


We aimed to study the risk factors of erectile dysfunction (ED) and different patterns of phosphodiestrase type 5 inhibitors (PDE5is) usage among Egyptian patients.
Patients and methodsOne thousand five hundred consecutive Egyptian patients complaining of ED were included in this cross-sectional study from July (2014) to October (2015). Patients were requested to answer the international index of erectile function questionnaire (IIEF-5). Statistical differences between groups were tested using Chi square test and Spearman's rho correlation coefficient for qualitative variables.
ResultsRemarkably, significant associations between IIEF scores and aging and diabetes mellitus (DM) and hypertension (HTN) and ischaemic heart disease (IHD) and hyperlipidaemia were shown in the studied patients (p<.0001, p<.0001, p<.0001, p<.0001, p<.0001, respectively). Eventually, our study showed significant correlations between different age groups and morning erection and lower urinary tract symptoms and HTN and IHD and DM where the severity of ED was directly proportional to the absence or decreased strength of morning erection with aging and the increased incidence of LUTS and HTN and IHD and DM with aging (p<.0001; p=.001; p<.0001; p<.0001; p<.0001, respectively).
ConclusionOur study demonstrated that aging; DM, HTN and hyperlipidaemia are potential major risk factors of ED in Egypt for further validation. In addition, most of the participants used PDE5is without prior medical consultation together with concomitant administration of illicit drugs.
El objetivo fue estudiar los factores de riesgo de la disfunción eréctil (DE) y los diferentes patrones de uso de los inhibidores de la fosfodiesterasa tipo 5 (PDE5is) entre los pacientes egipcios.
Pacientes y métodosMil quinientos pacientes egipcios consecutivos que se quejaban de DE fueron incluidos en este estudio transversal desde julio de 2014 hasta octubre de 2015. Se pidió a los pacientes que respondieran al cuestionario del índice internacional de la función eréctil (IIEF-5). Las diferencias estadísticas entre los grupos se probaron mediante la prueba de Chi-cuadrado y el coeficiente de correlación rho de Spearman para las variables cualitativas.
ResultadosNotablemente, se mostraron asociaciones significativas entre las puntuaciones del IIEF, el envejecimiento, la diabetes mellitus (DM), la hipertensión (HT), la cardiopatía isquémica (IHD, por sus siglas en inglés) y la hiperlipidemia en los pacientes estudiados (p<0,0001; p<0,0001; p<0,0001; p<0,0001, p<0,0001, respectivamente). Eventualmente, nuestro estudio había mostrado correlaciones significativas entre los diferentes grupos de edad, la erección matutina, los síntomas del tracto urinario inferior, la HT, la IHD y la DM donde la severidad de la DE era directamente proporcional a la ausencia o la disminución de la fuerza de la erección matutina con el envejecimiento y el aumento de la incidencia de LUTS, HT, IHD y DM con el envejecimiento (p<0,0001; p=0,001; p<0,0001; p<0,0001; p<0,0001, respectivamente).
ConclusiónEn resumen, nuestro estudio demostró que el envejecimiento; la DM, la HT y la hiperlipidemia son los principales factores de riesgo potenciales de la DE en Egipto para una mayor validación. Además, la mayoría de los participantes usaron PDE5is sin consulta médica previa junto con la administración concomitante de drogas ilícitas.
Epidemiology may be defined as the scientific evaluation of distribution and determinants of disease in humans where these data are the cornerstone for determining the overall magnitude of a problem in a given community. Health care providers benefit from these data to identify the magnitude of the studied problem in the community and set up screening, diagnostic, and treatment plans.1 ED is highly prevalent all over the world and is estimated to increase exponentially over the next 10–15 years. Every culture may differ significantly from it's counterpart as regards orientations about male sexual function and effects of ED on quality of life.2–4 Several epidemiological studies have shown a strong association between ED prevalence and age and chronic medical conditions including cardiovascular risk status, diabetes mellitus (DM), depression, lower urinary tract symptoms.5–8 However, there is a difficulty to compare between different surveys due to tremendous variations in methodologies and interpretation of results, thus the conclusions stemmed from American and European studies may be inaccurate in reflecting the magnitude of ED in the developing world.2 This is comprehensible as these conclusions were based on studies conducted mainly in a dominantly white male population with a different life style and developed socioeconomic standard of living. Furthermore, about 30% of ED men seek professional help ending in 11% only who actually receive treatment.9,10 Our current research studied the epidemiological factors of ED and demonstrated different patterns of phosphodiestrase type 5 inhibitors (PDE5is) usage among a representative sample of the Egyptian society.
Patients and methodsStudy design and settingsOne thousand five hundred consecutive Egyptian patients complaining of ED were included in this cross sectional study from our outpatient clinics from July (2015) to October (2016). All the enrolled participants signed informed consents. Approval of our local ethical committee was obtained that is compliant to Helsinki declaration (1964).
Inclusion criteriaAny patient complained of ED for at least three months and involved in a stable relationship was recruited in this study.
Exclusion criteriaAll subjects with unstable relationship were excluded from this study. Also, patients receiving intracorporeal injection or underwent penile implant or patients who suffer from premature ejaculation were excluded from this study as this may affect the outcome of the international index of erectile function questionnaire.11
All the participants were subjected to the following:
Patients were asked about age, residence and level of education. Special habits of known or probable negative effect on erectile function such as tobacco smoking, alcohol or recreational drugs abuse were asked about. Moreover, the patients were asked mainly about systemic illnesses that are mostly relevant or can affect erectile function such as type and duration of diabetes mellitus (DM) and hypertension (HTN), chronic hepatitis (HCV) (past history or active disease), ischemic heart disease (IHD) (past history) with special care to the usage of PDE5is. Also, we asked for lipid profile to determine hyperlipidemia as well as symptoms of micturation difficulties to determine lower urinary tract symptoms (LUTS).
Finally, patients were requested to answer the international index of erectile function questionnaire (IIEF-5).11 Severity of ED was determined according to IIEF-5 scores as follow: mild erectile dysfunction (17–21), moderate erectile dysfunction (8–11), mild to moderate erectile dysfunction (12–16), severe erectile dysfunction (5–7).
Statistical methodThe data was analyzed using the statistical package SPSS version 15 and summarized using descriptive statistics: mean, standard deviation, minimal and maximal values for quantitative variables and number and percentage for qualitative values. Statistical differences between groups were tested using Chi square test and Spearman's rho correlation coefficient for qualitative variables. P-values less than or equal to 0.05 was considered statistically significant
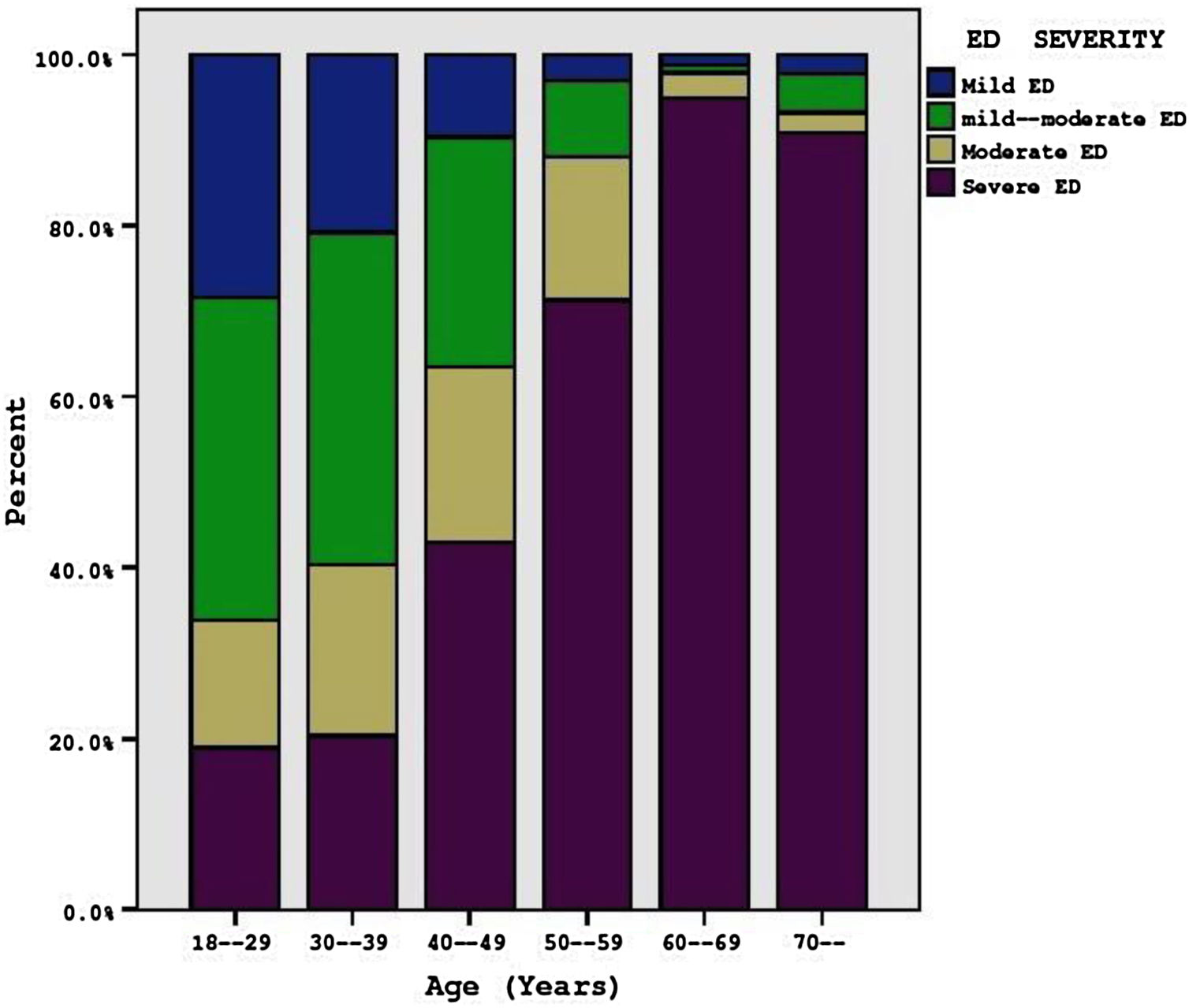
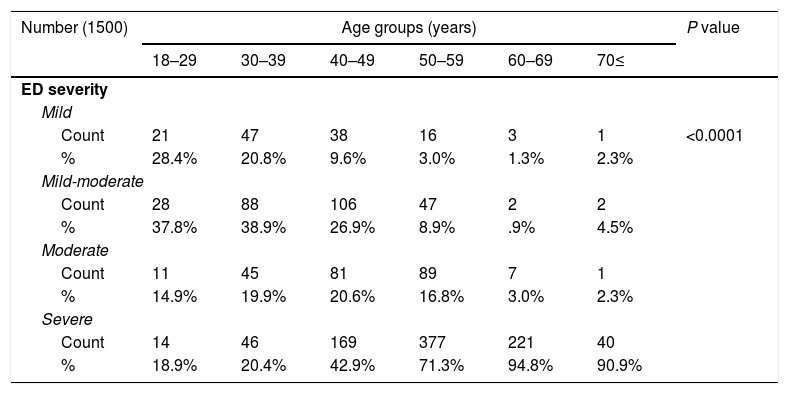
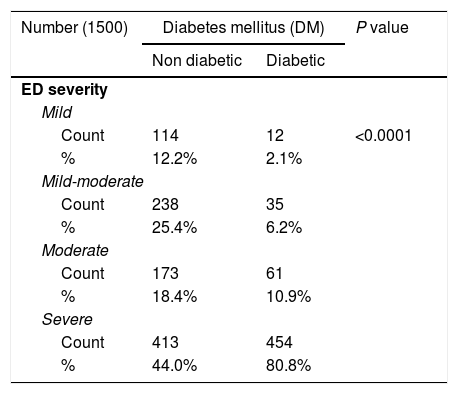
ResultsOur study had shown that the mean age of the patients was 49.48 years±11.27. Furthermore, the mean duration of DM was 8.75 years±6.72. Besides, the mean duration of HTN of the patients was 7.20 years±5.79. Remarkably, the degree of ED was categorized as mild (n=126), moderate (n=273) and severe (n=867) according to the IIEF erectile function domain scores and showed significant association with aging (p<0.0001) (Table 1, Fig. 1). Also, 722 patients (48.1%) were non smokers, while 668 patients were current smokers, and 110 patients were ex-smokers (7.3%). No significant association was noticed between IIEF score and smoking (p 0.096) (Table 1). 108 patients (7.2%) did not abuse substances other than nicotine (tobacco), while the majority of the patients (1392, 92.8%) abused illicit substances (Table 1). Our study had revealed a statistical inverse relationship between IIEF scores and substance abuse (p<0.0001) (Table 1). There were 938 patients (62.5%) who didn’t have DM, while 562 patients (37.5%) had DM (Table 2).
Shows association between severity of erectile dysfunction (ED) and different age groups and smoking and addiction among the participants.
| Number (1500) | Age groups (years) | P value | |||||
|---|---|---|---|---|---|---|---|
| 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70≤ | ||
| ED severity | |||||||
| Mild | |||||||
| Count | 21 | 47 | 38 | 16 | 3 | 1 | <0.0001 |
| % | 28.4% | 20.8% | 9.6% | 3.0% | 1.3% | 2.3% | |
| Mild-moderate | |||||||
| Count | 28 | 88 | 106 | 47 | 2 | 2 | |
| % | 37.8% | 38.9% | 26.9% | 8.9% | .9% | 4.5% | |
| Moderate | |||||||
| Count | 11 | 45 | 81 | 89 | 7 | 1 | |
| % | 14.9% | 19.9% | 20.6% | 16.8% | 3.0% | 2.3% | |
| Severe | |||||||
| Count | 14 | 46 | 169 | 377 | 221 | 40 | |
| % | 18.9% | 20.4% | 42.9% | 71.3% | 94.8% | 90.9% | |
| Number (1500) | Smoking | ||||||
|---|---|---|---|---|---|---|---|
| Ex smoker | Non smoker | Smoker | |||||
| ED severity | |||||||
| Mild | |||||||
| Count | 7 | 54 | 65 | 0.96 | |||
| % | 6.4% | 7.5% | 9.7% | ||||
| Mild-moderate | |||||||
| Count | 12 | 137 | 124 | ||||
| % | 10.9% | 19.0% | 18.6% | ||||
| Moderate | |||||||
| Count | 14 | 110 | 110 | ||||
| % | 12.7% | 15.2% | 16.5% | ||||
| Severe | |||||||
| Count | 77 | 421 | 369 | ||||
| % | 70.0% | 58.3% | 55.2% | ||||
| Number (1500) | Addiction | P-value | |
|---|---|---|---|
| Positive | Negative | ||
| ED severity | |||
| Mild | |||
| Count | 106 | 20 | <0.0001 |
| % | 7.6% | 18.5% | |
| Mild-moderate | |||
| Count | 234 | 39 | |
| % | 16.8% | 36.1% | |
| Moderate | |||
| Count | 215 | 19 | |
| % | 15.4% | 17.6% | |
| Severe | |||
| Count | 837 | 30 | |
| % | 60.1% | 27.8% | |

shows association between severity of ED and DM and HTN and hyperlipidemia and IHD.
| Number (1500) | Diabetes mellitus (DM) | P value | |
|---|---|---|---|
| Non diabetic | Diabetic | ||
| ED severity | |||
| Mild | |||
| Count | 114 | 12 | <0.0001 |
| % | 12.2% | 2.1% | |
| Mild-moderate | |||
| Count | 238 | 35 | |
| % | 25.4% | 6.2% | |
| Moderate | |||
| Count | 173 | 61 | |
| % | 18.4% | 10.9% | |
| Severe | |||
| Count | 413 | 454 | |
| % | 44.0% | 80.8% | |
| Number (1500) | Hypertension (HTN) | ||
|---|---|---|---|
| Negative | Positive | ||
| ED severity | |||
| Mild | |||
| Count | 117 | 9 | <0.0001 |
| % | 10.0% | 2.7% | |
| Mild-moderate | |||
| Count | 235 | 38 | |
| % | 20.1% | 11.5% | |
| Moderate | |||
| Count | 206 | 28 | |
| % | 17.6% | 8.5% | |
| Severe | |||
| Count | 612 | 255 | |
| % | 52.3% | 77.3% | |
| Number (1500) | Hyperlipidemia | ||
|---|---|---|---|
| Negative | Positive | ||
| ED severity | |||
| Mild | |||
| Count | 122 | 4 | <0.0001 |
| % | 9.3% | 2.1% | |
| Mild-moderate | |||
| Count | 254 | 19 | |
| % | 19.4% | 10.1% | |
| Moderate | |||
| Count | 205 | 29 | |
| % | 15.6% | 15.4% | |
| Severe | |||
| Count | 731 | 136 | |
| % | 55.7% | 72.3% | |
| Number (1500) | Ischemic heart disease (IHD) | ||
|---|---|---|---|
| Negative | Positive | ||
| ED severity | |||
| Mild | |||
| Count | 123 | 3 | <0.0001 |
| % | 9.0% | 2.3% | |
| Mild-moderate | |||
| Count | 261 | 12 | |
| % | 19.1% | 9.0% | |
| Moderate | |||
| Count | 221 | 13 | |
| % | 16.2% | 9.8% | |
| Severe | |||
| Count | 762 | 105 | |
| % | 55.7% | 78.9% | |
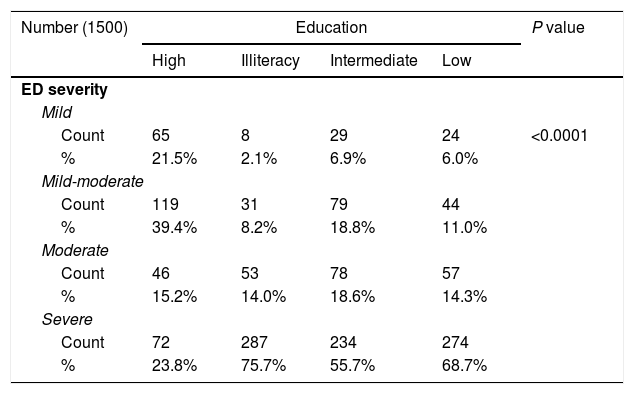
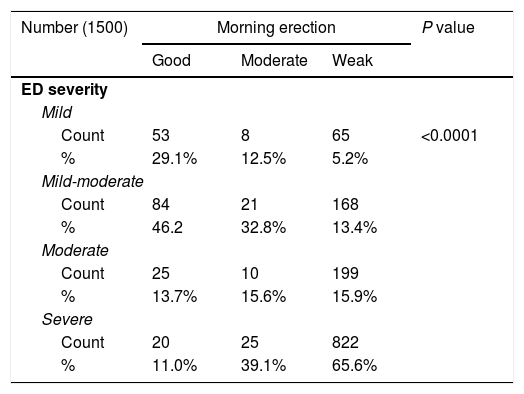
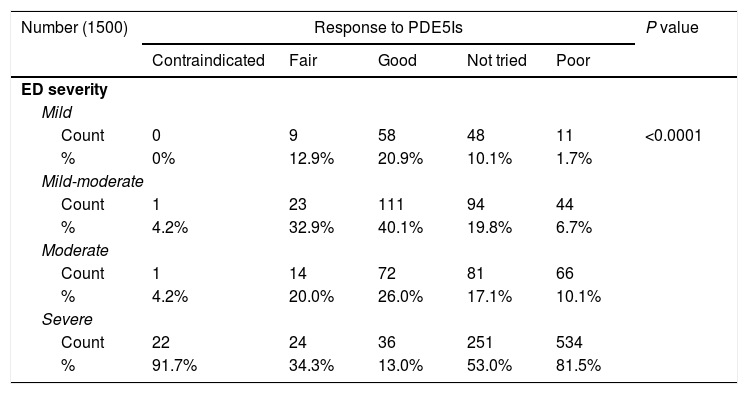
A significant association between IIEF scores and DM was shown in the studied patients (p<0.0001) (Table 2). There were 1170 patients (78%) who didn’t have HTN, while 330 patients (22%) had HTN. A significant association between IIEF scores and HTN in the studied patients was also observed (p<0.0001) (Table 2). Additionally, 133 patients (8.9%) suffered from IHD, while 1367 patients (91.1%) did not suffer from IHD. Our study had demonstrated a significant association between IIEF scores and IHD (p<0.0001) (Table 2). Association between hyperlipidemia and IIEF scores was shown to be statistically significant (p<0001) (Table 2). Remarkably, only 20.1% of the included patients received high education, 28% received intermediate education, while 51% were illiterate or received low level of education (Table 3). Interestingly, our study had shown significant negative association between higher level of education and percentage of complete ED (p<0.0001) (Table 3). Moreover, the majority (63%) of the patients were coming from rural and semirural areas including slums and countryside while 37% of the patients were coming from urban areas. Significant positive association was noticed between residence in rural areas and percentage of complete ED (p<0.0001) (Table 3). Further, 353 patients (23.5%) suffered from LUTS and 1147 patients (76.4%) didn’t complain of LUTS (Table 3). No significant correlation was observed between IIEF scores and LUTS (p=0.226) (Table 3). 1254 patients (83.6%) had weak morning erection (Table 4). The difference in the level of morning erection among the participants as regards to the severity of ED was of high statistical significance (p<0.001) (Table 4). Moreover, significant association was noticed between good morning erection and wife cooperation as incidence of good morning erection exponentially increased with higher wife cooperation (p=0.012) (Table 4). The majority of the patients (534 out of 655, 81.5%) who showed poor response to PDE5Is were suffering from severe ED (Table 5). The difference in the response to PDE5Is among the participants was of high statistical significance (p<0.0001) (Table 5). 55 patients (3.7%) were known to be HCV positive, while 1445 patients (96.3%) were not known to have HCV (p 0.335) (Table 5).
shows association between severity of ED and level of education and residence and lower urinary tract symptoms (LUTS).
| Number (1500) | Education | P value | |||
|---|---|---|---|---|---|
| High | Illiteracy | Intermediate | Low | ||
| ED severity | |||||
| Mild | |||||
| Count | 65 | 8 | 29 | 24 | <0.0001 |
| % | 21.5% | 2.1% | 6.9% | 6.0% | |
| Mild-moderate | |||||
| Count | 119 | 31 | 79 | 44 | |
| % | 39.4% | 8.2% | 18.8% | 11.0% | |
| Moderate | |||||
| Count | 46 | 53 | 78 | 57 | |
| % | 15.2% | 14.0% | 18.6% | 14.3% | |
| Severe | |||||
| Count | 72 | 287 | 234 | 274 | |
| % | 23.8% | 75.7% | 55.7% | 68.7% | |
| Number (1500) | Residence | ||
|---|---|---|---|
| Rural | Urban | ||
| ED severity | |||
| Mild | |||
| Count | 34 | 92 | <0.001 |
| % | 3.5% | 17.2% | |
| Mild-moderate | |||
| Count | 109 | 164 | |
| % | 11.3% | 30.6% | |
| Moderate | |||
| Count | 148 | 86 | |
| % | 15.4% | 16.0% | |
| Severe | |||
| Count | 673 | 194 | |
| % | 69.8% | 36.2% | |
| Number (1500) | LUTS | P-value | |
|---|---|---|---|
| Negative | Positive | ||
| ED severity | |||
| Mild | |||
| Count | 89 | 37 | 0.226 |
| % | 7.8% | 10.5% | |
| Mild-moderate | |||
| Count | 202 | 71 | |
| % | 17.6% | 20.1% | |
| Moderate | |||
| Count | 183 | 51 | |
| % | 16.0% | 14.4% | |
| Severe | |||
| Count | 673 | 194 | |
| % | 58.7% | 55.0% | |
shows association between severity of ED and morning erection and association between wife cooperation and morning erection.
| Number (1500) | Morning erection | P value | ||
|---|---|---|---|---|
| Good | Moderate | Weak | ||
| ED severity | ||||
| Mild | ||||
| Count | 53 | 8 | 65 | <0.0001 |
| % | 29.1% | 12.5% | 5.2% | |
| Mild-moderate | ||||
| Count | 84 | 21 | 168 | |
| % | 46.2 | 32.8% | 13.4% | |
| Moderate | ||||
| Count | 25 | 10 | 199 | |
| % | 13.7% | 15.6% | 15.9% | |
| Severe | ||||
| Count | 20 | 25 | 822 | |
| % | 11.0% | 39.1% | 65.6% | |
| Number (1500) | Morning erection | P-value | ||
|---|---|---|---|---|
| Good | Moderate | Weak | ||
| Wife cooperation | ||||
| Cooperative | ||||
| Count | 138 | 52 | 1060 | 0.012 |
| % | 75.8% | 81.3% | 84.5% | |
| Non cooperative | ||||
| Count | 44 | 12 | 194 | |
| % | 24.2% | 18.7% | 15.5% | |
shows association between severity of ED and response to phosphodiestrase type 5 inhibitors (PDE5Is) and hepatitis C virus (HCV).
| Number (1500) | Response to PDE5Is | P value | ||||
|---|---|---|---|---|---|---|
| Contraindicated | Fair | Good | Not tried | Poor | ||
| ED severity | ||||||
| Mild | ||||||
| Count | 0 | 9 | 58 | 48 | 11 | <0.0001 |
| % | 0% | 12.9% | 20.9% | 10.1% | 1.7% | |
| Mild-moderate | ||||||
| Count | 1 | 23 | 111 | 94 | 44 | |
| % | 4.2% | 32.9% | 40.1% | 19.8% | 6.7% | |
| Moderate | ||||||
| Count | 1 | 14 | 72 | 81 | 66 | |
| % | 4.2% | 20.0% | 26.0% | 17.1% | 10.1% | |
| Severe | ||||||
| Count | 22 | 24 | 36 | 251 | 534 | |
| % | 91.7% | 34.3% | 13.0% | 53.0% | 81.5% | |
| Number (1500) | HCV | P-value | |
|---|---|---|---|
| Negative | Positive | ||
| ED severity | |||
| Mild | |||
| Count | 120 | 6 | 0.335 |
| % | 8.3% | 10.9% | |
| Mild-moderate | |||
| Count | 268 | 5 | |
| % | 18.5% | 9.1% | |
| Moderate | |||
| Count | 225 | 9 | |
| % | 15.6% | 16.4% | |
| Severe | |||
| Count | 832 | 35 | |
| % | 57.6% | 63.6% | |
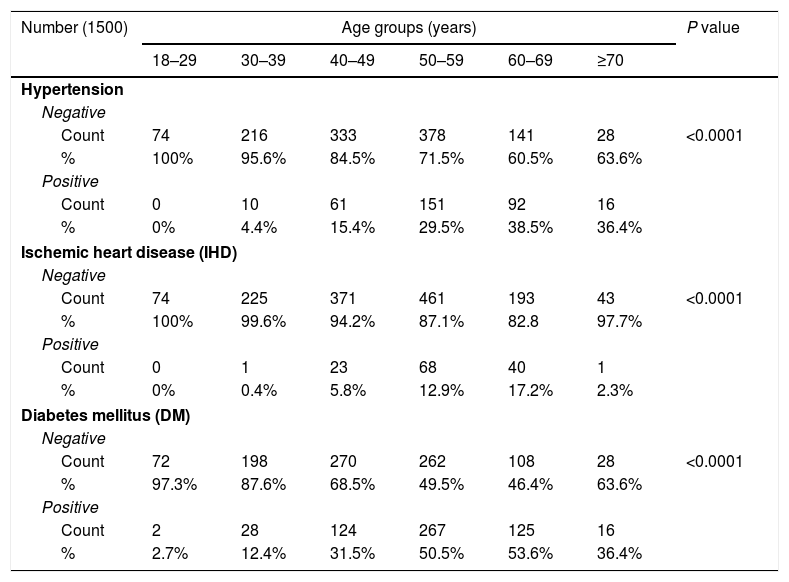
Eventually, our study had shown correlations between different age groups and morning erection and lower urinary tract symptoms and HTN and IHD and DM (Table 6), where the severity of ED was directly proportional to the absence or decreased strength of morning erection with aging and the increased incidence of LUTS and HTN and IHD and DM with aging (p<0.0001; p=0.001; p<0.0001; p<0.0001; p<0.0001, respectively) (Table 6).
shows the correlation between different age groups and hypertension and IHD and DM.
| Number (1500) | Age groups (years) | P value | |||||
|---|---|---|---|---|---|---|---|
| 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | ≥70 | ||
| Hypertension | |||||||
| Negative | |||||||
| Count | 74 | 216 | 333 | 378 | 141 | 28 | <0.0001 |
| % | 100% | 95.6% | 84.5% | 71.5% | 60.5% | 63.6% | |
| Positive | |||||||
| Count | 0 | 10 | 61 | 151 | 92 | 16 | |
| % | 0% | 4.4% | 15.4% | 29.5% | 38.5% | 36.4% | |
| Ischemic heart disease (IHD) | |||||||
| Negative | |||||||
| Count | 74 | 225 | 371 | 461 | 193 | 43 | <0.0001 |
| % | 100% | 99.6% | 94.2% | 87.1% | 82.8 | 97.7% | |
| Positive | |||||||
| Count | 0 | 1 | 23 | 68 | 40 | 1 | |
| % | 0% | 0.4% | 5.8% | 12.9% | 17.2% | 2.3% | |
| Diabetes mellitus (DM) | |||||||
| Negative | |||||||
| Count | 72 | 198 | 270 | 262 | 108 | 28 | <0.0001 |
| % | 97.3% | 87.6% | 68.5% | 49.5% | 46.4% | 63.6% | |
| Positive | |||||||
| Count | 2 | 28 | 124 | 267 | 125 | 16 | |
| % | 2.7% | 12.4% | 31.5% | 50.5% | 53.6% | 36.4% | |
Our study had reported that the mean age of the patients was 49.48 years that was slightly lower than that reported by the Massachusetts male aging study (MMAS) where the mean age in this study was 54 years which may be attributed to the fact that the studies were carried on in different periods, different ethnic background, and increased life expectancy in the United States of America (USA) and western world.5,12 Our study had demonstrated that the prevalence and severity of ED were strongly correlated to aging which comes in line with Bacon et al (2003) who stated a sharp decline of all aspects of sexual function after the age of 50 years by a decade.13 In addition, Laumann et al (2007) stated that when sociodemographic, health, relationship, psychological, and lifestyle variables were controlled ED risk increased with increasing age.14 The current study had revealed that geographical location seemed to affect prevalence and severity of ED as the majority of the patients were coming from rural and semirural areas this may be attributed to having lower level of education and lower economic level. In addition to cultural beliefs of the traditional maleness roles of self-reliance, emotional control, and power that are popular in rural areas together with lack of information, difficulty and reluctance to access health services leading to a delay in seeking treatment with subsequent deterioration and increased severity of the condition. Similarly, Ansong et al. (2000) who studied rural men living in New York State found that 42% guys suffered from ED, which was three to four folds higher than their counterparts in the MMAS suggesting a higher prevalence of ED in rural areas than urban areas.15
Our study showed a strong inverse association between ED and educational attainment, this finding can be explained by the fact that higher education is an interface for higher socioeconomic standard of living, which is linked to healthy lifestyle factors and rapid access to better health care. Moreover, literate men might also be more likely to seek medical attention at an earlier course of the condition.16,17 Our study did not demonstrate any association between the type of smoking and the severity of ED. Similarly, MMAS revealed that tobacco was not an independent risk factor.5 However, tobacco increased other risk factors as the impact of smoking when being exclusive in a subgroup of men without other risk factors of ED doubled the risk of this condition.5 Furthermore, our study did not reveal any significant difference in the severity of ED between current and ex smokers that could be seen in line with several previous studies.8,18 Our study revealed that only 7.2% of the patients reported substance abuse. In the current study, ED was shown to be of milder degree in more than 50% of patient with substance abuse which may be explained by the fact that most of our patients were young age. Consistently, Berrada et al. (2003) found no significant relation between ED and substance abuse as most abusers were young age.19 In the same line, Chew et al. (2008) reported findings that suggested a modest negative association between alcohol abuse and ED that was confounded by the association of other risk factors such as cardiovascular disease and cigarette smoking.8 In contrast, Allen et al (2018) had concluded that that cigarette smoking, alcohol, and lack of physical activity are important for sexual dysfunction.20 Noteworthy, 66.8% of the patients already had utilized PDE5is without professional medical consultation this is due to the ability to purchase PDE5is without medical consultation in Egypt. Further, our study had shown a higher incidence of PDE5is usage among substance abusers. Recently, a study conducted by Attia et al. (2019) demonstrated similar findings as regards PDE5is without medical prescription in addition to concomitant illicit substances intake with PDE5is.21
Our study showed a higher incidence of diabetic patients which makes DM one of the most important and common causes of ED in our country as Egypt is one of the top 10 countries with the highest prevalence of DM worldwide according to the international federation of diabetes and the low patient compliance to treatment and diabetes control which lead to higher prevalence of ED among diabetic patients in Egypt. Besides that, our study showed significant correlation between the severity of ED and presence and duration of DM which comes in line with results of a recent study carried out by Rosen et al. (2009).22 On the other hand, Shabsigh et al. (2005) who conducted a cross-national survey on men's health issues demonstrated the presence of DM in 25% of patients with severe ED.23 Our study demonstrated that hypertensive patients represented 22% of the whole sample. Similarly, Ahn et al. (2007) who conducted a study in South Korea found that hypertensive patients represented 21% of ED patients.24 On the contrary, Seftel et al. (2004) observed that 41.6% of the ED patients had HTN.25 These findings can be explained by large database (more than 2 million patients) of the aforementioned study and different ethnic background as it was carried out in USA. In addition, our study had demonstrated that the severity of ED was directly proportional to the presence and duration of HTN that was similar to the findings of Doumas et al. (2006).26 Our study had demonstrated that 133 patients (8.9%) were known to have IHD which comes more in line with previous study conducted by Ahn et al. (2007).24 On the other hand, Chew et al. (2008) reported higher incidence of IHD (23.2%) among a sample of patients complaining of ED.8 Recently, a study conducted among New Zealand patients who suffer from ED had shown that ED is a marker of subclinical cardiovascular disease.27 Our study had shown that 12.5% of our patients suffered from elevated cholesterol levels where the risk of complete ED was increased. In the same context, the MMAS and a previous report had demonstrated that elevated total cholesterol and low high-density lipoprotein cholesterol levels increased the risk of both complete and moderate to complete ED.8,28
Although our study had revealed that the incidence of LUTS among our patients was (23.5%), yet there was no significant association between LUTS and ED that may be explained by the difference in severity of LUTS in our study compared to others. Where a study by Marszalek et al (2007) performed on patients with LUTS and chronic pelvic pain showed that the IIEF-5 score was 19.5 for men with mild chronic pelvic pain and LUTS versus 15.1 in subjects with moderate/severe symptoms.29 Our study had revealed that only 4% of our patients had chronic hepatitis. Similarly, Marumo et al. (2001) had demonstrated that the prevalence rate of hepatic disease in their ED patients was 4.7%.30 Although the severity of ED was higher in patients with hepatic disease than patients who didn’t have hepatic disease, yet, the difference was of no statistical significance which may be explained by the relatively small number of patients with hepatic disease in our study. Our study had shown that most of the patients with good morning erection were of the youngest age groups suggesting a larger role of psychogenic ED in younger age groups which coincides with Shamloul et al. (2005) findings.31 Interestingly, a relation between morning erection and wife cooperation as an indicator of interpersonal factor was revealed to be significant in our study where the incidence of wife cooperation increased in patients with good morning erection indicating the negative effect of wife in-cooperation as a cause or triggering factor for psychogenic ED. We recognize that our target population was small in size which can be considered a major limitation. Also, non randomized nature of our participants can be added as another limitation. However, our study is one of the first in Egypt to demonstrate the epidemiology of ED among patients who suffer from this condition in addition to one of the few studies that demonstrated the pattern of PDE5Is administration among Egyptian patients who suffer from ED.
ConclusionIn sum, our study demonstrated that aging; DM, HTN and hyperlipidemia are major risk factors of ED in Egypt that is aggravated by low socioeconomic status and low of level of education. In addition, the majority of the participants used PDE5is without prior medical consultation together with concomitant administration of illicit drugs.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestAll authors report no conflict of interest.