


Urinary incontinence is a severe and common health problem. In this study, we aimed to assess severity of sexual dysfunction and depression in patients with urinary incontinence.
Materials and methodsThe study has been conducted between 2015 and 2017. Age, body mass index, accompanying health problems, Over Active Bladder (OAB) symptom score, Type of urinary incontinence, Beck Depression Scale were assessed for all patients. International Index of Erectile Function-5 (IIEF-5) was used for male patients in order to assess sexual dysfunction. Index of Female Sexual Function (IFSF) and Female Sexual Distress Scale (FSDS) were used in female patients in order to assess sexual dysfunction.
Results33 patients have been included in the study (Male-12: Urge-10/Stress-1/Mixed-1/Female-21: Urge-10/Stress-6/Mixed-5). Mean age of all patients was 47.9 (Male-49.3/Female-47.2). Mean Body Mass Index for all patients was 23.2 (Male-25.9/Female-21.8). Mean OAB score was 24.3 for all patients (Male-27.5: Urge-28.6/Stress-17/Mixed-27/Female-22.5: Urge-24.2/Stress:21.3/Mixed-20.6). Mean Beck Depression Result for all patients was 20.9 (Male-18.5: Urge-20.2/Stress-9/Mixt-11/Female-22.4: Urge-19.1/Stress-20.3/Mixed-31.6). Mean IIEF-5 score for male patients was 39.5 (Urge-41.4/Stress-55/Mixed-5). Mean IFSF score for female patients was 19.9 (Urge-17.9/Stress-21.3/Mixed-22.4) and mean FSDS score for female patients was 22.1 (Urge-22.3/Stress-23.1/Mixed-20.8).
DiscussionMost of the patients that have been included in the study were diagnosed as urge incontinence. When assessing the OAB scores, they were higher in urge incontinence group. Beck depression results showed higher scores in female patients and it was higher in urge group of male patients and mixt group of female patients. Sexual dysfunction rates were found to be higher for both genders.
La incontinencia urinaria es un problema de salud grave y frecuente. En este estudio se pretende evaluar la gravedad de la disfunción sexual y la depresión en pacientes con incontinencia urinaria.
Materiales y métodosEl estudio se ha realizado entre 2015 y 2017. Edad, índice de masa corporal, problemas de salud concomitantes, puntuación de los síntomas de vejiga hiperactiva, tipo de incontinencia urinaria y escala de depresión de Beck fueron evaluados en todos los pacientes. El índice internacional de la función eréctil 5 (IIEF-5) fue utilizado en los pacientes varones para determinar la disfunción sexual. El índice de la función sexual femenina (IFSF) y la escala sexual femenina de la señal de socorro (FSDS, por sus siglas en inglés) fueron utilizados en pacientes mujeres para determinar la disfunción sexual.
ResultadosTreinta y tres pacientes han sido incluidos en el estudio (varones: 12, ganas: 10, estrés: 1 y mixto: 1; mujeres: 21, ganas: 10, estrés: 6 y mixto: 5). La media de edad de todos los pacientes era de 47,9 (varones: 49,3 y mujeres: 47,2) años. El índice de masa corporal promedio de todos los pacientes fue de 23,2 (varones: 25,9 y mujeres: 21,8). La media de puntuación de vejiga hiperactiva en todos los pacientes fue de 24,3 (varones: 27,5, ganas: 28,6, estrés: 17 y mixto: 27; mujeres: 22,5, ganas: 24,2, estrés: 21,3 y mixto: 20,6). Los resultados de la media de Beck para la depresión de todos los pacientes fue de 20,9 (varones: 18,5, ganas: 20,2, estrés: 9 y mixto: 11; mujeres: 22,4, ganas: 19,1, estrés: 20,3 y mixto: 31,6). La puntuación media IIEF-5 para pacientes varones fue de 39,5 (ganas: 41,4, estrés: 55 y mixto: 5). La puntuación media IFSF para pacientes mujeres fue de 19,9 (ganas: 17,9, estrés: 21,3 y mixto: 22,4) y la puntuación media FSDS para pacientes mujeres fue de 22,1 (ganas: 22,3, estrés: 23,1 y mixto: 20,8).
DiscusiónLa mayoría de los pacientes que han sido incluidos en el estudio fueron diagnosticados con incontinencia de urgencia. A la hora de evaluar las puntuaciones de vejiga hiperactiva fueron más altos en el grupo de incontinencia. Los resultados de la media de Beck para la depresión mostraron puntuaciones más elevadas en pacientes mujeres y fue mayor en el grupo de pacientes varones con ganas y en el grupo de pacientes mujeres con mixto. Las tasas de disfunción sexual se encontraron altas en ambos sexos.
Urinary incontinence (UI) is a severe and common health problem that has many effects on quality of life in terms of many specific points and pathologic conditions. UI is basically the involuntary loss of urine and this condition leads to psychosocial and hygienic problems.1 It is seen nearly 20–30% of people.1 UI was detected as highest in Hispanic women and followed by white, black, Asian-American women.2,3 Also it was found to be higher in African-American women comparing to white women.3 UI would be mainly classified into three groups as urge only, stress only and mixed types.4 Both types are highly prevalent.5 All these types of incontinence affect the quality of life but it was found that mixed type was mostly affecting.6 UI was found to be strongly associated with depression and sexual dysfunction that causes both personal and familial problems.7 This pathology has also negative effect on the economy of countries.7 Many studies have been conducted in order to show these relations. Sutherst et al. mentioned about the adverse effect of incontinence on sexual life and they found that bladder instability was causing higher dysfunction rates.8 These patients have a strong fear to face UI episode during the intercourse.5 UI is also strongly associated with depression and in a study it was found that women with depression were more likely to mention about their incontinence problems.9 In some studies it is claimed that there is role of monoamines in these three pathologic entities.10 There are validated scoring systems for assessing these entities reported and validated in the literature. OAB-v8 is one of these questionnaires that is consisting of patient-reported outcomes and it gives information about symptom bother.11 Index of Female Sexual Function (IFSF) is a multidimensional tool that is assessing sexual function in women and mainly reporting outcomes about discomfort, dryness, attempts, desire, desire level, satisfaction, satisfaction with partner, orgasm frequency and clitoral sensation.12,13 Female Sexual Distress Scale (FSDS) is used to assess sexually caused distress in women.14 Studies showed the validity of this scale.14 In our study we have used the revised version of FSDS consisting of 13 questions.15 International index of erectile function (IIEF) is a diagnostic tool for assessing the male sexual function.16 According to IIEF, five severity degrees were described for erectile dysfunction.16 Beck Depression Inventory is a widely used tool for screening depression and it is worldwide tool that was validated with many studies.17 In this study, we aimed to assess severity of sexual dysfunction and depression in patients with urinary incontinence. We have used validated questionnaires and scales for screening the status of patients. Also the patients were divided into groups regarding to the types of urinary incontinence for both genders.
Materials and methodsThe study has been conducted in Kecioren Research and Training Hospital between 2015 and 2017. Age, body mass index, accompanying health problems, Over Active Bladder symptom score (OABv8), type of urinary incontinence, Beck Depression Scale were assessed for all patients. OABv8 is consisting of 8 questions, 5 scores for each questions and if the score is 8 or greater it reveals the presence of over active bladder. This questionnaire was conducted for all patients in order to assess their results and for comparison. Beck Depression Scale is consisting of 21 questions and it is used for evaluating depression. There are 4 scores for each questions from 0 to 3 and there are 6 groups for grouping the severity of depression. 1–10 are considered to be normal, 11–16 shows mild mood disturbance, 17–20 shows borderline clinical depression, 21–30 shows moderate depression, 31–40 shows severe depression and over 40 score means extreme depression. Urinary incontinence types are mainly classified into three groups as urge, stress and mixed types. International Index of Erectile Function (IIEF) was used for male patients in order to assess sexual dysfunction. IIEF questionnaire is consisting of 15 questions, questions are assessing erectile function, orgasmic function, sexual desire, intercourse satisfaction, overall satisfaction and 1–10 scores show severe erectile dysfunction, 11–16 shows moderate dysfunction, 17–21 shows mild to moderate dysfunction, 22–25 shows mild dysfunction and 26–30 shows no dysfunction. Index of Female Sexual Function (IFSF) and Female Sexual Distress Scale (FSDS) were used in female patients in order to assess sexual dysfunction. Index of Female Sexual Function (IFSF) is consisting of 9 questions with 5 scores for each that is used to assess sexual function of women. The scores were classified into three groups as under 15, 15–25, 25–35 and over 35. Lower scores show sexual dysfunction in women and it was pointed in several studies that if the score is under 30, it indicates sexual dysfunction in Turkish population. Revised Female Sexual distress Scale is consisting of 13 questions and if the score is over 11 it shows distress of women. The scale was validated in studies and was found to be suitable to use for female patients in Turkey.18 In our study, sexually active, male and female patients with urinary incontinence were included in the study. Sexually inactive patients and patients that were sexually active but did not have any type of urinary incontinence were excluded from the study. The scientific studies are mainly assessed in four categories according to the guide for Revista Internacional de Andrologia and these categories are epidemiologic studies, qualitative methodology articles, mixed methodology articles and review articles.19 Our study is mainly included in the first group, epidemiologic studies.19
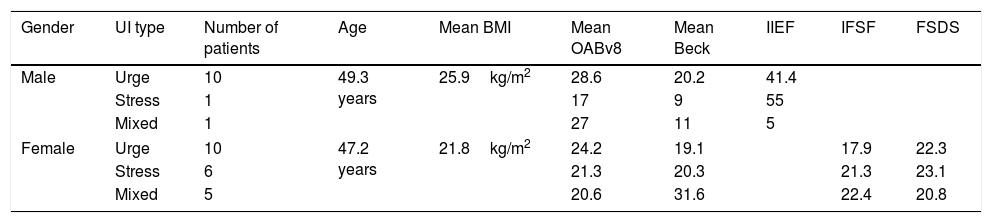
Results33 patients have been included in the study (Male-12: Urge-10/Stress-1/Mixed-1, Female-21: Urge-10/Stress-6/Mixed-5). Mean age of all patients was 47.9 (Male-49.3/Female-47.2). Mean Body Mass Index for all patients was 23.2 (Male-25.9/Female-21.8). All the scores were classified into groups according to incontinence types (Table 1). Mean OAB score was 24.3 for all patients (Male-27.5: Urge-28.6/Stress-17/Mixed-27, Female-22.5: Urge-24.2/Stress:21.3/Mixed-20.6). Mean Beck Depression Result for all patients was 20.9 (Male-18.5: Urge-20.2/Stress-9/Mixed-11/Female-22.4: Urge-19.1/Stress-20.3/Mixed-31.6). Mean IIEF score for male patients was 39.5 (Urge-41.4/Stress-55/Mixed-5). Mean IFSF score for female patients was 19.9 (Urge-17.9/Stress-21.3/Mixed-22.4) and mean FSDS score for female patients was 22.1 (Urge-22.3/Stress-23.1/Mixed-20.8).
Incontinence types and scores.
| Gender | UI type | Number of patients | Age | Mean BMI | Mean OABv8 | Mean Beck | IIEF | IFSF | FSDS |
|---|---|---|---|---|---|---|---|---|---|
| Male | Urge | 10 | 49.3 years | 25.9kg/m2 | 28.6 | 20.2 | 41.4 | ||
| Stress | 1 | 17 | 9 | 55 | |||||
| Mixed | 1 | 27 | 11 | 5 | |||||
| Female | Urge | 10 | 47.2 years | 21.8kg/m2 | 24.2 | 19.1 | 17.9 | 22.3 | |
| Stress | 6 | 21.3 | 20.3 | 21.3 | 23.1 | ||||
| Mixed | 5 | 20.6 | 31.6 | 22.4 | 20.8 | ||||
Urinary incontinence is a common urological disorder that affects a large population and their quality of life.20 There are different types of UI and for identifying the type validated questionnaires and clinical tools are used.20 This pathologic entity is seen at nearly all ages but it increases with age.21 There are some consequences of UI as worse quality of life, familial problems, stress, depression and sexual dysfunction.7 Most of the patients that have been included in our study were diagnosed as urge incontinence. When assessing the OAB scores, they were higher in urge incontinence group. There are several studies that are assessing the relations between sexual dysfunction, depression and incontinence also the difference between types of incontinence.22 In a study conducted by Chiara et al. there were no difference in terms of Beck depression scores between types of in continence for female patients.23 In contrast to this outcome, Stach-Lempinen et al. indicated higher scores in urge incontinence group when comparing to stress incontinence for female patients.24 In our study, Beck depression results showed higher scores in female patients and while assessing male patients the scores were higher in urge incontinence group but for female patients the scores were higher in mixed incontinence group comparing to urge and stress group. Studies were also conducted to show the relation between sexual dysfunction for the patients with UI. Duralde et al. evaluated female patients with UI for sexual dysfunction and they found that patients with mixed UI had higher sexual dysfunction rates.25 In another study, women were found to be negatively affected in terms of sexual function and the most affected points were found to be desire, lubrication, orgasm and sexual satisfaction.26 In our study, IFSF and FSDS scores were used to assess the relation for female patients. IFSF and FSDS scores showed the presence of sexual dysfunction and similar results for all incontinence subtypes. For male patients several factors are affecting this relation. Studies showed that for the male patients that had radical prostatectomy, foreplay incontinence was a severe problem with higher rates (38%).27 In out study IIEF was used to assess male patients. IIEF scores showed higher dysfunction rates for mixed group. But more patient numbers needed in order to make a decision.
LimitationsThe number of patients that was included in the study would be increased and that would reveal better results. Control groups were not included in the study because there are scales fort he validated tools that were used. Large patient groups including controls would be compared in the future studies.
ConclusionAll the validated scales and scoring systems showed the presence of depression and sexual dysfunction for both genders with different types of urinary incontinence. It is very important to consider these pathologic entities that would be seen together while designing the treatment strategies.
Conflict of interestsThe authors declare no conflict of interests.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.