

This study analyzed the importance of exercise frequency on eating disordered behaviors and psychological well-being and the ability of various exercises, individual, and psychological variables to predict eating disordered behaviors. The following characteristics were measured: eating disordered behaviors, dieting habits, physical activity, goal orientation, social physique anxiety, and self-esteem. The results showed that regular exercise was reported more frequently by males, those with high attraction towards exercise, and adolescents with fewer dieting behaviors. Moreover, adolescents who exercised regularly showed fewer eating disordered behaviors and had more positive psychological functioning. The results also confirmed the importance of various exercises, individual, and psychological variables in predicting eating disordered behaviors. In conclusion, this study validates the importance of regular exercise for promoting psychological well-being and preventing eating disordered behaviors in adolescence.
Este estudio se realizó en una muestra de 192 adolescentes portugueses. Se analizó la importancia de la frecuencia de la práctica en conductas alimentarias y en el bienestar psicológico. Además, se intenta explicar las conductas alimentarias tomando en consideración las características deportivas, individuales y psicológicas. Las variables evaluadas fueron: los trastornos de la conducta alimentaria, la tendencia a realizar dietas, las rutinas en la práctica de ejercicio, la orientación de objetivos, la ansiedad física social y la autoestima. Los resultados mostraron que mantenían una práctica regular de ejercicio principalmente los adolescentes varones, quienes tenían una atracción positiva por el ejercicio y menor tendencia a conductas dietéticas. También se ha encontrado que el grupo con práctica regular de ejercicio presentaba menos trastornos de la conducta alimentaria, así como un mejor funcionamiento psicológico. La predicción de perturbaciones alimentarias confirma la importancia de las variables deportivas, individuales y psicológicas. En resumen, los resultados confirmaron la importancia de la práctica de ejercicio no solo en términos de bienestar psicológico, sino también en la prevención de conductas alimentarias problemáticas en adolescentes.
Exercise has been positively associated with physical health and psychological well-being (Hagger, 2010). These effects have been well documented among adults, but less evidence exists regarding the benefits of exercise among younger people (Sallis, Prochaska & Taylor, 2000). According to Fox (2000), exercise may be an effective way for children and adolescents to develop a positive self-image and has the greatest potential to be effective when it is presented in a way that encourages mastery and self-development. Despite these positive findings, there is evidence that young people do not exercise enough or that they simple do not sufficiently incorporate physical activity into their lifestyles (Griffiths et al., 2013; Hills, Andersen & Byrne, 2011).
Thus, it is necessary to understand the psychological processes that are involved in engaging in a physically active lifestyle among adolescents (Hagger, 2010). Identifying the psychological factors related to physical activity among youths is important for public health and can help increase the number of young people who meet health-related physical activity guidelines (Davies, Gregory & White, 1995). Moreover, it is important to understand the relation between exercise frequency and various individual and psychological variables for adolescents, as well as the relation between these variables and health-related behaviors, such as eating disordered behaviors (e.g., eating restraint, binge eating, induced vomiting, and laxative use). According to previous research, exercise frequency is related to body dissatisfaction as well as the development and maintenance of eating problems and eating disorders (Garner, Rosen & Barry, 1998; Gonçalves & Gomes, 2012).
This study has two main purposes. First, the association between adolescents’ exercise frequency and various individual variables was analyzed, with particular attention to individual differences in eating disordered behaviors and psychological factors. Second, eating disordered behaviors were examined by taking into account exercise frequency as well as significant individual and psychological characteristics.
Regarding the first aim of this study, the association between exercise frequency and various individual characteristics was analyzed to determine whether adolescents who regularly practice exercise and those who do not differ in terms of their eating disordered behaviors and on various psychological variables (e.g., goal orientation, social physique anxiety, and self-esteem). Eating disordered behavior was assessed because of our interest in determining whether adolescents with different levels of exercise frequency differ in terms of eating disordered behaviors. Such differences may occur because adolescence is marked by changes in lifestyle that may lead to new eating behaviors (Rodríguez et al., 2001). Thus, it becomes important to know whether exercise frequency is related to eating disordered behaviors during adolescence.
Goal orientation, social physique anxiety, and self-esteem were examined because of their importance in explaining an individual's propensity to exercise. Regarding goal orientation, motivation tends to be positively correlated with physical exercise (Kilpatrick, Hebert & Bartholomew, 2005), and some authors have argued that goal setting is an important factor determining participation in physical activity (Harwood, Wilson & Hardy, 2002; Kilpatrick, Bartholomew & Riemer, 2003). In this study, we examined adolescents’ goal orientation regarding exercise by assessing participant's task orientation (e.g., success in exercise based on self-referenced criteria such as increasing effort) and ego orientation (e.g., success in exercise based on the adequacy of one's personal ability and the demonstration of one's superior competence compared with other exercisers) (Petherick & Markland, 2008).
Social physique anxiety is an important self-presentational concern for adolescents. In fact, a fear about physical appearance appears to be central to adolescents’ sense of self-worth and has the potential to affect their overall well-being (Caglar, Bilgili, Karaca, Ayaz & Ayaz, 2010). Thus, exercise frequency may be related to adolescents’ perception of their social physique.
With regard to self-esteem, differences between exercisers and non-exercisers in terms of self-esteem have been widely reported (Scully, Kremer, Meade, Graham & Dudgeon, 1998). However, less evidence exists regarding the differences in self-esteem between adolescents who exercise occasionally and those who exercise regularly.
The second aim this study was to predict eating disordered behaviors based on both exercise frequency (e.g., occasional and regular exercise) and individual characteristics (e.g., gender, BMI, desired ideal weight, and attraction toward exercise). These individual variables were selected based on their importance in explaining eating disordered behaviors (see Gomes, Martins & Silva, 2011; Grieve, Wann, Hensen & Ford, 2006; Hausenblas & McNally, 2004; Sanford-Martens et al., 2005). In addition, we included psychological variables (e.g., goal orientation, social physique anxiety, and self-esteem) in the regression model in order to analyze the predicted value of these variables for eating disordered behaviors. All these variables were included in the model to explain the multiple effects of exercise, individual, and psychological variables on eating disordered behaviors. As noted by Cusatis and Shannon (1996), it is crucial for studies to identify more variables that can help explain eating disordered behaviors of adolescents because previous research has incorporated a limited number of variables and thus has provided an incomplete and overly simplistic depiction of this phenomenon.
Finally, we defined two groups for these analyses (i.e., occasional and regular exercise groups). Our main concern here was the possibility of error due to misclassification bias. In fact, assessing physical activity in children and youths based on self-report information is known to be difficult and subject to classification errors (Pate, 1993). This concern seems relevant when self-report measures are used to assess adolescents’ physical exercise over several weeks. In this case, participants may overestimate their exercise routines by indicating their desired amount of exercise rather than their actual amount of exercise. Thus, in order to prevent this problem from occurring, the participants’ exercise ratings for a recent period of time (i.e., the last week) were used as the definition criteria in both the occasional and the regular exercise groups.
More specifically, four goals were established for this study:
- •
Analyze the associations between exercise frequency and various individual characteristics (e.g., gender, BMI, desired ideal weight, attraction toward exercise, and dieting behavior).
- •
Analyze the differences between the occasional and the regular exercise groups in terms of their eating disordered behaviors and propensity for eating disordered behavior.
- •
Analyze the differences between the occasional and the regular exercise groups regarding goal orientation, social physique anxiety, and self-esteem.
- •
Analyze the psychological predictors of eating problems after controlling for relevant exercise and individual characteristics.
A convenience sample was recruited from three public schools on the island of Pico (Azores, Portugal). The total sample consisted of 248 high school students (7th-12th grade, ages between 13 and 18 years old). However, on the basis of the information obtained in the Physical Activity Questionnaire for Adolescents, 50 participants were excluded because they did not record their exercise in the last week due specific reasons not related to their life style (e.g., illness, family problems). Thus, the sample was reduced to 192 participants (53.1% female, n=102), who were then divided into two groups: the occasional exercise group (i.e., maximum of two periods of exercise in the last week) and the regular exercise group (i.e., minimum of three periods of exercise in the last week).
In the occasional exercise group, there were 109 participants (56.8%), with 70 females (64.2%). The ages were between 13 and 18 years old (Mean, 15.5±1.48). Data on participants’ body mass index (BMI) was also collected for each group. The BMI is a measure of the human body shape based on an individual's weight and height — weight (kilograms) / height (meters)2. BMI categories include underweight (≤ 18.5), normal weight (18.5–24.9), overweight (25–29.9), and obese (≥ 30). The majority of the participants in the occasional exercise group were normal weight (n=69, 63.3%), 11 (10.1%) were below normal weight, and 29 (26.6%) were overweight. 56% (n=61) reported a desire to weigh less than their current weight, 27.5% (n=30) reported a desire to remain the same weight, and 16.5% (n=18) reported a desire for an ideal weight greater than their current one; 78 participants (71.5%) reported having moderate to high attraction toward exercise.
In the regular exercise group, there were 83 participants (43.2%), with 32 females (38.6%). The ages were between 13 and 18 years old (mean, 15.7±1.41). The majority of the participants were normal weight (n=48, 57.8%), 26 (31.3%) were overweight, and 9 (10.9%) were below normal weight. In addition, 44.6% (n=37) reported a desire to weigh less than their current weight, 39.8% (n=33) reported a desire to remain the same weight, and 14.5% (n=12) reported a desire for an ideal weight higher than their current one (one participant did not report information for this variable); 82 participants (98.7%) reported having moderate to high attraction toward exercise.
MeasuresDemographic and exercise information. This questionnaire was developed for the current study in order to collect personal information on the participants (e.g., gender, age, weight, height, and desired ideal weight). Self-reported current weight and height were used to determine the BMI, and the participants were asked to indicate whether they liked to exercise using in a Likert scale (0=“not at all”, 3=“very much”). This score represents “attraction toward exercise”.
Eating Disorder Examination Questionnaire (EDE-Q) (Fairburn & Beglin, 1994; Portuguese adaptation byMachado, 2007). This instrument is a self-report version of the Eating Disorder Examination, a well-established investigator-based interview (Fairburn & Cooper, 1993). This version comprises 28 items answered on a seven-point Likert scale ranging from 0 (“none”) to 6 (“every day”). The EDE-Q includes four subscales reflecting the severity of aspects related to pathological eating disordered behaviors that have occurred in the past 28 days: namely, restraint (α=.74), eating concern (α=.74), shape concern (α=.86), and weight concern (α=.75). Higher scores in each dimension are indicative of a greater propensity for eating disordered behaviors. A global score was also calculated from the average of the four subscale scores (α=.92). The EDE-Q also included six items assessing specific behaviors related to eating disorders, and four of these items evaluated binge-eating and compensatory behaviors that occurred over the past 28 days.
Dieting Status Measure (DiSM) (Strong & Huon, 1997; Portuguese adaptation byGomes, 2010a). This instrument presents six statements describing dieting behavior, ranging from “I have never dieted in order to lose weight” to “I am always dieting in order to lose weight.” Participants were asked to select the statement that best described their current situation. The following responses were used to define their dieting status: 1=never dieters, 2=dieters, 3=ex-dieters, 4=sometimes dieters, 5=often dieters, and 6=always dieters.
Physical Activity Questionnaire for Adolescents (PAQA) (Kowalski et al., 1997; Portuguese adaptation byGomes, 2010bGomes, 2010b). For the purpose of this study, we used two items from this questionnaire. The first assessed the frequency of physical activity in the last 7 days (“last week”), and the second evaluated the occurrence of specific problems that could have prevented exercise in the past 7 days (“last week”) (e.g., illness, significant life changes). On the basis of the results of the first item, two groups were created: the occasional exercise group corresponds to a maximum of two periods of exercise in the last week, and the regular exercise group corresponds to a minimum of three periods of exercise in the last week. The second question had two response options: “Nothing happened to me that prevented me from exercising” and “I could not do exercise”.
Goal Orientation in Exercise Measure (GOEM) (Petherick & Markland, 2008; Portuguese adaptation byGomes & Capelão, 2013). This instrument evaluated exercisers’ goal orientation, which represents individual differences in the way that people construe their perception of success related to physical activity. Two major goal perspectives were evaluated: task-oriented goals (α=.90) and ego-oriented goals (α=.90). This version of the GOEM comprises ten items answered on a five-point Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Higher scores in each dimension are indicative of greater orientation toward task and ego goals.
Social Physique Anxiety Scale-Revised (SPAS-R) (Hart et al., 1989; Portuguese adaptation byGomes, 2010c). This instrument was originally developed as a 12-item measure, but a 9-item version was later proposed by Martin, Rejeski, Leary, McAuley and Bane (1997). The SPAS-R measures the degree of anxiety that a person experiences when he or she perceives that his or her physique is being evaluated or observed by others (Hart et al., 1989). Participants were asked to indicate the degree to which each statement was true of them on a 5-point Likert scale ranging from 1 (“not at all”) to 5 (“extremely”). A global score was calculated, with higher scores indicating more social physique anxiety (α=.92).
Rosenberg Self-Esteem Scale (RSE) (Rosenberg, 1965; Portuguese adaptation byRomano, Negreiros, & Martins, 2007). The RSE Scale is a 10-item self-report questionnaire that assesses self-esteem using a four-point scale from 1 (“strongly disagree”) to 4 (“strongly agree”). Higher scores represented higher self-reported levels of self-esteem (α=.87).
ProcedureThe study followed ethical procedures as outlined in the Declaration of Helsinki (version from 2008). Data collection involved the following steps: (a) permission was requested from the Portuguese Ministry of Education and the regional school authorities; (b) the school directors were contacted to inform them about the research project and to ask their permission to collect data, and (c) the schools were visited by the research team to discuss the data collection with teachers and students. The research was presented as a study about the relationship between physical activity habits and the psychological factors as well as eating disordered behaviors of adolescents. Informed consent was obtained from students, and in the case of young students (less than 18 years of age), their parents/guardians also signed the consent forms. The evaluation protocol was completed at the schools during one class after receiving permission from the teacher. All participants were informed that their participation was voluntary and anonymous. Three hundred questionnaires were distributed, and 248 were collected and were considered valid (the return rate was 77.7%). Please note that as described in the “participants section” from these 248 questionnaires, 50 were later excluded because these participants did not record their exercise frequency in the last week.
ResultsAssociations between individual variables and physical activityIn the first set of analyses, we tested the association between exercise groups (i.e., occasional and regular exercise) and participants’ gender, BMI, desired ideal weight, attraction toward exercise, and dieting behavior. χ2 tests and logistic regression analyses were conducted to test these associations.
A significant association was found between the exercise group and participants’ gender (X2(1)=12.47; p < .001); female adolescents were more likely to exercise occasionally (n=70, 68.6%), whereas males were more likely exercise regularly (n=51, 56.7%). In fact, male adolescents were 2.86 times more likely to exercise regularly (Wald X2=12.168; p < .001; OR=2.86).
There were no statistically significant differences between the exercise groups in terms of BMI (X2(1)=.51, n.s.), for which two BMI groups were created (normal weight vs. overweight). In addition, no statistically significant differences were found between the exercise groups in terms of desired ideal weight (X2(1)=2.20, n.s.), for which two groups based on desired ideal weight were created (e.g., desire to weigh less than the current weight vs. desire to remain the same weight and desire for an ideal weight higher than the current one).
A significant association was found between the exercise group and participants’ attraction toward exercise (X2(1)=25.17; p < .001). In this case, almost 97% (n=31) of the adolescents that reported having a low attraction toward exercise were in the occasional exercise group, and 51.3% (n=82) of the adolescents that reported having a high attraction toward exercise were in the regular exercise group. Adolescents with a high attraction toward exercise were significantly more likely to exercise regularly (Wald X2=18.887; p < .001; OR=2.52).
Last, we found a marginally statistically significant association between the exercise group and participants’ propensity for dieting behavior (X2(1)=3.00; p < .10). The results indicated that 69% of those who reported dieting (sometimes, often, and always; n=29) were in the occasional exercise group. The difference between exercise groups regarding the propensity for dieting behavior was less evident among those who did not report dieting, with 53.4% (n=55) in the occasional exercise group and 46.6% (n=48) in the regular exercise group.
Physical activity and eating disordered behaviorsThe purpose of these analyses was to test for differences between the occasional and the regular exercise groups in terms of eating disordered behaviors. To evaluate whether such differences exist, we applied t-tests for independent samples to the global score of the instruments and a multivariate analysis of variance to the subscales of the multidimensional instruments. This same procedure was also used in the next analysis reported in this paper.
Multivariate tests revealed differences between the groups on the EDE-Q subscales (Wilks’ λ=0.91; F(4,165)=4.17; p < .01; X2=0.09). Univariate tests showed that the adolescents in the occasional exercise group scored higher than the adolescents who were regular exercisers on the shape concern subscale and on the weight concern subscale (but with the weight concern subscale, the differences were only marginally significant). In the same way, the occasional exercise group scored higher on the EDE-Q global score (but again, the differences were only marginally significant). These differences are presented in table 1.
Differences between the groups in eating disordered behaviors and psychological dimensions
| Occasional exercise | Regular exercise | g.l. | F / t | |||
|---|---|---|---|---|---|---|
| M (SD) | n | M (SD) | N | |||
| EDE-Q: Eating disorder | (1,168) | |||||
| EDE-Q: Restraint | .85 (1.01) | 93 | .97 (1.26) | 77 | .48 | |
| EDE-Q: Shape concern | 1.89 (1.72) | 93 | 1.25 (1.50) | 77 | 6.47a | |
| EDE-Q: Eating concern | .61 (.76) | 93 | .55 (88) | 77 | .25 | |
| EDE-Q: Weight concern | 1.84 (1.75) | 93 | 1.40 (1.60) | 77 | 2.95b | |
| EDE-Q: Global score | 1.37 (1.23) | 109 | 1.04 (1.19) | 83 | (190) | 1.88b |
| GOEM: Goal orientation | (1,184) | |||||
| GOEM: Task | 3.44 (.95) | 108 | 3.98 (.92) | 78 | 15.14c | |
| GOEM: Ego | 1.78 (.87) | 108 | 2.30 (1.06) | 78 | 13.64c | |
| SPAS-R: Physiq. anxi. | (188) | |||||
| SPAS-R: Global score | 2.60 (1.16) | 107 | 2.16 (1.10) | 83 | 2.65d | |
| RSE: Self-esteem | (188) | |||||
| RSE: Global score | 2.78 (0.62) | 109 | 3.12 (0.56) | 81 | –3.95c | |
In the next step, we used X2 tests to analyze the associations between exercise frequency (e.g., occasional and regular exercise) and specific behaviors related to eating disorders, as assessed by the EDE-Q (“diagnostic items”). We found one marginally significant difference in the diagnostic criteria of the EDE-Q between the groups over the last four weeks (table 2). Moreover, from the reported frequencies of binge eating and purging (e.g., self-induced vomiting and laxative use), 26 participants (13.5%) appeared to meet the diagnostic criteria for a binge eating disorder, with 20 of these participants (76.9%) in the occasional exercise group. Additionally, 10 participants (5.21%) appeared to meet the diagnostic criteria for nonpurging type bulimia nervosa, with six of these participants (60%) in the occasional exercise group, and 11 participants (5.73%) appeared to meet the diagnostic criteria for purging type bulimia nervosa, with six of these participants (55.5%) in the regular exercise group.
Percentage of participants in the occasional exercise group and the regular exercise group reporting EDE-Q diagnostic items
| EDE-Q: Diagnostic items | Occasional exercise | Regular exercise | |||
|---|---|---|---|---|---|
| No, n (%) | Yesa, n (%) | No, n (%) | Yesa, n (%) | X2 | |
| 13. Ingestion of a large amount of food | 55 (50.9) | 53 (49.1) | 32 (38.6) | 51 (61.4) | 2.90b |
| 14. Loss of control over eating | 57 (52.8) | 51 (47.2) | 47 (56.6) | 36 (43.4) | .28 |
| 15. Ingestion of a large amount of food with loss of control | 56 (51.9) | 52 (48.1) | 50 (60.2) | 33 (39.8) | 1.34 |
| 16. Self-induced vomiting in order to control weight and shape | 101 (93.5) | 7 (6.5) | 76 (91.6) | 7 (8.4) | .26 |
| 17. Use of laxatives in order to control weight and shape | 102 (94.4) | 6 (5.6) | 73 (88.0) | 10 (12.0) | 2.58 |
| 18. Excessive exercise in order to control weight and shape or “burn” calories | 77 (71.3) | 31 (28.7) | 53 (63.9) | 30 (36.1) | 1.20 |
The next analysis tested for differences between the occasional and the regular exercise groups regarding the remaining psychological dimensions (i.e., goal orientation, social physique anxiety, and self-esteem).
We found differences between the groups in the subscales of the GOEM instrument (Wilks’ λ=.89; F(2,183)=11.38; p < .001; X2=.11). Univariate tests revealed that the regular exercise group reported having more task motivation and ego motivation. On the contrary, the regular exercise group reported having less social physique anxiety. In addition, adolescents who were regular exercisers scored significantly higher than the adolescents who occasionally exercised on the RSE instrument, indicating that regular exercisers had higher self-esteem. These differences are presented in table 1.
Predictors of eating disordersTo predict eating disordered behaviors, we applied a regression analysis with blocked entry procedures, controlling for exercise variables (e.g., exercise frequency) and individual variables (e.g., gender, BMI, desired ideal weight, and attraction toward exercise). In the final block, we introduced the psychological variables (e.g., goal orientation regarding exercise, social physique anxiety, and self-esteem). The tested model showed no problems of multicollinearity and normality (Tabachnick & Fidell, 2001).
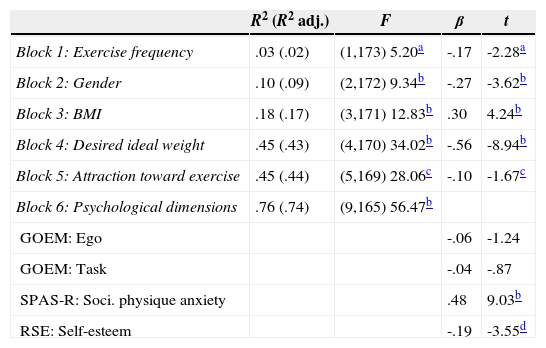
In the first block, we controlled for participants’ exercise frequency, and the model was found to be significant and explained 2% of the variance. Thus, adolescents with less frequent exercise reported having more eating disordered behavior. In the second block, we controlled for gender, and the model was found to be significant, with 9% of the variance explained. Female adolescents reported having more eating disordered behavior than males. When BMI was added to the regression in the third block, the model accounted for 17% of the variance, and it was found to be statistically significant. Overweight adolescents also reported having more eating disordered behavior. In the fourth block, we added participants’ desired ideal weight, and the model was significant and explained 43% of the variance. In this case, adolescents with a desire to weigh less had a greater propensity for eating disorder behavior. In the fifth block, we added attraction toward exercise, and the model was only marginally significant and explained 44% of the variance. In this case, low attraction toward exercise predicted eating problems (but the values were only marginally significant). In the final block, we added the psychological variables, and the model was statistically significant, with 74% of the total variance explained. After taking into account the effects of individual and exercise variables, both social physique anxiety and self-esteem emerged as significant predictors. Thus, higher social physique anxiety and lower self-esteem predicted a propensity for eating disorder behavior. The results of these analyses are summarized in table 3.
Regression model for the prediction of the EDE-Q global score
| R2 (R2 adj.) | F | β | t | |
|---|---|---|---|---|
| Block 1: Exercise frequency | .03 (.02) | (1,173) 5.20a | -.17 | -2.28a |
| Block 2: Gender | .10 (.09) | (2,172) 9.34b | -.27 | -3.62b |
| Block 3: BMI | .18 (.17) | (3,171) 12.83b | .30 | 4.24b |
| Block 4: Desired ideal weight | .45 (.43) | (4,170) 34.02b | -.56 | -8.94b |
| Block 5: Attraction toward exercise | .45 (.44) | (5,169) 28.06c | -.10 | -1.67c |
| Block 6: Psychological dimensions | .76 (.74) | (9,165) 56.47b | ||
| GOEM: Ego | -.06 | -1.24 | ||
| GOEM: Task | -.04 | -.87 | ||
| SPAS-R: Soci. physique anxiety | .48 | 9.03b | ||
| RSE: Self-esteem | -.19 | -3.55d |
Attraction toward exercise: 0-Low attraction, 1-High attraction; BMI: 0-Normal weight, 1-Overweight; Desired ideal weight: 0-Lower than the current weight, 1-Same or higher than current weight; Exercise frequency: 0-Occasional exercise, 1-Regular exercise; Gender: 0-Female, 1-Male.
This study had two main aims. First, we analyzed the association between exercise and adolescents’ individual characteristics and tested whether exercise frequency is affected by differences in eating disordered behaviors and psychological functioning. Then, we assessed the predictive ability of exercise, individual, and psychological variables in explaining eating disordered behaviors.
Regarding the first aim, three findings should be stressed. First, being male, having a higher attraction toward exercise, and having a lower propensity for dieting were associated with a greater likelihood of exercising regularly among the adolescents. Some of these findings are consistent with those of other studies, in that females consistently report having a lower exercise frequency than boys (Troiano et al., 2008; Whitt-Glover et al., 2009). Moreover, almost 97% of the adolescents that reported having a low attraction toward exercise also exercised occasionally, and only one adolescent (1.2%) with regular physical activity reported having a low attraction toward exercise. Thus, enjoyment and leisure clearly are important for participation in exercise, which reinforces the need for pleasure and fun in programs that promote physical activity in young people.
Second, adolescents with a pattern of occasional exercise reported having more eating disordered behaviors (particularly in the shape concern subscale of the EDE-Q). Despite finding no significant difference between the groups in the diagnostic criteria of the EDE-Q, we should note that the higher percentage of possible cases of binge eating disorder and nonpurging-type bulimia nervosa were found in the occasional exercise group. These results as well as our finding that adolescents’ propensity for dieting is associated with occasional exercise highlight the value of exercise in promoting health. Few studies have examined the relationship between exercise frequency and eating disordered behaviors in such detail. However, in one study with US adolescents, Pate, Heath, Dowda and Trost (1996) concluded that low physical activity was associated with unhealthy habits, including excessive dietary behavior. Overall, and perhaps most important, our results reinforce the advantages of adolescents’ participation in exercise for fun, fitness, and social interaction (Smolak, Murnen & Ruble, 2000).
Third, the regular exercise group was more motivated to exercise, had less social physique anxiety, and higher self-esteem. These results support the importance of goal orientation not only for sport participation (Harwood et al., 2002) but also for exercise participation among adolescents (Kilpatrick et al., 2003). In the same way, our results regarding self-esteem confirm previous findings of a positive association among self-esteem, exercise participation, and sport involvement (e.g., Ekeland, Heain & Hagen, 2005; Parfitt & Eston, 2005; Penedo & Dahn, 2005). Our results indicate that such these differences self-esteem also extend to adolescents with different exercise frequencies. Moreover, the fact that adolescents who exercise regularly had less social physique anxiety is important because research has demonstrated that social physical anxiety is associated with both low exercise frequency and excessive exercise, negative perfectionism, and socially prescribed perfectionism (Caglar et al., 2010; Haase Prapanessis & Owens, 2002).
Regarding the second aim of this study, the results showed that eating disordered behaviors in adolescence are better predicted by the interaction between exercise (e.g., exercise frequency), individual (e.g., gender, BMI, desired ideal weight, and attraction toward exercise), and psychological variables (e.g., social physique anxiety and self-esteem). In fact, having an occasional exercise routine, being female, being overweight, desiring to weigh less, having a low attraction toward exercise, having more social physique anxiety, and having lower self-esteem all predicted the propensity for eating disordered behaviors. Prior research has also reinforced the importance of some of the predictor variables in our study, namely, the impact of social physique anxiety on abnormal eating disordered behaviors (Haase & Prapavessis, 2001) and the importance of BMI in the development of eating problems (Fairburn, Welch, Doll, Davies & O’Connor, 1997). However, our results also emphasize the importance of some variables that have received less attention in the literature (i.e., exercise frequency, attraction toward exercise, and desired ideal weight) and, most important, demonstrate that understanding adolescents’ eating disordered behavior requires analyzing exercise, individual, and psychological variables.
Some limitations of this research should be noted. The use of convenience sampling and the small number of participants in the study hinder the generalizability of the results. Moreover, the cross-sectional nature of our adopted design and our reliance on self-report questionnaires are also limitations of the study.
In conclusion, this study demonstrates that being male, having a higher attraction toward exercise, and having a lower propensity for dieting are associated with a greater likelihood of exercising regularly among adolescents. By the contrary, adolescents who exercise occasionally are more concerned about their body shape, have lower task and ego motivation to exercise, have higher social physique anxiety, and have less self-esteem. In sum, regular exercise seems to be associated with psychological well-being and with a lower propensity for eating disordered behaviors in adolescents.