






To determine the true position of the mandible is one of the most important aspects of orthodontic-surgical diagnosis. It provides information about the skeletal discrepancy between the maxilla and mandible even in patients with conditions other than a normal pattern of mandibular stability. In patients with hemifacial microsomia it is difficult to determine the true position of the mandible, since due to their condition, they present structural alterations that hinder record taking. The purpose of this study was to assess two techniques for recording mandibular position (power centric technique and the gothic arch technique) to determine the most effective method to provide greater accuracy in the record taking process. Eight patients with hemifacial microsomia, ages between 13 and 17, four female (50%) and four male (50%) were assessed. A total of 16 semi-adjustable articulator mountings were conducted using both techniques. Changes in the overjet, vertical discrepancy and between dental midlines were monitored. The results showed that there were significant sagittal, vertical and transverse differences with the gothic arch technique.
Determinar la verdadera posición mandibular es uno de los aspectos más importantes para el diagnóstico ortodóncico-quirúrgico, el cual nos proporcionará la discrepancia esquelética entre el maxilar y la mandíbula, más aún en pacientes que presenten condiciones diferentes a un patrón normal de estabilidad mandibular. En los pacientes que presentan microsomias hemifaciales es difícil determinar su verdadera posición mandibular, ya que por la misma condición presentan alteraciones estructurales que dificultan la toma de registros. El propósito del estudio fue evaluar dos técnicas para el registro de la posición mandibular (técnica céntrica de poder y técnica del arco gótico) con objeto de determinar el método más eficaz para brindar mayor veracidad en el registro, dado que, en nuestra institución se han experimentado algunas inconsistencias durante la obtención de registros en pacientes con malformaciones o discrepancias esqueléticas considerables. Se evaluaron ocho pacientes con microsomia hemifacial de entre 13 y 17 años de edad, cuatro del sexo femenino (50%) y cuatro del sexo masculino (50%). Se realizaron 16 montajes en un articulador semiajustable utilizando ambas técnicas, se monitorearon los cambios en la sobremordida horizontal, vertical y discrepancia entre las líneas medias dentales. Los resultados mostraron que hubo diferencias significativas sagitales, verticales y transversales con la técnica del arco gótico.
To determine true mandibular position is one of the most important aspects for the surgical orthodontic diagnosis of a patient. It will help in determining the skeletal discrepancy between the maxilla and mandible, even more in patients with conditions different to a normal pattern of mandibular stability. In patients who have hemifacial microsomia it is difficult to determine mandibular position, since by their same condition, they have structural alterations that hinder record taking. Currently, a variety of clinical techniques are used to obtain mandibular records in centric relation (CR). All of them involve some type of mandibular manipulation, followed by the placement of a registration material (wax) that reproduces cusp indentations with which the models are mounted. One of the most frequently used techniques is the one- hand rearward pressure. There are others referred by Woelfel such as the neuromuscular guided RC (Lucia jig and the Leaf Gauge by Long).1
The method that Roth suggests is the power or force centric that uses two segments of wax and results from mandibular manipulation and an anterior stop for the CR record.2,3 Other method is the record of the Gothic Arc tracing, considered as a starting point from which protrusive and lateral mandibular movements begin in patients. The vertex is the point of reference designated as CR. In this technique there is no manual mandibular manipulation.4,5
Background on centric relation recordsIn 1756 Phillip Ptaff6 was the first to describe his technique for bite registration called «taking bite». Since the end of the nineteenth century it was the most commonly method used however, several clinical trials have developed other techniques for centric relation records. In 1955 Shanahan7 described the technique «swallowing or free closure», which was based on the fact that swallowing saliva was the determining factor for the vertical dimension and centric relation. Other researchers used the technique described by Mc-Collum8 called «chin- point guidance» which retrudes the prognathic jaw and emphasize the importance of the axial axis in the records of centric relation. Dawson9 recommended the technique of «bilateral handling», which emphasized the importance of guiding the mandible upwards by positioning the operator's fingers in the goniac angles while the thumbs apply pressure to the chin to facilitate condylar settlement in centric relation. Another technique known as «Myo-monitor» is based on stimulated muscle contractions to register centric relation.10
Lucia11 in 1964 suggested the use of an anterior jig designed to minimally separate the maxillary and mandibular teeth, and to break the proprioceptive pattern resulting from dental contact thus allowing the muscles to seat the condyle. Lundeen12 and Wood13 reported that a strong muscle contraction performed by a patient with an anterior rigid stop seats the condyle into the uppermost position compared to other techniques. Williamson14 advocated the use of calibrated sheets with the same purpose: an anterior upper settlement of the condyle by action of the upper head of the lateral pterygoid muscle and the temporalis muscle without the influence of dental contact. Roth designed a technique called centric that uses two segments of blue wax DelarMR (Dollar Co, Lake Oswego) for bite registration. This technique allows the patient's muscles to seat the condyles without the influence of the dental contact.15
The first graphic record was based on the studies of mandibular movements by Balkwill in 1866.16 The arch intersection produced by the left and right condyle forms a vertex known as the Gothic arch tracing.
The first «tracing vertex» was reported by Hesse in 1897, and the technique was imposed and popularized by Gysi around 1910.17 The plotter designed by Gysi was an extraoral plotter. The tracing plates, coated with wax, were attached to the mandibular arch.
An incisal guide pin was mounted in the maxillary arch. When successful record was taken, the patient kept the plates centered on the apex of the tracing sustained by a niche so that they were recorded and fixed.18 In 1927 Hanau19 recognized that the Gysi tracing is effective for recordings, but its universal use is not good. On the other hand, Tench20 established that the Gysi tracing technique should be the only method to perform the centric relation records; and that all other methods were «deception and games». Gysi concluded that his tracing technique only has five degrees of error, while the records obtained with bite wax displayed up to about 25 degrees of error.21
Hemifacial microsomia (ocular-auricular-vertebral syndrome, Goldenhar)Hemifacial microsomia is the most common form of facial asymmetries. It affects about one in every 5,000 births and occupies the second place of the most common facial deformities.22,23
In 1960 hemifacial microsomia was defined as a condition that affects the development of the primary ear, mouth, and mandible. The disease varies from mild to severe, and the anomaly is just on one side in many cases, but bilateral involvement is also known to occur, with a more severe expression on one side. The Goldenhar syndrome is considered a variation of this condition, characterized by vertebral anomalies and epibulbar dermoids. The condition is known for being extremely complex and heterogeneous.
Although there is no consensus upon a minimum of diagnostic criteria, the characteristic facial phenotype is sufficient when the manifestations are present. In some instances, pre-auricular anomalies and isolated microtia, might represent the slightest demonstration of the condition. Unilateral microtia or an abnormality of the ear, including the pre-auricular tags, has been suggested as a mandatory feature for some authors. The disease is not only limited to facial structures, other abnormalities, such as cardiac, renal, and skeletal might exist.
The group of anomalies suggests that its origin is approximately at 30-45 days of pregnancy. This has been confirmed in humans by evidence of the disruption test of blood supply. The alteration of chondrogenesis has also been exposed as a theory.
Anomalies in the first and second branchial arch frequently combined with facial paralysis have been observed in children born from pregnant women exposed to thalidomide, primidone, and retinoic acid.
Materials and methodsThe present study was assessed and approved by the Department of Education and Academic Development of HIMFG. Informed consent was obtained in accordance with the requirements stipulated by the HIMFG. All patients with hemifacial microsomia between the ages of 13 and 17 years sent by the external patient service for orthodontic treatment were included. Patients with any pathologic change in the mandible that alters the position of the same (tumors, fracture, cysts), patients with early mixed dentition and patients with dental agenesis in the posterior or anterior segment of the arches that would interfere with the records, were excluded. All the patients who abandoned the study and those who were subjected to restorative treatment during the taking of records were excluded.
All procedures were carried out by a single operator previously calibrated to decrease the degree of error. During the course of the procedure the articulator, face-bow, mounting pin, bite tabsMR and mounting table of the PanadentMR system were used.
For each patient, three sets of alginate impressions were taken. They were immediately disinfected with hypochlorite sodium and flushed. Then, cast models were obtained carefully with plaster type IV (Scottish Rock- WhipMixCorp). The surplus and bubbles present in the models were removed in order to eliminate interference.
Upper model mountingThe splitcast technique was used for the upper model mounting by placing plaster-cast separator between the surfaces when joining them. This procedure had the purpose of rectifying the correct mounting of the lower model with the power centric technique. To mount the upper model, the records obtained through each patient's face-bow were transferred to the articulator.
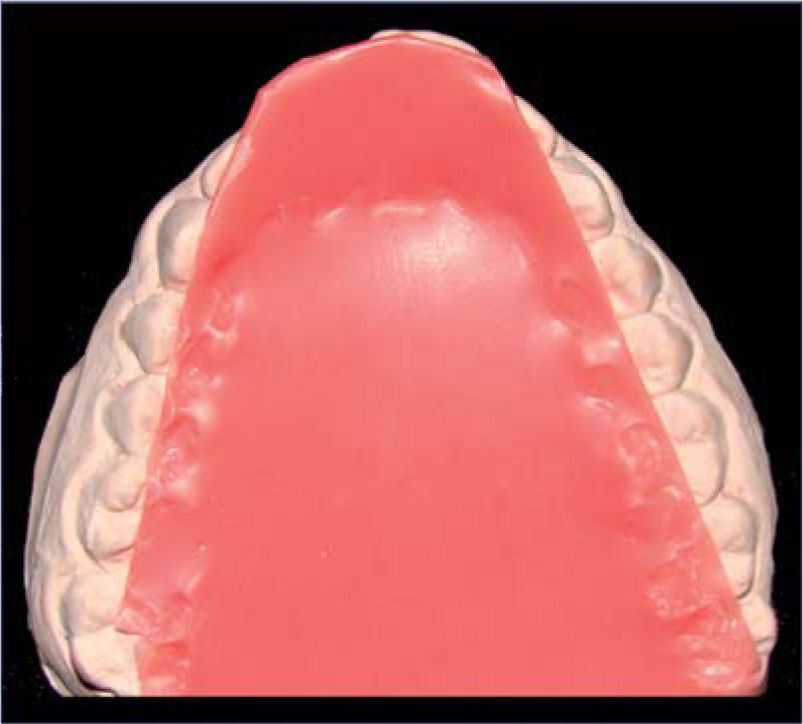
MIC recordThe record of maximum intercuspation was conducted with MoycoMR extra hard pink wax, a sheet of wax was taken and warmed up to 53 oC in order to bend it and thus obtain a sheet with two thicknesses of wax. Then the wax was pre-adjusted to the models to obtain a more accurate record and to make it more comfortable for the patient. The wax was warmed up again and introduced carefully into the patient's mouth asking him or her to close strongly in their usual closing position, until the occlusal portion of the antagonist teeth made contact. Before the wax hardened, the lateral and posterior surplus was cut. The wax was placed in the mouth again and it was verified that closure with and without wax was the same (Figure 1).

Once the MIC record was obtained, a cotton roll was placed between the patient's incisors for five minutes before beginning the procedure for both record-taking techniques.
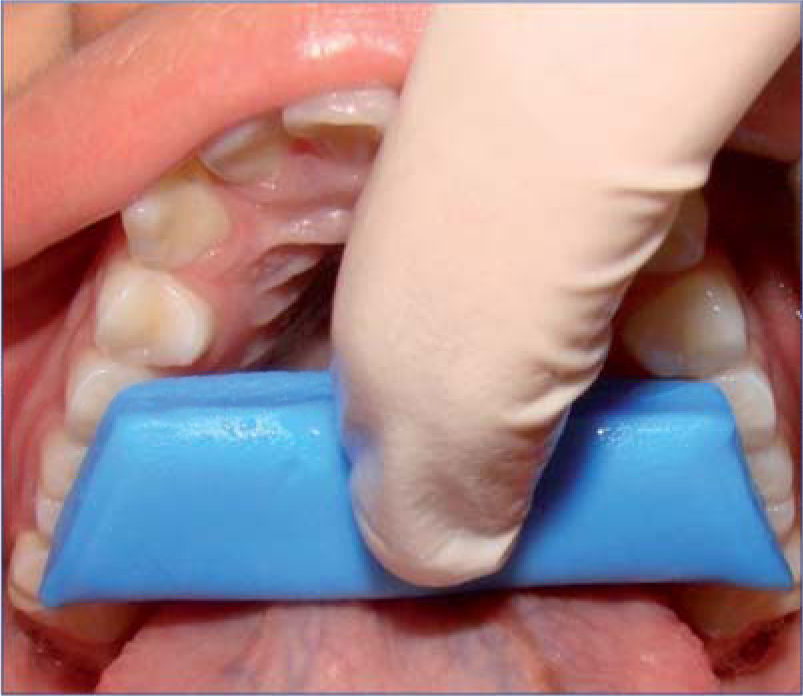
CR record: power centric techniqueTwo segments of DelarMR blue wax for bite registration were used for each patient. The anterior segment was built with a three-wax-sheet thickness and covered the distal portion of upper right lateral incisor up to the distal portion of the lateral incisor on the opposite side. The palatal extension varied depending on the patient's overjet. The posterior segment was constructed with two thicknesses of wax. This segment included the space between right second premolar and first molar to the contralateral second premolar and first molar. Then the patient was reclined on the dental chair to a 45o angle with respect to the floor.
The wax was warmed to 53 oC and then was placed in the patient's mouth. Once the anterior segment of wax was in place, the clinician guided the mandible to centric relation, settling the condyles upwards and guiding the pogonion down. Immediately the patient was instructed to close the jaw until the posterior teeth had a 2 mm dysocclusion. Before removing the anterior segment, it was cooled with compressed air and after removal it was placed in water and ice to prevent deformational changes (Figure 2).

Afterwards, the posterior segment was heated at a 53 oC temperature and placed on the upper teeth. With the posterior segment in position, the anterior segment was positioned again in the upper arch. The patient was guided in the same way towards mandibular closure until contact of the lower incisors was settled within the anterior block. The cooling procedure of the materials was repeated before and after removing them from the mouth (Figure 3).

Once the record was obtained, the waxes were adjusted to eliminate interferences and the mounting of the lower model was performed using the Split-cast as a proceedings correction method.
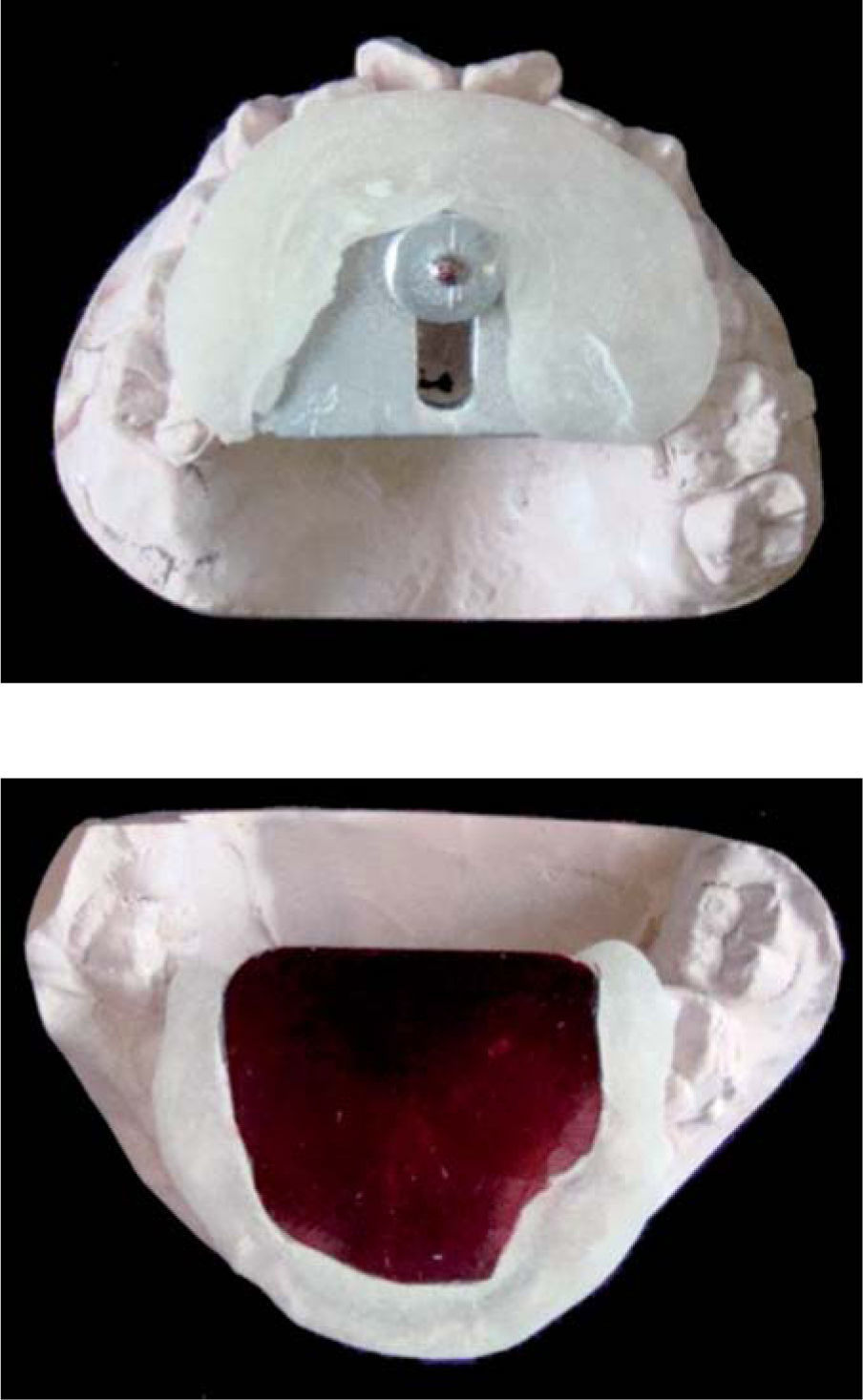
CR record: Gothic arch tracing techniqueFor the recording of centric relation with the Gothic arch tracing technique, plates of the commercial house DentsplyMR, were used and individually adapted for each patient using a set of plaster models mounted on a hinge articulator in maximum intercuspation. Nic-toneMR autocuring transparent acrylic was used for their individualization. Before placing the lower plate in the patient's mouth it was inked with a red permanent marker, since, on this surface the tracing of the mandibular movements were drawn (Figure 4).

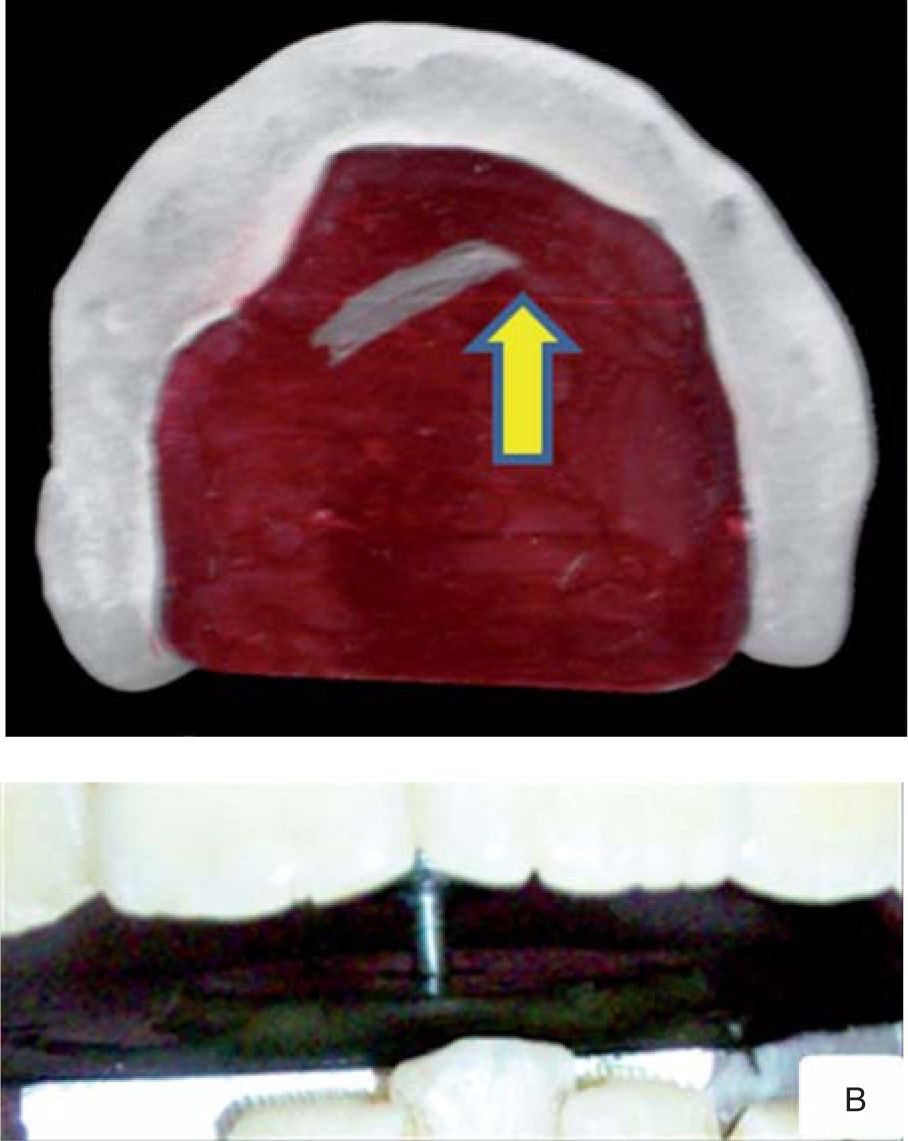
The patient was placed in a 90-degree position from the floor and the upper plate with the marker rod was inserted in the mouth. Next, the bottom plate was placed in the lower dental arch and the patient was given the instruction to occlude until the upper rod made contact with the bottom plate. The patient was told to perform protrusion and lateral movements for two minutes without separating the plates, carefully monitoring that there were no contacts or interferences during record taking, thus ensuring that the contact occurred only between the rod and the lower plate (Figure 5).

Once the tracing was obtained, the lower plate was removed and the centric lock was placed. The centric lock is a device that contains a perforation which was placed and fixed with wax just above the apex of the Gothic arch tracing, better known as centric relation (Figure 6).
.")
Once the position of the lower plate was verified, it was placed again inside the patient's mouth and it was sought that the rod would fall into the hole of the centric relation lock. In this position white mounting plaster was injected laterally in order to obtain the guides for the mounting of the lower model. After 4 minutes, once the positives of the plaster cast have been obtained, the plates and Gothic arch tracing guides were removed for adjustment.
The mounting of the lower model was carried out through the use of the plates along with the obtained plaster guides, which secured greater precision at the time of the procedure (Figure 7).

Once the records were completed and the mountings were made, we proceeded to the measurement of the occlusal findings by means of a digital caliper and the sagittal, transverse and vertical distractions were measured.
Statistical analysisProportion comparison was performed using the Wilcoxon test for ranks for the qualitative variables as well as median proof for comparison of the same. p < 0.05 was considered statistically significant.
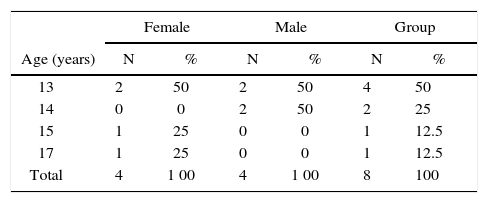
ResultsA total of 16 model mountings were performed for eight patients with hemifacial microsomia; four of them were female (50%) and four were males (50%), with a median age of 13 years. The relationship with regard to the distribution by age and gender are shown in table I.
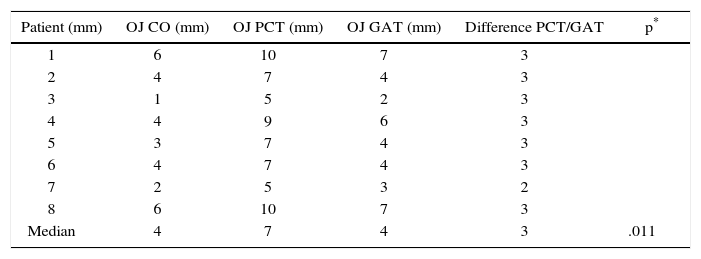
With regard to the overjet (OJ) a median in centric occlusion (CO) of 4 mm was found, with a maximum of 6 mm and a minimum of 1 mm. With the power centric technique (PCT) a median of 7 mm with a maximum of 10 mm and a minimum of 5 mm was determined. The Gothic arc tracing technique (GAT) showed a median of 4 mm with a maximum of 7 mm and a minimum of 2 mm. The distribution is shown in table II.
Overjet (OJ) comparison in centric relation with the power centric technique and the gothic arch tracing technique in 8 patients with hemifacial microsomia.
| Patient (mm) | OJ CO (mm) | OJ PCT (mm) | OJ GAT (mm) | Difference PCT/GAT | p* |
|---|---|---|---|---|---|
| 1 | 6 | 10 | 7 | 3 | |
| 2 | 4 | 7 | 4 | 3 | |
| 3 | 1 | 5 | 2 | 3 | |
| 4 | 4 | 9 | 6 | 3 | |
| 5 | 3 | 7 | 4 | 3 | |
| 6 | 4 | 7 | 4 | 3 | |
| 7 | 2 | 5 | 3 | 2 | |
| 8 | 6 | 10 | 7 | 3 | |
| Median | 4 | 7 | 4 | 3 | .011 |
OJ CO = Overjet in centric occlusion, OJ PCT = Overjet, power centric technique, OJ GAT = Overjet, gothic arc tracing technique mm = milimeters
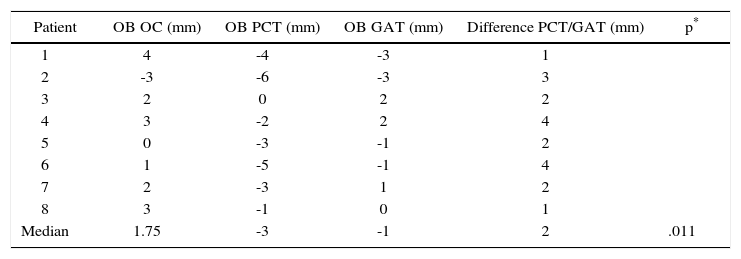
With regard to the overbite (OB), a median in centric occlusion of 1.75 mm was found, with a maximum of 4 mm and a minimum of 0 mm. With the power centric technique, a median of -3 mm with a maximum of -6 mm and a minimum of 0 mm was determined. The Gothic arc tracing technique had a median of -1 mm with a maximum of -3 mm and a minimum of 0 mm. The distribution is shown in table III.
Overbite (OB) comparison in centric relation with the power centric technique and the gothic arc tracing technique in 8 patients with hemifacial microsomia.
| Patient | OB OC (mm) | OB PCT (mm) | OB GAT (mm) | Difference PCT/GAT (mm) | p* |
|---|---|---|---|---|---|
| 1 | 4 | -4 | -3 | 1 | |
| 2 | -3 | -6 | -3 | 3 | |
| 3 | 2 | 0 | 2 | 2 | |
| 4 | 3 | -2 | 2 | 4 | |
| 5 | 0 | -3 | -1 | 2 | |
| 6 | 1 | -5 | -1 | 4 | |
| 7 | 2 | -3 | 1 | 2 | |
| 8 | 3 | -1 | 0 | 1 | |
| Median | 1.75 | -3 | -1 | 2 | .011 |
OB CO = Overbite in centric occlusion OB PCT = Overbite, power centric technique OB GAT = Overbite, gothic arc tracing technique mm = millimeters
Regarding the discrepancy between midlines we found a median in centric occlusion of 2 mm with a maximum of 3 mm and a minimum of 0 mm. With the power centric technique the median was 5 mm, with a maximum of 6 mm and a minimum of 4mm, the gothic arc technique showed a median of 3 mm, with a maximum of 4 mm and a minimum of 1 mm. The distribution is shown in table IV.
Comparison of the discrepancy between midlines found in centric occlusion with the power centric technique and the gothic arc technique in patients with hemifacial microsomia.
| Patient | MLD CO (mm) | MLD PCT (mm) | MLD GAT (mm) | Difference PCT/GAT (mm) | p* |
|---|---|---|---|---|---|
| 1 | 2 | 5 | 3 | 2 | |
| 2 | 3 | 6 | 4 | 2 | |
| 3 | 1 | 4 | 1 | 3 | |
| 4 | 0 | 4 | 3 | 1 | |
| 5 | 0 | 5 | 2 | 3 | |
| 6 | 3 | 6 | 4 | 2 | |
| 7 | 2 | 5 | 3 | 2 | |
| 8 | 2 | 6 | 3 | 2 | |
| Median | 2 | 5 | 3 | 2 | .011 |
MLD CO = Midline discrepancy in centric occlusion, MLD PCT = Midline discrepancy, power centric technique, MLD GAT = Midline discrepancy, Gothic arc tracing technique mm = millimeters Direct source 2012.
The topic of centric relation records and the true mandibular position is very controversial. However, the pursuit of excellence and distinction as health professionals must lead us to improve the quality of our records to establish a diagnosis and treatment plan that provide better results.
In the present study the observed discrepancies between the compared techniques were the downwards and posterior condylar distraction which are the most frequent as mentioned by Wood, Crawford and Roth. Crawford described as a clinical problem a horizontal or vertical discrepancy of 1 mm and of 0.5 mm in the transverse plane. Utty et al. stated that this problem is found in horizontal and vertical discrepancies beginning at 2.0 mm and transverse at 0.5 mm. Klary et al conducted a study in 200 patients and found that the most frequent kind of distraction is downwards and posterior.
In our study the power centric technique (PCT) showed a trend toward a larger displacement in the horizontal plane (7 mm) than the Gothic arch technique (GAT) (4 mm). In the vertical plane, it was a -3 mm displacement with the power centric technique and a -1 mm displacement with the Gothic arc technique, indicating a lower displacement. Therefore, it was concluded that the most frequent condylar displacement pattern was more present in both directions with the power centric technique. This is consistent with the results published by the authors mentioned above perhaps due to the deprogramming that was performed during record taking.
Schmitt mentioned that the power centric technique is highly reproducible, however, in our population it has been noticed that severe malocclusions do not allow a proper handling of the materials during record taking specially in class II or class III patients with an OJ larger than 6 mm (positive or negative).
The control of the record taking process with GAT is more accurate because the materials do not distort, it does not require the patient's cooperation or the clinician's dexterity - experience.
ConclusionsThe findings of this study suggest that the Gothic arch is a more stable technique than the power centric technique due to the fact that the materials used to mount to in CR are not thermoplastic and do not require experienced handling from the operator or the patient's cooperation. Additionally, during record taking the Gothic arc technique offers a degree of dysocclusion and muscle fatigue that relaxes the patient's muscles thus moving closer to centric relation.
The Gothic arch technique is highly reproducible. Although it requires more laboratory time, it reduces chair-time and is more cost-effective. This study was developed with the purpose of changing our centric relation record taking technique since we had inconsistencies in the records, especially in a population with asymmetries and skeletal deformities which make it difficult to obtain reliable centric relation records.
The authors suggest performing prospective studies with a larger sample size in order to verify the findings of the present study.