



The aim of the present study was to assess the relationship between penile length and somatometric parameters, especially cachexia.
Material and methodsWeight and heights of all patients were measured and recorded by an internal medicine specialist. Flaccid and stretched states of penis were measured from pubic bone to tip of glans along the dorsum of the penis using a rigid metric ruler by a single urology specialist. Patients with urogenital abnormalities were excluded from the study. Penile length, age, weight and height values were recorded. Body mass index (BMI) was computed as the ratio of weight to the square of height. Patients were divided into three groups according to BMI cachexia, normal weight and obesity. Groups were defined: Group 1: Cachexia, BMI<18.5; Group 2: normal weight BMI, between 18.5 and 25; Group 3: obesity, BMI>30. Mean and median penile lengths were calculated. These three groups were evaluated in terms of whether there is a difference between flaccid and stretched penile length. Also correlation between weight, height and penile length was determined.
Statistical analyses were performed using the SPSS for windows ver. 16.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at p<0.05.
ResultsOne hundred and twenty four patients enrolled in the study. Fourteen patients were in the cachectic group. Fifty six patients were in the normal weight group. Fifty four patients were in the obese group. Both flaccid and stretched penile lengths were statistically different in these groups (p<0.001; p<0.001). When we compared the groups separately, cachectic group's penile lengths were significantly longer than the normal weight group at both (p<0.01; p=0.02). Cachectic group's penile lengths were significantly longer than the obese group (p<0.001; p<0.001). Also normal weight group's penile lengths were longer than those of the obese group (p<0.001; p<0.001).
ConclusionThe present study is the first one assessing the relationship between cachexia and penile length. As a result, cachexia may be an advantage for penile length.
El objetivo del presente estudio fue evaluar la relación entre la longitud del pene y los parámetros somatométricos, especialmente la caquexia.
Materiales y métodosEl peso y la altura de todos los pacientes fueron medidos y registrados por un especialista en medicina interna. Los estados flácidos y estirados del pene se midieron a partir del hueso púbico hasta la punta del glande a lo largo del dorso del pene, utilizando una regla métrica rígida, por un único especialista en urología. Los pacientes con anormalidades urogenitales fueron excluidos del estudio. Se registraron la longitud del pene, la edad, el peso y las alturas. El índice de masa corporal (IMC) se calcula como el cociente entre el peso y el cuadrado de la altura. Los pacientes fueron divididos en 3 grupos según el IMC: caquexia, peso normal y obesidad. Se definieron los grupos: Grupo 1: caquexia, IMC<18,5; Grupo 2: peso normal, IMC entre 18,5 y 25, y Grupo 3: obesidad, IMC>30. Se calcularon las longitudes del pene media y mediana. Estos 3 grupos fueron evaluados en términos de si había diferencia entre la longitud del pene flácido y estirado. También se determinó la correlación entre el peso, la altura y la longitud del pene.
Los análisis estadísticos se realizaron con el programa SPSS® para Windows ver. 16.0 (SPSS Inc., Chicago, IL, EE.UU.). La significación estadística se estableció en p<0,05.
ResultadosCiento veinticuatro pacientes fueron incluidos en el estudio. Catorce pacientes estaban en el grupo de la caquexia. Cincuenta y seis pacientes estaban en el grupo de peso normal. Cincuenta y cuatro pacientes estaban en el grupo obeso. Ambas longitudes del pene flácido y estiradas fueron estadísticamente diferentes en estos grupos (p<0,001; p<0,001). Cuando se compararon las longitudes del pene por separado, las del grupo caquéctico fueron significativamente mayores que las del grupo de peso normal en ambos (p<0,01; p=0,02). Las longitudes del pene del grupo caquéctico fueron significativamente más largas que las del grupo de obesos (p<0,001; p<0,001). También la longitud del pene del grupo de peso normal era mayor que la del grupo de obesos (p<0,001; p<0,001).
ConclusiónEl presente estudio es el primero en evaluar la relación entre la caquexia y la longitud del pene. Como resultado, la caquexia puede ser una ventaja para la longitud del pene.
Penis size has been the subject of curiosity among people throughout history. Variety of studies have been published about penile length in several societies.1–4 Also many studies have investigated penile length and its relationship with somatometric parameters.2,5,6 Obesity affects negatively the person in many ways.4 Also, overweight or obesity adversely affects the development of penis.7 Increasing numbers of obese men complain about their penile size. Although a number of studies have examined the relationship between obesity and penile length, there is no study examining the relationship between cachexia and penile length.2,3,6,8
The aim of the present study was to assess the relationship between penile length and somatometric parameters, especially cachexia.
Materials and methodsAfter getting written consent, weight and heights of all patients, admitted to the internal medicine outpatient clinic due to weight problems, were measured and recorded by an internal medicine specialist in the same device between 10.00 a.m and 2.00 p.m. Urologic examination was performed by a single urologist in these patients in daylight. Examination room temperature is automatically controlled at 25°C with central air condition. Flaccid and stretched states of penis were measured from pubic bone to tip of glans along the dorsum of the penis using a rigid metric ruler by a single urology specialist. Patients with urogenital abnormalities (e.g., varicocele, cryptorchidism, hypospadias, Peyronie’ s disease, penile curvature) were excluded from the study. The penile length was recorded separately. Age, weight and heights were also recorded. Body mass index (BMI) was computed as the ratio of weight to the square of height. Patients were divided into three groups according to body mass index as cachexia, normal weight and obesity. Groups were defined: Group 1: Cachexia BMI<18.5; Group 2: normal weight BMI 18.5 and 25; Group 3: obesity BMI>30.9 Mean and median penile lengths were calculated. These three groups were evaluated in terms of whether there is a difference between flaccid and stretched penile length. Also correlation between weight, height and penile length was determined.
Statistical analyses were performed using the SPSS for windows ver. 16.0 (SPSS Inc., Chicago, IL, USA). The variables were investigated using visual(histograms, probability plots) and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk’ s test) to determine whether or not they are normally distributed. Descriptive analyses were presented using means and standard derivation. As the body weight, BMI, age, flaccid and stretched penile lengths measurements were not distributed the Kruskal–Wallis test were conducted to compare these parameters. The Mann–Whitney U test was performed to test the significance of pairwise differences using Bonferroni correction to adjust for multiple comparisons. Statistical significance was set at p<0.05.
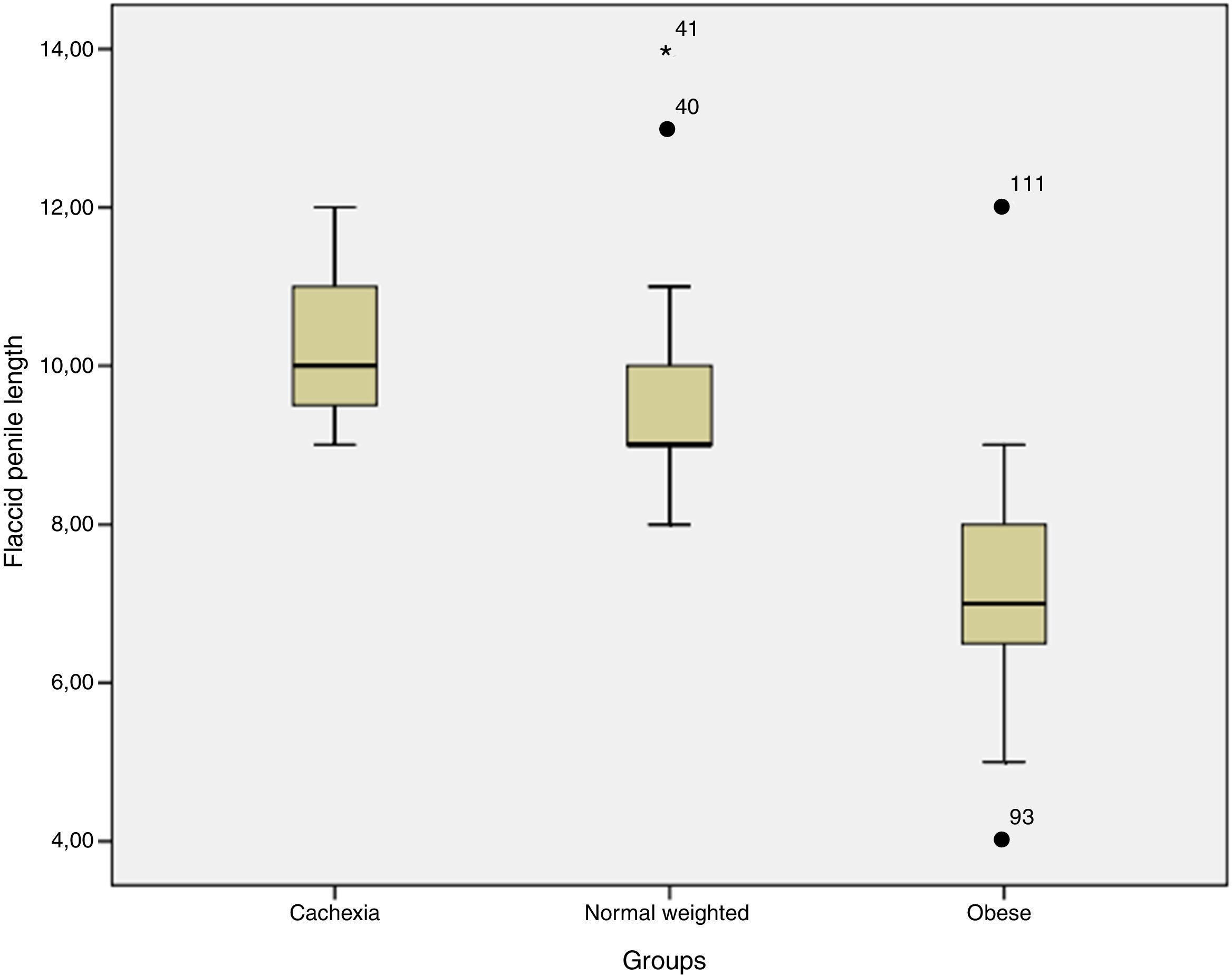
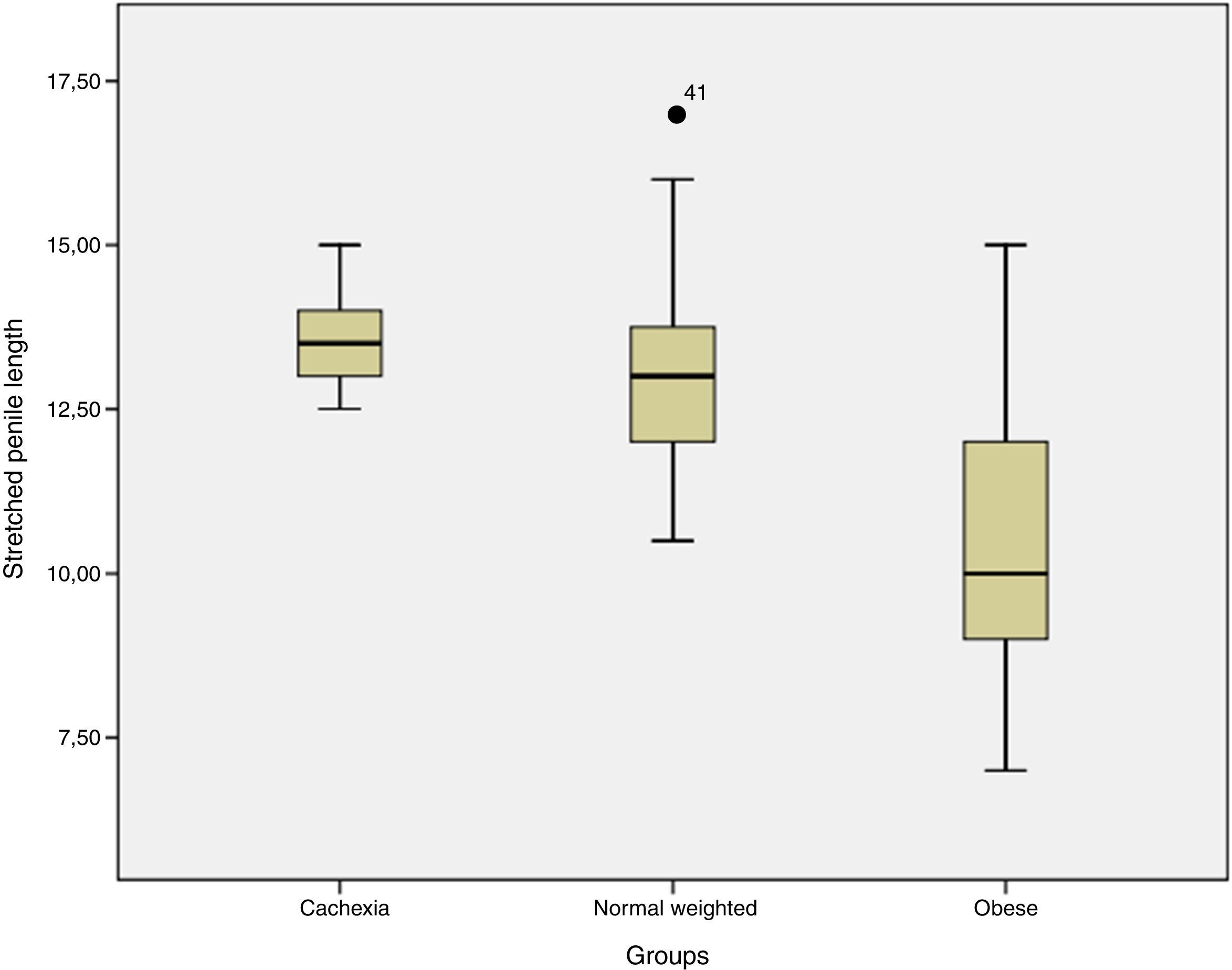
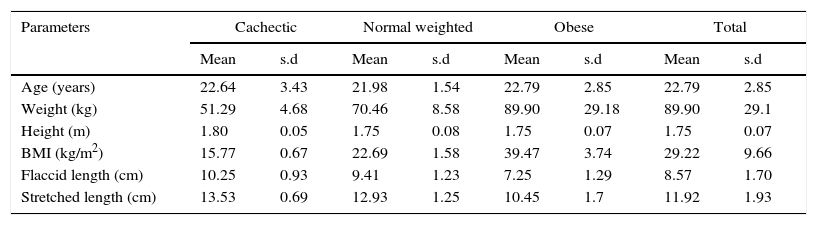
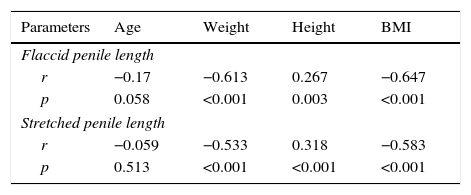
ResultsOne hundred and twenty four patients enrolled in the study between September 2014 and September 2015. Mean age was 22.79±2.85. Mean weight was 89.90±29.1kg. Mean height was 1.75±0.07m. Mean BMI was 29.22±9.66. Mean flaccid penile length was 8.57±1.70cm. Mean stretched penile length was 11.92±1.93cm. Fourteen patients were in cachectic group. Cachectic group's mean age was 22.64±3.43. Mean weight was 51.29±4.68kg. Mean height was 1.80±0.05m. Mean BMI was 15.77±0.67. Mean flaccid penile length was 10.25±0.93cm. Mean stretched penile length was 13.53±0.69cm. Fifty six patients were in normal weighted group. Normal weighted group's mean age was 21.98±1.54. Mean weight was 70.46±8.58kg. Mean height was 1.75±0.08m. Mean BMI was 22.69±1.58. Mean flaccid penile length was 9.41±1.23cm. Mean stretched penile length was 12.93±1.25cm. Fifty four patients were in obese group. Obese group's mean age was 22.79±2.85. Mean weight was 89.90±29.18kg. Mean height was 1.75±0.07m. Mean BMI was 39.47±3.74. Mean flaccid penile length was 7.25±1.29cm. Mean stretched penile length was 10.45±1.70cm (Table 1). Both flaccid and stretched penile lengths were statistically different in these groups (p<0.001; p<0.001) (Kruskall–Wallis test) (Table 2, Figs. 1 and 2). When we compared the groups separately cachectic group's penile lengths were significantly longer than normal weighted group at both (p<0.01; P=0.02) (Mann–Whitney U test). Cachectic group's penile lengths were significantly longer than obese group (p<0.001; p<0.001) (Mann–Whitney U test). Also normal weighted group's penile length’ s were longer than obese group (p<0.001; p<0.001). When we evaluated the correlations between flaccid penis length and other parameters, height and stretched penile length was positively correlated (p=0.003, r=0.267; p<0.001, r=0.916). Weight and BMI was negatively correlated (p<0.001, r=−0.613; p<0.001, r=−647). Age was not correlated (p=0.058, r=−0.17). When we assessed the correlations between stretched penile length and other parameters with spearman's correlation test, height and flaccid penile length was positively correlated (p<0.01, r=0.318; p<0.001, r=0.916). Weight and BMI were negatively correlated (p<0.001, r=−0.533; p<0.001, r=−0.583). Age was not significantly correlated (p=0.51, r=−0.05) (Table 3).
Features of study population.
| Parameters | Cachectic | Normal weighted | Obese | Total | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | s.d | Mean | s.d | Mean | s.d | Mean | s.d | |
| Age (years) | 22.64 | 3.43 | 21.98 | 1.54 | 22.79 | 2.85 | 22.79 | 2.85 |
| Weight (kg) | 51.29 | 4.68 | 70.46 | 8.58 | 89.90 | 29.18 | 89.90 | 29.1 |
| Height (m) | 1.80 | 0.05 | 1.75 | 0.08 | 1.75 | 0.07 | 1.75 | 0.07 |
| BMI (kg/m2) | 15.77 | 0.67 | 22.69 | 1.58 | 39.47 | 3.74 | 29.22 | 9.66 |
| Flaccid length (cm) | 10.25 | 0.93 | 9.41 | 1.23 | 7.25 | 1.29 | 8.57 | 1.70 |
| Stretched length (cm) | 13.53 | 0.69 | 12.93 | 1.25 | 10.45 | 1.7 | 11.92 | 1.93 |
Comparison of penile lengths according to BMI groups.
| Groups | Count | Flaccid penile length | Stretched penile length | Flaccid penile length | Stretched penile length |
|---|---|---|---|---|---|
| Cachectic group | 14 | 10.25±0.93 | 13.53±0.69 | p<0.001 | p<0.01 |
| Normal group | 56 | 9.4±1.23 | 12.93±1.25 | ||
| Obesity group | 54 | 7.2±1.29 | 10.45±1.70 |
Kruskal–Wallis Test.


There were 31 obese patients with concealed penis. Only 23 obese patients did not have concealed penis. We compared these two groups for penile lengths to determine the measurement errors due to suprapubic fat in obese patients with concealed penis. There was no statistically significant difference in both flaccid and stretched penile lengths between these groups (p=0.73, p=0.30) (Mann−Whitney U test). This showed us that our measurements did not affected by suprapubic fat and measurements were correct.
DiscussionPenis size is the power indicator for men. Several men complained about his penis length and went to urology outpatient clinics, although many of them had normal penis length. This situation called small penis syndrome.10 Measurements of the penile length gain importance especially in these people. Flaccid and stretched penile length measurements gives adequate information as erect states.1,11 Therefore, measurements can be done in flaccid and stretched states.
Obesity can affect the penile size due to low androgen levels due to body fat.7 Also excessive adiposity might affect other genital organs negatively, because of high estradiol and low testosterone concentrations.12 Lower weight may be advantage for penile length due to low adipose tissue. Our study showed that cachectic people have longer penile length than normal weighted and obese men (p<0.001).
There are studies about flaccid penile length and weight. Aslan and Promodu found a weak significant correlation.2,8 Ponchietti found a weak negatively correlation.4 We found strong inverse correlation between flaccid penile length and weight and BMI (p<0.001, r=−0.613; p<0.001, r=−0.647). Our results support results of Ponchietti. Correlations between stretched penile length and weight were weak in Aslan and Promodu’ s studies.2,8 Again inverse correlation was detected in Ponchietti’ s study. Our study’ s correlations were inversely strong (p<0.001, r=−0.533; p<0.001, r=−0.583). High adipose tissue in the body causes high estradiol and low testosterone concentrations.12 This adversely affects the development of the penis. Present study showed that less adipose tissue may be advantage for penile length.
Correlation between flaccid penile length and height was evaluated before. Five studies found a weak correlation.2,4–6,13 However one study reported no significant correlation.14 Our study showed a strong correlation between flaccid penile length and height (p=0.003, r=0.267). Five studies found positive correlation between stretched penile length and height.2,4,5,8,13 Our study also showed positive correlation (p<0.01, r=0.318).
Several studies showed no correlation between age and penile length.1–3,6,13–15 Correlation also was not significant in our study in both flaccid and stretched length (p=0.058, r=−0.17; p=0.51, r=−0.05).
At the end we controlled our measurement technique if the suprapubic fat affected the results negatively. But results of men with concealed penis and normal men were similar in both state (p=0.73, p=0.30). In addition flaccid and stretched penile measurements were correlated (p<0.001, r=0.916). This showed us our technique was true.
The main limitation of the study is the small number of cachexia group. However, cachexia is rarely seen in male people. This situation can also be due to it.
ConclusionThere were several studies which evaluated the relationship between penis size and many somatometric paramaters, but present study is the first one assessed the relationship between cachexia and penile length. As a result cachexia may be an advantage for penile length.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interestThe authors declare no conflict of interest.