurge noticed markedly on the left side. There are also dilated, regurging gubernucular veins more on the left side. Thus, a preoperative trans-rectal ultrasound (TRUS) was performed to assert the presence of 3 vasa differentia on the left side and to exclude any associated vas deferens anomalies (Fig. 2). During the follow-up visit, the patient was doing well without complain and pelvi-abdominal ultrasonography did not reveal any associated urogenital anomalies (Fig. 3).


Among the anomalies of the vas deferens, duplication of the vas deferens is a rare congenital malformation with only a few cases reported in the world literature. Since Coetzee (1959) who firstly reported a double vas deferens, there have been 28 reports describing a total of 29 cases of duplicated vasa deferentia.11
Recently, an Egyptian case report demonstrated the presence of duplicated vas deferens that was also on the left side.12 Identification of the vas deferens is necessary during operations such as varicocelectomy orchiopexy, herniorrhaphy, or vasectomy because injury to the vas deferens is a recognized surgical complication of these operations.4,8,13,14 Noteworthy, Injury to the vas deferens during surgery may cause infertility, chronic pain, and spermatic granulomas.15 While the terms duplicate and double vas deferens have been used interchangeably, duplication of the vas deferens refers to the identification of two separated vas deferens within the spermatic cord, and it should be distinguished from the term double vas, which describes an ectopic ureter draining into the ejaculatory system and is often associated with ipsilateral renal dysgenesis.4,7 Liang et al. (2012) has suggested 3 classification systems for poly-vasa deferentia.3 Type I is the classical duplicated vas deferens (partial or complete) where a second vas deferens is identified in the spermatic cord with no polyorchidism.3 Type II is multiple vas deferens associated with polyorchidism.3 Type III is false poly-vasa deferential and represents the double vas deferens, where an ectopic ureter drains into the ejaculatory system.3 Intraoperative exploration and postoperative pelvi-abdominal US confirmed that there was no extra testis and abnormal ureter draining system in our case. Thus, our case cannot be one of these 3 types and should be considered as type IV multiple vas deferens where 3 vasa deferentia were detected without polyorchidism. Duplication of the vas deferens has been identified within a wide range of ages from 7 months to 75 years.9,16 As regards laterality, it has been reported that right-sided, left-sided and bilateral duplication occurred equally; unilateral duplication is twice as common as bilateral duplication.3 Interestingly, there is no more information about triplication of the vas deferens to assess its relation to genitor-urinary anomalies.
Further discussion on possible genitourinary abnormalities that may accompany triplication vas deferens is required as well as consensus on intraoperative exploration and post-operative imaging should be established. Diagnosis of triplication of the vas deferens is the identification of a third vas deferens. As triplicated vasa deferentia may be found incidentally, intra-operative doppler can be helpful in the differentiation of the vas deferens from other structures such as the spermatic arteries and veins.3 In conclusion, triplication of the vas deferens was not reported before. Failure to recognize this variation can lead to injury of the vas deferens during inguinal surgery and can result in unexpected outcomes after vasectomy. TRUS is an important tool to confirm the presence of 3 vasa differentia. Postoperative imaging such as abdominal US or CT scans should be performed to determine the presence of any other genitourinary anomalies.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Author's contributionsMohammed Yousry: did the operation and TRUS for the patient.
Sameh Fayek: intellectually drafted the manuscript and revised its data critically.
Conflict of interestThe authors report no conflict of interest.