


To analyze facial changes after surgically-assisted rapid palatal expansion using the analysis of Arnett and Bergman.
Material and methodsFor the Arnett analysis, before and after surgery lateral head films and profile and frontal facial photographs were obtained to compare changes in soft tissues. All data were measured with an Ormco brand protractor.
ResultsThe most significant changes were: a 7o increase in the nasolabial angle, a 4o increase in the upper lip angle, the upper lip length decreased 1mm, the upper incisor exposure increased 2mm. When performing the photographic analysis of the facial thirds and fifths, these changes were more notorious and it was observed how by modifying the lower third, the aesthetics of the entire face of the patient is affected. These changes gave the patient a younger and more aesthetic appearance.
ConclusionSurgically-assisted rapid palatal expansion allows us to observe rapid changes in the facial structures of our patients. In this case changes that improve not only function but also facial aesthetics were observed, such as closure of the nasolabial angle, an increase in the upper lip angle, a decrease in upper lip length and upper incisor exposure.
Analizar los cambios faciales posteriores a la expansión rápida quirúrgica asistida mediante el análisis de Arnett y Bergman.
Material y métodosPara el análisis de Arnett se utilizaron radiografías laterales de cráneo y fotografías extraorales de perfil y frontal antes y después de la cirugía para comparar los cambios en tejidos blandos. Todos los datos fueron medidos con un protractor marca Ormco.
ResultadosLos cambios más signifi cativos son: ángulo nasolabial aumentando 7o, ángulo del labio superior aumentó 4o, disminuyó 1mm la longitud del labio superior, aumentó 2mm la exposición del incisivo superior. Al realizar el análisis fotográfico de tercios y quintos faciales, fueron más notorios estos cambios y se observó cómo al ser modificado el tercio inferior, repercute en la estética de todo el rostro de la paciente, estas modificaciones le dieron un aspecto más juvenil y estético.
ConclusiónLa expansión del maxilar quirúrgicamente asistida nos permite ver cambios más rápidos en estructuras faciales en nuestros pacientes, en este caso se registraron cambios que mejoran no sólo la función sino también la estética facial, como el cierre del ángulo nasolabial, aumento del ángulo del labio superior, disminución de la longitud del labio superior, exposición del incisivo superior.
Surgically-assisted rapid palatal expansion (SARPE), is achieved through a series of parasagittal osteotomies on the lateral fl oor of the nose or on the medial floor of the sinus which are connected by a transverse cut. This treatment is indicated in patients who have already concluded their growth stage and who have a cross bite of more than 5 mm; skeletal constriction of the maxilla, which is characterized by a very narrow palatal vault that can be corrected by opening the mid-palatal suture. Changes in facial tissues have been reported after SARPE such as a slight retroposition of the upper lip, accompanied by an anterior alveolar remodeling, changes in upper incisor inclination, an increase of the nasal base, and fl attening and retraction of the nasal tip. These changes will depend on the degree of difficulty of the expansion process.1–11
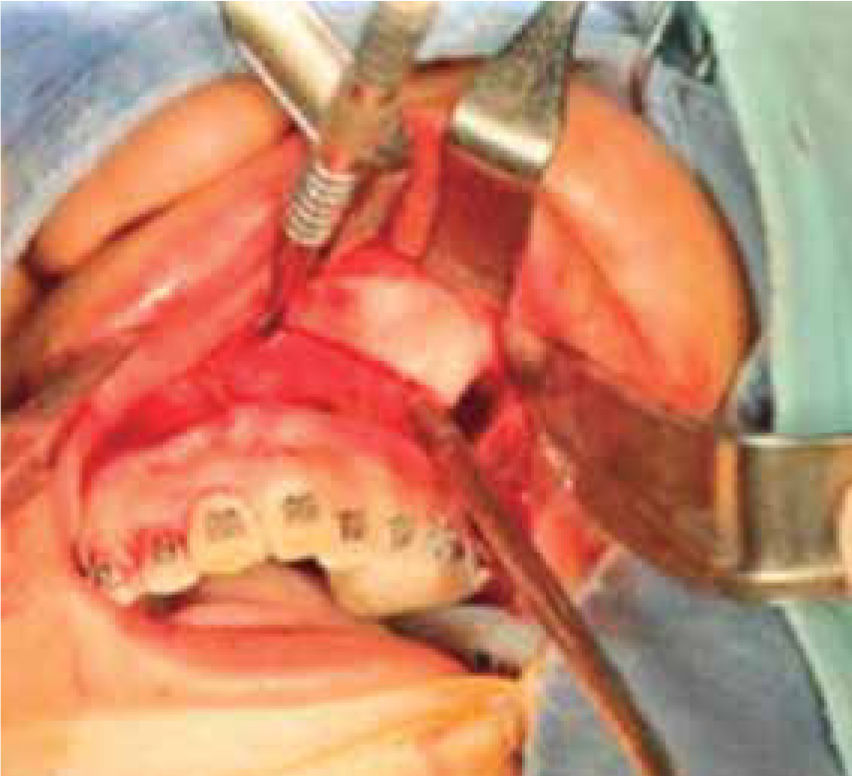
MATERIAL AND METHODSFemale patient, 16 years of age, skeletal and dental class III relationship, posterior crossbite, with a discrepancy of -2.4mm in the maxilla. A passive encapsulated hyrax-type expander was placed as well as brackets from first premolar to first premolar with a .012mm arch wire prior to the surgically assisted expansion. The patient was sedated and local anesthetic without vasoconstrictor was placed. Parasagittal osteotomies were conducted in order to release the sutures that were already ossified; once this step was completed we proceeded to the activation of the hyrax-type expander to open the maxillary and palatal sutures to confirm the success of the procedure by producing a diastema between the upper central incisors.
At the end of the surgery a diastema of 1mm was achieved. Subsequently 27 activations were prescribed thus achieving a 9.5mm expansion and a diastema of 3.3mm (Figure 1), thereby correcting the size deficit of the maxilla. The expander was removed three months after the surgical procedure and the facial changes were analyzed using the Arnett and Bergman analysis, which shows the aesthetic changes that occurred in the patient.

For the Arnett analysis lateral head films as well as facial profile and frontal photographs were obtained, before and after surgery, to compare the soft tissue changes. All data were measured with an Ormco® brand protractor.
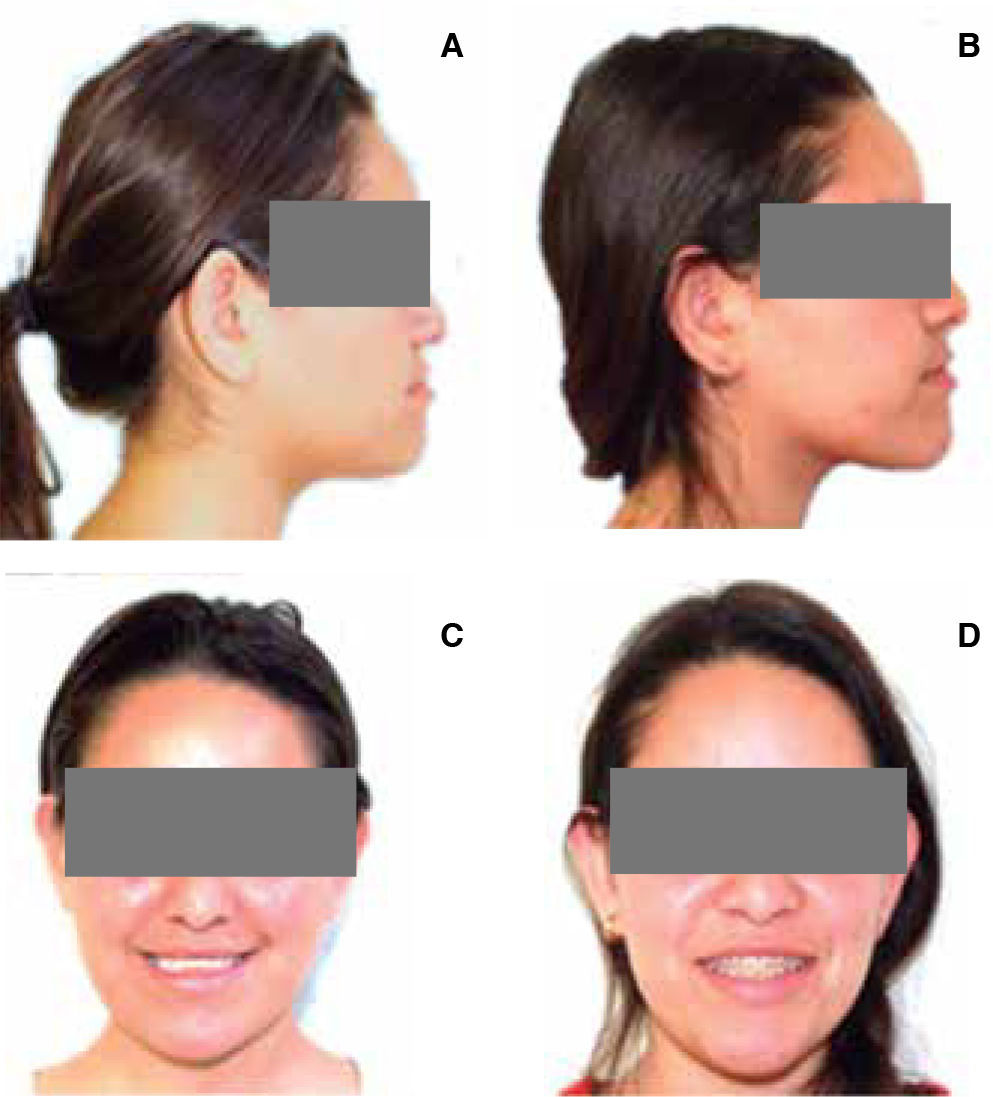
RESULTSSome of the most significant changes were: 7° increase in the nasolabial angle, the upper lip angle increased 4o, the upper lip length decreased 1mm, and the upper incisor exposure increased 2mm. The photographic analysis of the facial thirds and fifths made these changes more noticeable and revealed how when the lower third was modified, it had an impact on the aesthetics of the entire face of the patient. These modifications gave the patient a more youthful and aesthetic look (Figure 2).

A Profile photograph before the surgical expansion treatment where the upper lip collapse may be observed. B. Profile photograph after the expansion where the modification of the nasolabial angle is more noticeable due to the protrusion of the upper lip. C. Frontal photograph before treatment. The patient looks older due to the maxillary collapse and due to the poor upper incisor exposure. D. Frontal photograph after the expansion. The patient's face looks more her age, the inciso r exposure increased thus favoring the smile height.
There are several studies that illustrate the changes that occur in patients who are undergoing a process of surgically assisted rapid palatal expansion. However, few focus on the aesthetic benefits that may be observed in the patient when compared with other structures that show a more noticeable change such as the airways, in V. Pereira-Filho «Volumetric upper airway assessment in patients with transverse maxillary deficiency after surgically assisted rapid maxillary expansion»1 and the article by Xuemei Gao, Jingjing Zeng «A prospective CBCT study of upper airway changes after rapid maxillary expansion» the authors came to the conclusion that no statistically significant changes were found in regard to the increase of the oropharyngeal airspace, and explained that the changes that might be present in the airway after the expansion of the maxillary sinus depend on the existence, location, cause and severity of the nasal obstruction. The assessment of these cases was performed through the use of cone-beam images, Dolphin Imaging 3D software, and CBCT using the Ez3D2009 software.2,10
Other authors who focused their study in the SARPE postsurgical changes were Rania M et al. This article refers to three-dimensional changes that occur in the orofacial region and compares tooth-borne and bone-borne surgically assisted expansion. The changes were evaluated by CT cone beam. No statistically significant differences were found between these therapeutics however changes in soft tissues were observed, mainly a slight retrusion of the upper lip, due to the inclination of the upper central incisors hence contributing to the lip gap closure.6
E.T Daif in the article «Segment tilting associated with surgically assisted rapid maxillary expansion» tells us that the change that occurs in surgically assisted expansion is the inclination of the maxilla. According to their study most of the inclination occurs in the anterior and lower segment of the maxillary sinus,4 which results in a more protrusive, favorable projection of the anterior maxilla modifying the nasolabial angle and lip projection.9
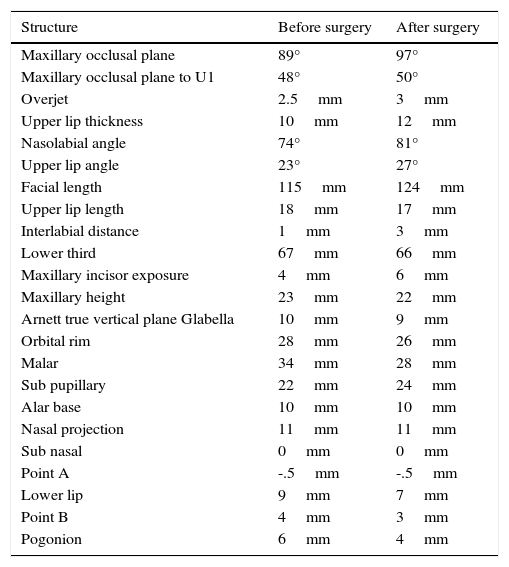
Likewise, the aim of this case report was to show the facial changes that occur in the patient after the expansion by means of a photographic and radiographic analysis following the guidelines established by Dr. G. William Arnett and described in his soft tissue analysis (Table I). As was described in previous articles one of the major changes occurs in the position of the upper lip positively affecting all the lower third. This highlights the value of lip projection, which is of great importance in the patient's facial aesthetics.
This table shows the complete Arnett analysis before and after treatment to compare the changes in the soft tissues.
| Structure | Before surgery | After surgery |
|---|---|---|
| Maxillary occlusal plane | 89° | 97° |
| Maxillary occlusal plane to U1 | 48° | 50° |
| Overjet | 2.5mm | 3mm |
| Upper lip thickness | 10mm | 12mm |
| Nasolabial angle | 74° | 81° |
| Upper lip angle | 23° | 27° |
| Facial length | 115mm | 124mm |
| Upper lip length | 18mm | 17mm |
| Interlabial distance | 1mm | 3mm |
| Lower third | 67mm | 66mm |
| Maxillary incisor exposure | 4mm | 6mm |
| Maxillary height | 23mm | 22mm |
| Arnett true vertical plane Glabella | 10mm | 9mm |
| Orbital rim | 28mm | 26mm |
| Malar | 34mm | 28mm |
| Sub pupillary | 22mm | 24mm |
| Alar base | 10mm | 10mm |
| Nasal projection | 11mm | 11mm |
| Sub nasal | 0mm | 0mm |
| Point A | -.5mm | -.5mm |
| Lower lip | 9mm | 7mm |
| Point B | 4mm | 3mm |
| Pogonion | 6mm | 4mm |
Surgically-assisted maxillary expansion allows us to see more rapid changes in the facial structures of our patients. In the case hereby presented there were changes that enhanced not only function but also facial aesthetics, such as closure of the nasolabial and the upper lip angle; reduction in the upper lip length and exposure of the upper incisor.
To Dr. Laura Isabel Carrillo Román for her invaluable support with the Arnett analysis and to EE José Carlos Ramírez López for editing this paper.
Student of the Specialty of Orthodontics and Dentomaxillofacial Orthopedics. Autonomous University of San Luis Potosí.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia