


Blood count parameters of patients referring with penile vasculogenic erectile dysfunction (ED) were examined in this study. It was investigated whether eosinophil count (EC), platelet count (PC) and mean platelet volume (MPV), values among the suspected predictive parameters which may affect vascular functions, have a contribution on ED pathology or not.
Materials and methodsPatients referring erectile dysfunction complaint were evaluated. Depending on the medical story, ED degree was determined by measuring International Index of Erectile Function (IIEF). Values such as hormones, complete blood count and other laboratory markers were examined. Penile doppler ultrasonography (PDU) was performed in patients suspected to have vasculogenic ED. According to PDU result, patients with vascular deficiency were included in the penile vasculogenic ED group and patients with normal results were included in the control group. 49 patients participated in the study from the penile vasculogenic ED group and 30 patients from the control group. Intergroup comparisons were performed using the Mann–Whitney U test and the chi-square (χ2) test was used to assess the relationship between categorical variables within the patient groups.
ResultsLow IIEF score in vasculogenic ED group compared to the control group and high EC, MPV and PC values were detected to be statistically significant (p<0.001, p=0.026, p=0.009, p=0.029, respectively). No statistically significant difference was observed among the two groups when age, white blood cells, red blood cells or hemoglobin values are considered (p=0.332, p=0.235, p=0.127, p=0.696, respectively).
ConclusionHigh MPV value and platelet count showing the platelet functions and high eosinophil count are important factors which may play a role in penile vasculogenic ED etiopathogenesis.
Los parámetros de conteo de sangre de los pacientes referidos con disfunción eréctil (DE) vasculogénica del pene fueron examinados en este estudio. Se investigó si los valores de conteo de eosinófilos (CE), el conteo de plaquetas (CP) y el volumen plaquetario medio (VPM), entre los parámetros predictivos sospechados de afectar las funciones vasculares, contribuyen a la patología de DE o no.
Materiales y métodosSe evaluó a los pacientes referidos con quejas de DE. Dependiendo de su historial médico, el grado de DE fue determinado midiendo el índice internacional de función eréctil (IIFE). Se examinaron los valores de hormonas, el conteo total de sangre y otros valores de laboratorio. Se utilizó la ultrasonografía Doppler peneana (UDP) en pacientes en los que se sospechaba DE vasculogénica. Según el resultado de la UDP, los pacientes con deficiencia vascular fueron incluidos en el grupo de DE vasculogénica del pene y los pacientes con resultados normales fueron incluidos en el grupo de control. En el estudio participaron 49 pacientes en el grupo de DE vasculogénica del pene y 30 pacientes en el grupo de control. Las comparaciones intergrupales fueron realizadas utilizando el test U de Mann-Whitney y el test de la chi cuadrado (χ2) para analizar la relación entre los variable categóricos en los grupos de pacientes.
ResultadosResultados bajos de IIFE en el grupo de DE vasculogénica comparados con el grupo de control y resultados altos de CE, VPM y PC fueron detectados como estadísticamente significativos (p<0,001, p=0,026, p=0,009 y p=0,029, respectivamente). No se observó ninguna diferencia significativa estadísticamente entre los 2 grupos cuando se consideraron los valores de edad, glóbulos blancos, glóbulos rojos y hemoglobina (p=0,332, p=0,235, p=0,127 y p=0,696, respectivamente).
ConclusiónUnos valores altos de VPM, un conteo de plaquetas que muestra las funciones de plaquetas y un conteo alto de eosinófilos son factores importantes que pueden desempeñar un papel en la etiopatogenia de la DE vasculogénica del pene.
Erectile dysfunction (ED) is among common diseases. It was predicted that 322 million people will have ED around the world in 2025.1 In studies made on males between forty and seventy years of age, the prevalence was found 69.2% in Turkey and 52% in United States of America.2,3 Erectile dysfunction is difficulty in obtaining and maintaining adequate erection for a satisfactory sexual performance and the stability of this condition.4 Penile erection occurs due to psychological, neural, vascular and endocrine factors and a healthy interaction among them. Erectile dysfunction occurs due to problems in all these factors. ED has a prevalence increasing with age. Since penis has a special vascular network, vascular causes play an important role in ED etiology. These causes are divided into three categories as arteriogenic ED, venogenic ED and mixed vasculogenic ED.4
A metaanalysis made presented strong proofs demonstrating that ED is related to the increase in death risk caused by increased cardiovascular disease (CVD), coronary artery disease, stroke and all reasons.6 Evidences showing that ED is an early finding for coronary artery and peripheric vascular disease gradually increase.4
Platelets play an important role in the atherosclerosis formation phase. Mean platelet volume (MPV) is a significant demonstrator of platelet activity and platelet function reflecting platelet production speed and platelet stimulation. MPV is a potential indicator for thrombocyte reactivity. Large thrombocytes have a more active and more prothrombotic potential in metabolic and enzymatic aspects. Increased MPV is related with indicators demonstrating thrombocyte activity such as increased thrombocyte gathering, tromboxan synthesis and increased expression of adhesion molecules. There are studies showing that increased MPV triggers and increases atherosclerotic processes such as acute coronary syndrome, myocardium infarction and thrombosis. It is known to be connected with atherosclerosis process in penile arterial deficiency.7–10
In many studies, it was claimed that there is a relation between eosinophilia and vascular dysfunction. It is known that eosinophils play an important role in endothelial dysfunction, vasoconstriction, inflammation and thrombosis. Eosinophils stimulate thrombocyte activation and aggregation. Eosinophils also make the thrombosis formation easier by preventing thrombomodulin.9–11
Due to these reasons, the relation between vasculogenic ED and eosinophil count (EC), platelet count (PC) and MPV has become popular in recent studies. However there is a low number of studies on the subject in literature.5,9,10,12
Blood count parameters of patients referring with penile vasculogenic erectile dysfunction (ED) were examined in this study. It was investigated whether eosinophil count (EC), platelet count (PC) and mean platelet volume (MPV) values among the suspected predictive parameters which may effect vascular functions have a contribution on ED pathology or not.
Materials and methods79 patients who referred to the hospital with erectile dysfunction complaint between October 2014 and January 2016, had PDU and whose results can be reached were included in the study. Medical history was taken in a careful and detailed way so that psychogenic and neurological factors can be eliminated and genital and neurological examinations were made. Depending on the medical story, ED degree was determined by measuring International Erectile Function Index (IIEF score). Hormonal and other laboratory values (FSH, LH, testosterone, prolactin, glycemia, urine analysis, kidney and liver function tests) and complete blood count were examined. Blood samples were drawn from the antecubital vein at 08:00–10:00 a.m. after an overnight fasting period. The blood samples were collected in tubes containing dipotassium ethylenediaminetetraacetic acid. All of the measurements were performed immediately after venipuncture to prevent in vitro platelet activation.
Penile doppler ultrasonography (PDU) was taken in patients suspected to have vasculogenic ED. After the operation, 60mg papaverine Hcl was applied by intracavernosal injection from the 1/3 zone of the penis proximally with 26 gauge 2ml injector. Afterwards, arterial and venous flows of the penis were evaluated in 5th, 10th, 15th and 20th minutes. Measurements were made with Siemens Acuson S2000, 9MHz linear probe. Arterial deficiency (arteriogenic ED) was diagnosed in patients with a peak systolic velocity (PSV) under 30cm/seconds, venous insufficiency (venogenic ED) in patients with end diastolic flow velocity (EDV) above 5cm/seconds and mixed ED. in patients with both. According to PDU result, patients with penile vasculogenic deficiency (arteriogenic+venogenic+mixed) were included in penile vasculogenic ED group and the patients with normal results were included in the control group. 49 patients participated in the study from the penile vasculogenic ED group and 30 patients from the control group.
Exclusion criteriaUsing antiplatelet and anticoagulant drugs, patients with neurogenic or endocrinological ED, a history of pelvic surgery and pelvic trauma, or other vascular risk factors for ED such as diabetes, smoking, or hypertension, recently diagnosed coronary artery disease (CAD) or hematological disorder, active infectious disease, malignancy, immunological disease, or renal or hepatic failure were excluded.
Statistical analysisStatistical analysis was performed with SPSS 15.0 for Windows version 15.0 (SPSS Inc., Chicago, IL, USA). Intergroup comparisons were performed using the Mann–Whitney U test and the chi-square (χ2) test was used to assess the relationship between categorical variables in the patient groups. Area Under the Curve was calculated by ROC regression analyses. Epidemiological diagnosis percentages were calculated by finding cut-off values.
p<0.05 was used as a threshold for statistical significance. Data were presented as means±s.d.
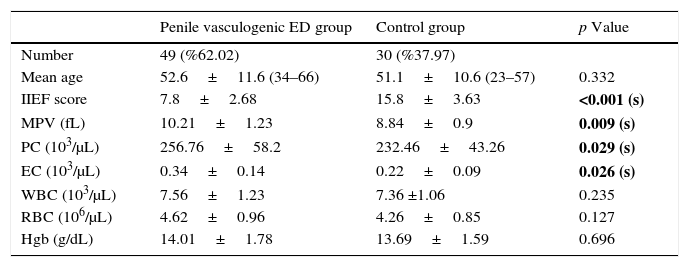
Results79 patients who had penile doppler ultrasonography (PDU) and meeting the criteria were included in the study. Penile vasculogenic deficiency was reported in 49 patients and 30 patients were reported to be normal as the result of PDU. These patients were divided into two as those with penile vasculogenic ED and the control group. In penile vasculogenic ED and control group, mean ages were: 52.6±11.4 (34–66), 51.1±10.6 (23–57) (p=0.332), IIEF scores were: 7.8±2.68, 15.8±3.63 (p<0.001). Other measurements were: MPV (fL); 9.93±1.01, 8.84±0.9 (p=0.009), Platelet Count (PC) (103/μL); 256.76±58.2, 232.46±43.26 (p=0.029), Eosinophil count (EC) (103/μL); 0.34±0.14, 0.22±0.09 (0.026). White blood cells (WBC) were measured as (103/μL); (WBC) (103/μL); 7.56±1.23, 7.36±1.06 (p=0.235), Red blood cells (RBC) (106/μL); 4.62±0.96, 4.26±0.85 (p=0.127), and Hemoglobin (Hgb) level (g/dL) as; 14.01±1.78, 13.69±1.59 (p=0.696). Low IIEF score in vasculogenic ED group compared to the control group and high EC, MPV and PC values were detected to be statistically significant (p<0.001, p=0.026, p=0.009, p=0.029, respectively). No statistically significant difference was observed among the two groups when age, WBC, RBC and Hgb values are considered (p=0.332, p=0.235, p=0.127, p=0.696, respectively). Findings for the patients and Complete Blood Count (CBC) values can be seen in Table 1.
Patient findings and complete blood count (CBC) values.
| Penile vasculogenic ED group | Control group | p Value | |
|---|---|---|---|
| Number | 49 (%62.02) | 30 (%37.97) | |
| Mean age | 52.6±11.6 (34–66) | 51.1±10.6 (23–57) | 0.332 |
| IIEF score | 7.8±2.68 | 15.8±3.63 | <0.001 (s) |
| MPV (fL) | 10.21±1.23 | 8.84±0.9 | 0.009 (s) |
| PC (103/μL) | 256.76±58.2 | 232.46±43.26 | 0.029 (s) |
| EC (103/μL) | 0.34±0.14 | 0.22±0.09 | 0.026 (s) |
| WBC (103/μL) | 7.56±1.23 | 7.36 ±1.06 | 0.235 |
| RBC (106/μL) | 4.62±0.96 | 4.26±0.85 | 0.127 |
| Hgb (g/dL) | 14.01±1.78 | 13.69±1.59 | 0.696 |
Abbreviations: IIEF, International Index of Erectile Function; MPV, mean platelet volume; PC, platelet count; EC, eosinophil count; WBC, white blood cells; RBC, red blood cells; Hgb, hemoglobin; s, significant. Values are presented as mean±s.d.
Statistically significant values are written with bold values.
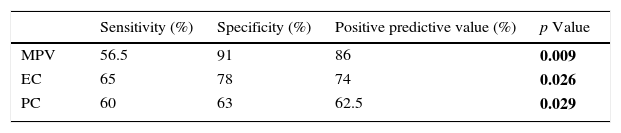
In the evaluation made with Roc regression analysis, statistically significant values for Vasculogenic ED were measured as:
MPV value – sensitivity: 56.5%, specificity: 91%, positive predictive value 86%.
EC – sensitivity: 65%, specificity: 78%, positive predictive value: 74%.
PC – sensitivity: 60%, specificity: 63%, positive predictive value: 62.5%. Findings for sensitivity, specificity and positive predictive values of the parameters statistically significant for vasculogenic ED are available in Table 2.
Table 2.Findings for sensitivity, specificity and positive predictive values of the parameters statistically significant for vasculogenic ED.
Sensitivity (%) Specificity (%) Positive predictive value (%) p Value MPV 56.5 91 86 0.009 EC 65 78 74 0.026 PC 60 63 62.5 0.029 Abbreviations: MPV, mean platelet volume; PC, platelet count; EC, eosinophil count.
Erectile dysfunction (ED) is a disease increasing with age. Its incidence shows a significant increase after 40 years of age especially. It was also detected to be between 1 and 10% even in males under 40 years of age in the studies made.13,14
Organic and psychological factors play a role in erectile dysfunction development. Organic causes play a more dominant role in ED etiology and vascular factors outstand among the organic causes of ED.15 So diseases causing vascular pathologies such as hypertension, hyperlipidemia, diabetes mellitus and coronary artery disease are the main risk factors for vasculogenic ED and this risk increases nearly 1.5–4 times in the presence of these risk factors.16,17 Vasculogenic ED is related to impairment of endothelium-dependent and endothelium-independent relaxations of smooth muscle cells and atherosclerotic occlusion in cavernous arteries. Since atherosclerosis affects all vascular bed, the earliest symptom development is expected in the artery with the narrowest vein lumen. Since the lumen of penile artery is between 1 and 2mm, symptoms based on atherosclerosis in penile artery are observed in early period.4,18,19
Vasculogenic ED plays an important and major role among ED causes. Since MPV and PC are significant demonstrators of platelet function and activation and thromboembolic event incidence increases with platelet activation, the relation between vasculogenic ED and MPV and platelet number is gradually becoming more important.
Eosinophils activate coagulation system and thrombocytes. This situation may cause vasospasm in arteries. It was reported that eosinophil granule proteins may affect cardiovascular system negatively by causing vascular injury and inflammatory cell infiltration. Previous studies demonstrated that eosinophils are related with stent thrombosis, stent restenosis and acute coronary syndromes.9,20 There are studies reporting that eosinophil count is related to vasospastic angina pectoris and large thrombus formation.21 Strong vasoconstrictor and procoagulant effects of eosinophils make us consider the presence of a relation between eosinophil count and vasculogenic ED. Thus eosinophil count was also included as a suspicious predictive factor in the current study.
Çiftci et al. (2013) compared 50 patients with vasculogenic ED with 40 healthy people and stated that MPV values and platelet number are statistically higher in vasculogenic ED group statistically. In this study, vascular endothelial cell damage occurring with thrombocyte activation was held responsible for vasculogenic ED etiopathogenesis.10
In a recent study made in 2015, three groups including vasculogenic ED, ED after radical prostatectomy (nonvasculogenic ED) and control group were compared and it was reported that MPV values and platelet count was statistically higher in vasculogenic ED group.5
Otunctemur et al. (2015) vasculogenic ED patients were compared with healthy control group and in addition to MPV and platelet count, eosinophil count was also included in examination. Although MPV values and platelet count was found statistically higher in vasculogenic ED group, no difference was found in eosinophil count among the two groups which is different from our study.9 The reason may be the fact that most of the patient group with vasculogenic ED in our study are arteriogenic ED patients. Ratio of patients with pure arteriogenic ED in the vasculogenic ED group in our study was 69.3% (34/49). Since thrombosis plays a significant role in arteriogenic ED etiology, high eosinophils may have increased arterial thrombosis potential. This condition may be the reason explaining a different result from the study by Otunctemur et al.
Aldemir et al. (2016) reported that among ED and healthy control group, mean platelet volume (MPV) and platelet distribution width (PDW) values are significantly higher in erectile dysfunction group but the platelet count is not different among the two groups. We think that the patients being general ED and not being specified as vasculogenic ED decrease the reliability of this study.12
In our study, we detected a significant difference between MPV, PC, EC values among the two groups and in penile vasculogenic ED group, MPV, PC and EC values were detected significantly high statistically (p=0.009, p=0.029, p=0.026, respectively).
MPV and PC values were detected high in penile arteriogenic ED group similar to the studies made before.5,9,10 This situation shows that MPV and PC values are a strong predictive factor for both specific penile arteriogenic ED and vasculogenic ED (arteriogenic+venogenic+mixed). However eosinophil count was detected significantly higher in penile arteriogenic ED group which is different from the study by Otunctemur et al.9
This situation suggests that eosinophil count plays a vasculogenic active role. Studies demonstrating that increasing eosinophil count has negative effects on coronary arteries were published.20,21 Based on the negative effect of increasing eosinophil count on arteries and the results of our study, we believe that eosinophil count could be an important factor in etiopathogenesis of penile vasculogenic ED. Since our results are different from the only study.9 We think that this study will make a significant contribution to literature based on its results and compared to the studies made with patients including general ED groups.
Since high MPV, PC and EC values carry vascular dysfunction risk, these patients should be examined carefully for possible asymptomatic cardiovascular system disease. System evaluation should be recommended even though a there is no known cardiovascular disease in this patient group when these values are high and erectile dysfunction is accompanying. Treatment options should be evaluated considering that vascular dysfunction may play a more active role in the etiology in erectile dysfunction accompanied by high MPV, PC and EC values.
ConclusionHigh MPV value and platelet count showing the platelet functions and high eosinophil count are important factor which may play a role in penile vasculogenic ED etiopathogenesis. We do not think that other blood count parameters such as WBC, RBC and Hbg play an active role in penile vasculogenic ED pathogenesis. High MPV, PC, EC values may give a clue about the vasculogenic ED etiology diagnosis without doing diagnostic invasive operations. We think that studies including a patient group including more patients and separate arteriogenic, venogenic, mixed ED patient groups would be more useful on this subject.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interestThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FundingThe authors received no financial support for the research, authorship, and/or publication of this article.
This article is in accordance with ethical standards and has been approved by local authorities.