


The purpose of this study was to determine if skeletal age, dental age and chronological age agreed in 41 subjects. The orthodontist not only needs to know the patient's chronological age, but also he must know what percentage of growth can be expected in one or two years treatment time. This information is obtained by assessing the skeletal age with hand-wrist radiographs, but there are other aids of diagnosis such as the panoramic X-ray on which dental age can be assessed, so that the clinician has two aids for a more comprehensive diagnosis. Unfortunately although these methods are widely commented in Literature in the clinical practice they are not considered that much. In order to evaluate the skeletal age, we used Fishman's method in the hand-wrist radiograph and to assess dental age, Dermirjian's method in the panoramic X-ray was used. t test was used to determine the significant differences between the variables and it was applied to a test of analysis of variance (ANOVA). The results suggest exist statistically significant differences between the skeletal age and the dental age, between the dental age and the chronological age, as well as between the skeletal age and the chronological age. In correlation terms it is only observed very little correlation between the chronological age and the dental age.
El propósito de este estudio fue el de determinar si coincide la edad ósea, la edad dental y la edad cronológica en 41 sujetos. El ortodoncista no sólo necesita conocer la edad cronológica del paciente, también debe saber qué porcentaje de crecimiento puede esperar en uno o dos años que será el tiempo de tratamiento, este dato se obtiene valorando la edad ósea mediante la radiografía digitopalmar, así mismo existen otros auxiliares de diagnóstico como la ortopantomografía, a través de la cual se valora la edad dental, de tal forma que el clínico cuenta con dos auxiliares que complementan el diagnóstico, desafortunadamente aunque estos métodos son ampliamente comentados en la literatura en la práctica no se toman en cuenta. Para evaluar la edad ósea se utilizó el método de Fishman en la radiografía digitopalmar y para valorar la edad dental se utilizó el método de Dermirjian en la ortopantomografía. Se utilizó la prueba t para determinar las diferencias significativas entre las variables y se aplicó una prueba de análisis de varianza (ANOVA). Los resultados sugieren que existen diferencias estadísticamente significativas entre la edad ósea y la edad dental, entre la edad dental y la edad cronológica, así como entre la edad ósea y la edad cronológica. En términos de correlación sólo se observa muy poca correlación entre la edad cronológica y la edad dental.
During orthopedic treatment it is very important to evaluate the individual's growth since most of the patients who require treatment for their malocclusions are in a growth period. The knowledge of the maturation stage of the patient permits a proper evaluation and determines if growth has been completed. This data has influence over the diagnosis, treatment objectives and treatment plan.1
Throughout life, people go by different maturational stages that imply an increasing level of maturation. Each individual has its own rhythm or growing period of time and according to it, growth can be fast, average or late.2
The most useful method to evaluate biological maturity is the estimation of the skeletal age due to the fact that the changes that bones experience during their maturation process are very similar in all individuals and each ossification center goes through a number of morphological changes that can be easily identified.3
The hand-wrist radiograph is the most used radiograph to assess skeletal development.4 It is used conventionally to estimate skeletal age because there is a large quantity of large and rounded bones in an area that can be easily observed.5
Hand-wrist radiographs have proved to be reliable in determining the peak growth. Other methods for identifying the individuals’ maturation stage have been suggested, such as the dental age. Most frequently the dental organs are visible in the oral cavity when their roots have developed three quarters of their final surface, however, studies suggest that root formation is a more reliable maturity indicator that dental eruption.6
Material and methodsIn the present study 41 hand-wrist and 41 panoramic radiographs from 8 to 14 year- old -patients from the Orthodontics Department of the Division of Postgraduate Studies and Research of the National University of Mexico and from the Federico Gómez Children's Hospital were used.
From the files, gender information and date of birth was obtained which established the chronological age of the patient. To determine the skeletal age the Fishman method was used because it evaluates the skeletal age by calculating the Skeletal Maturity Index and determines a value of chronological age according to pre-established tables.
The radiographic analysis was carried out in a white light negatoscope by only one person as it was also the case of file selection and data collecting.
The method used for the hand-wrist evaluation was the Fishman Method and the sample was classified in one of the eleven indicators of skeletal maturity (used during adolescence) or in one of the six indicators used during childhood. Then we reviewed the tables in which the average chronological age is proposed according to the skeletal maturity and thus the value for skeletal age was ascribed.
The indicators for skeletal maturity during childhood are designated with the letters F through K and involve developmental stages of the carpian bones, phalanges and metacarpal bones. They are called Skeletal Maturity Indicator (SMI) (Figure 1).
- •
SMI F: scaphoid bone and/or trapezoid bone present.
- •
SMI G: capping of the trapezoid and trapezium bones.
- •
SMI H: in the fourth finger, the distal phalanx the epiphysis is as wide as the diaphysis.
- •
SMI I: in the fourth finger, in the distal phalanx, the epiphysis is wider than the diaphysis.
- •
SMI J: in the second finger, in the proximal phalanx, the epiphysis is as wide as the diaphysis.
- •
SMI K: in the thumb, the epiphysis is as wide as the diaphysis.

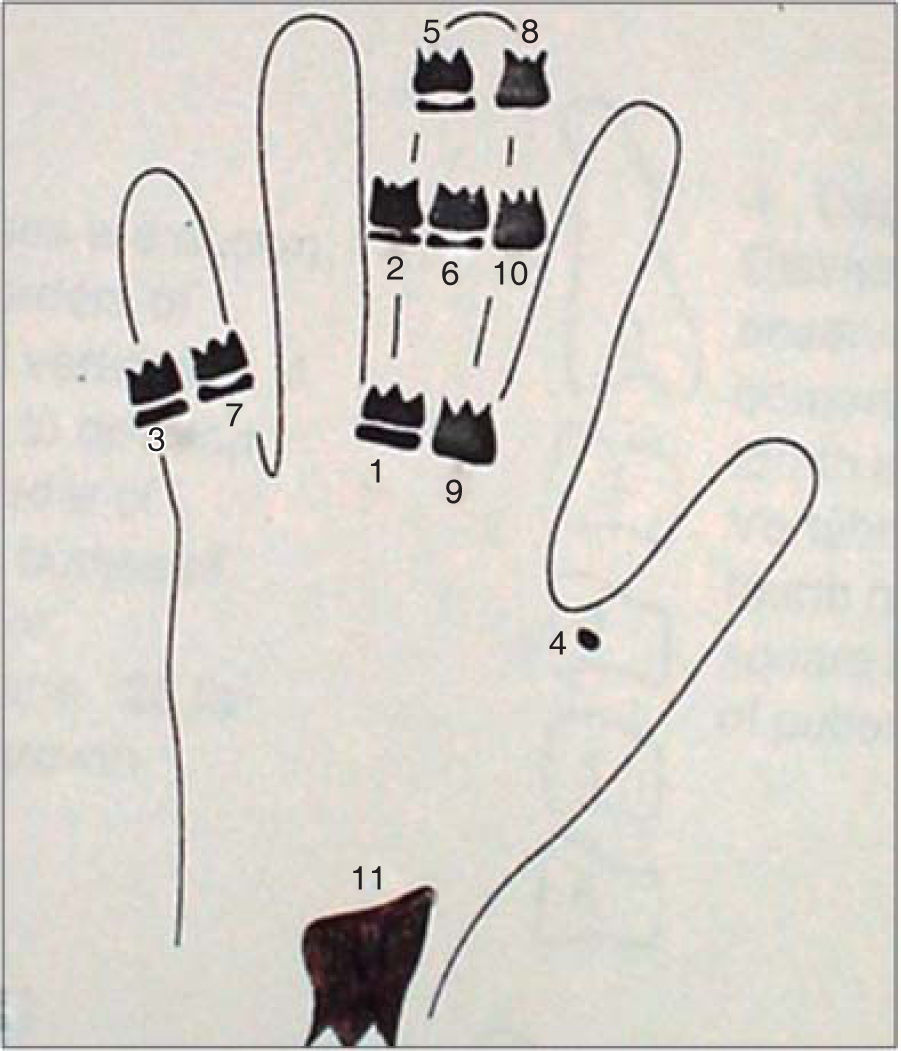
The indicators of skeletal maturity (SMI 1 to 11) of the adolescence involve developmental stages of specific phalanges, the thumb adductor sesamoid bone and the radius bone.
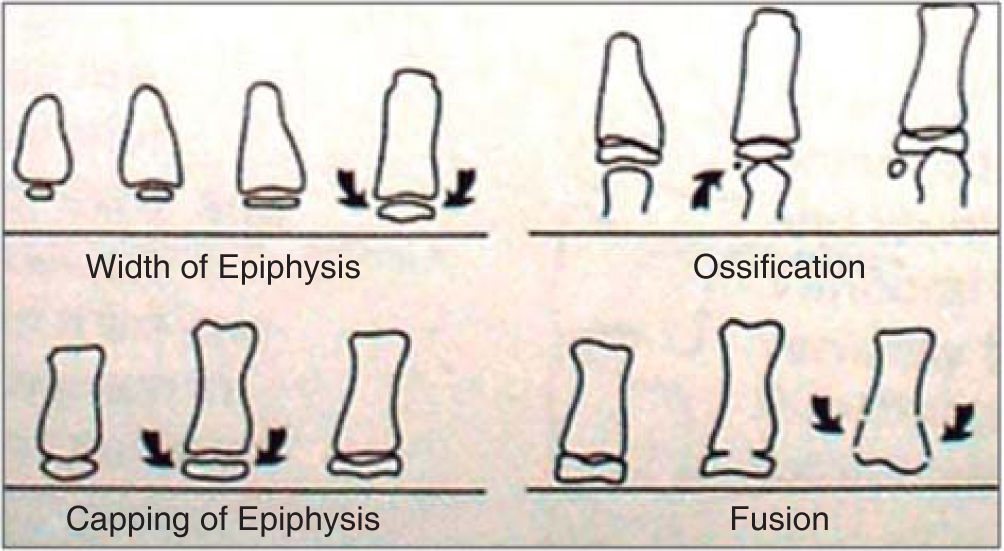
Fisherman describes four ossification stages (Figure 2):
- 1.
The width of the epiphysis is equal to the width of the diaphysis.
- 2.
The epiphysis caps the diaphysis.
- 3.
Ossification between the epiphysis and the diaphysis.
- 4.
The Skeletal Maturity Indicators (SMIs) of the adolescence are:
- -
SMI 1: Third finger, the width of the epiphysis of the proximal phalanx is equal or wider than the diaphysis.
- -
SMI 2: the mesial phalanx of the third finger is equal or wider than the diaphysis.
- -
SMI 3: fifth finger, the width of the epiphysis of the proximal phalanx is equal or wider than the diaphysis.
- -
SMI 4: ossification of the sesamoid bone of the thumb.
- -
SMI 5: fifth finger, the distal phalanx caps both sides of the epiphysis.
- -
SMI 6: third finger, the mesial phalanx caps both sides of the epiphysis.
- -
SMI 7: fifth finger, the mesial phalanx caps both sides of the epiphysis.
- -
SMI 8: third finger, the fusion of the distal phalanx is complete.
- -
SMI 9: third finger, the fusion of the proximal phalanx is complete.
- -
SMI 10: third finger, the fusion of the mesial phalanx is complete.
- -
SMI 11: the fusion of the radius is complete (skeletal growth is complete).
- -

There are six intermediate levels in the stages which are important to know in order to consider every possible treatment option.
- •
SMI 4+: SMI 4 present but just the medial side of the third finger, the distal phalanx is capped.
- •
SMI 5+: SMI 5 exists only the medial side of the third finger, the medium phalanx is capped.
- •
SMI 6+: SMI 6 is present just the medial side of the fifth finger, the medium phalanx is capped.
- •
SMI 7+: SMI 7 exists but only the mesial and central sides of the third finger, the distal phalanx is fused.
- •
SMI 10+: SMI 10 is present but just the central area of the radius is fused.
- •
SMI10++: SMI 10+ exists but just the central and distal portion of the radius bone sis fused.
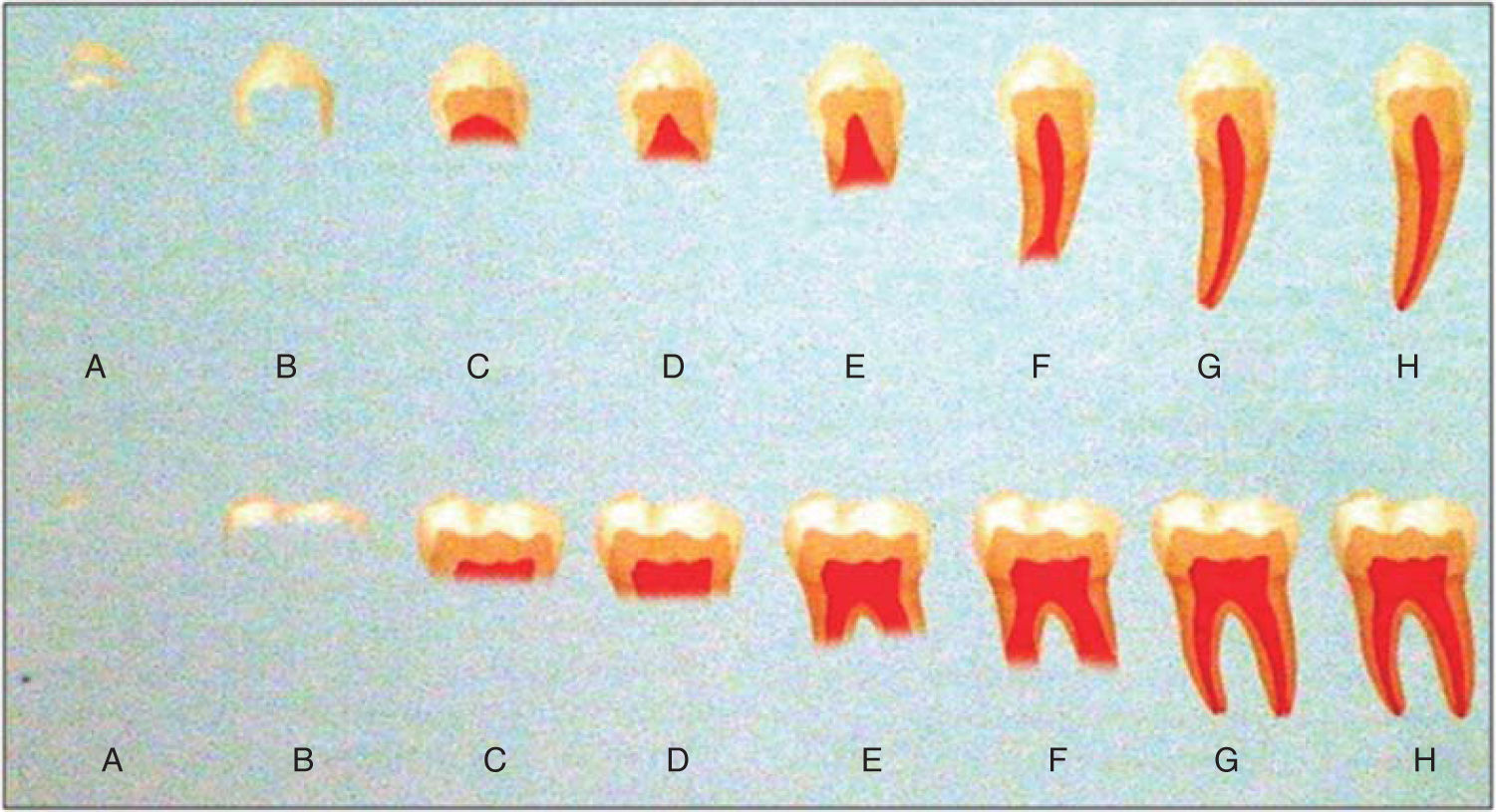
The method used to evaluate dental age was the Demirjian Procedure which is applied to primary and mixed dentitions. The method is based on a system in which a score is designated for each tooth according to its developmental stage and the sum of every score provides the maturity value for that individual (Figure 3).

The method from which the figures for each stage were derived and its justification were taken from the ones described by Tanner, Whitehouse and Haele in 1973 for skeletal age, giving each tooth a score that depends on its stage. These scores were obtained from the teeth on the lower left quadrant. In case one was missing during the assessment the one on the contralateral side was included and afterwards, added to obtain a total score for maturation which can be converted directly into dental age using a conversion table.
Boys and girls have different systems for their scores. It is reasonable to assume that the patterns for dental development do not vary greatly between different populations. The values shown for different stages might be applicable within certain limits to different populations.
The teeth were assessed in a scale from A to H according to the following specifications:
- A.
The beginning of calcification is observed in the form of an inverted cone on the upper portion of the crypt without fusion of the calcification points.
- B.
Fusion of the calcification points taking one or more cusps.
- C.
The enamel formation is completed on the occlusal surface, dentin increments are observed.
- D.
The crown is completed until the enamel-cement junction.
- a.
The upper border of the pulp chamber of unirradicular teeth has a more defined curve form, concave towards cervical with the projection of the pulp horns taking an umbrellalike shape. In the molars, the pulp chamber has a trapezoid form.
- b.
The beginning of the root formation can be observed and it has the shape of a spicula.
- a.
- E.
On teeth with one root the pulp chamber walls form straight lines interrupted by the pulp horn that looks bigger than in the previous stage.
- a.
The root length is shorter than the crown height.
- b.
In molars, the furcation has a half-moon shape.
- c.
The root length is shorter than the crown length.
- a.
- F.
The walls of the pulp chamber form a triangle.
- G.
The root canal walls are parallel and the apex is partially open.
- a.
Closure of the apical foramen.
- b.
The periodontal membrane has a uniform width around the root and apex.
- a.
The calibration of the researcher was appointed to a Dental Surgeon specialized in the area of growth and development. The intra and interobserver correspondence was 95% (kappa).
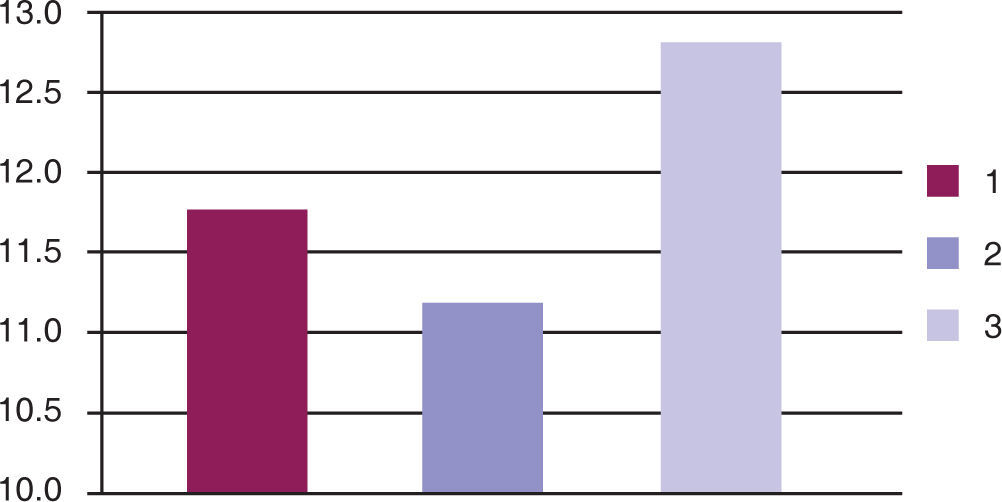
ResultsFrom the total sample, 56% were male (n=23) and 44% were female (n=18). When comparing the obtained measurements with the ANOVA analysis the results show that there are statistically significant differences between dental and chronological age (p < 0.05). Likewise statistically significant differences were found between the skeletal and chronological age (p < 0.05) (Figure 4).

Now, when seeking to find statistically significant differences between the three study variables the results again showed statistically significant differences (p < 0.05).
In terms of correlation it was observed that between dental age and skeletal age there is no correlation (r2=0.18), between chronological and skeletal age there is no correlation (r2=0.37) not so between chronological and dental age where very little correlation was determined (r2=0.63).
DiscussionThe results of the present study agree with Dermirjan and Buschang4 who found that the interrelation between skeletal and somatic maturity is consistent but that the association with dental maturity is very low or nonexistent.
On the other hand, Engstrom and Sagne4 found a positive correlation between dental and skeletal development.
Kanbur et al7 did not find any differences between dental and skeletal age in healthy individuals, in other words, there were no statistically significant differences between both. In their study they mention that healthy teenagers have a dental maturity according to their chronological age but not to their skeletal age.
Sierra and Vallejo8 did find significant differences between chronological and dental age using different study methods.
Demisch and Wartmann9 reported a high correlation between dental and skeletal age. Chertkow, Coutinho and Krailassiri report similar results.
Lewis, Garn and Tanner10 found a low or insignificant correlation between dental and skeletal development.
Other authors like Steel, Patterson and Garn4 have reported low correlation between skeletal and dental development, and concluded that the systems are independent of each other.
The inconsistency in the results is caused by the different methods and procedures used for data recollection.
ConclusionsStatistically significant differences (p < 0.05) were found between dental, chronological and skeletal age in the studied sample.
No correlation was found between dental and skeletal age, likewise between the chronological and the skeletal age no correlation was found. However, between dental and chronological age very little correlation was found.
According to the results obtained by this and other investigations it can be established that due to differences between dental, skeletal and chronological ages, it is necessary to take under consideration the three studied variables when performing a patient's diagnosis. Nevertheless we recommend that the most useful method for estimating a person's biological maturity is the skeletal age since it reliably represents the physical development of an individual.
It would be very useful to continue similar studies increasing the sample size and using different study methods in order to obtain more solid evidence and make stronger recommendations.