













Male pacient, 17 years 2 months of age, with a slight facial assimetry and convex profile. He was a hyperdivergent skeletal class II with bilateral molar class I, bilateral cuspid class II, mild crowding on the upper and lower arches, OD 31 with a bucal possition, increased overbite, and normal over jet. It was determined as a treatment plan: the use of MBT technique slot 0.022, extraction of the first maxillary bicuspids and one mandibular incisor as an alternative for dental compensation due to the degree of crowding. Functional bilateral molar class II and a bilateral canine class I was obtained as well as anormal overbite and overjet, incisor guidance and harmonic smile.
Se presenta a un paciente masculino de 17 años dos meses de edad, con ligera asimetría facial y perfil convexo, presenta clase ósea II, patrón hiperdivergente, clase l molar bilateral, clase ll canina bilateral, apiñamiento leve en arcada superior e inferior, OD 31 vestibularizado, sobremordida horizontal aumentado y sobremordida vertical dentro de la norma. Se determinó como plan de tratamiento el uso de brackets MBT slot 0.022” con la extracción de primeros premolares superiores y de un incisivo central inferior como plan de tratamiento compensatorio debido al grado de apiñamiento que presentaba obteniendo clase molar II funcional y canina I bilateral, sobre mordida horizontal y sobre mordida vertical adecuados, guía incisiva, desoclusiones en lateralidades y una sonrisa armónica.
During orthodontic treatment, Nanda mentions that the removal of a lower incisor is one of the alternatives in cases of overcrowding in the mandibular arch.1 The removal of mandibular incisors is an appropriate therapy in certain types of carefully selected malocclusions. It is especially suitable for patients with skeletal class I and mild skeletal class III malocclusions with a slight tendency to open bite.2 According to Zachrisson, the removal of a lateral incisor is generally preferred because it is less noticeable aesthetically, but the incisor that is farther outside of the natural arch and closest to the crowding is usually the best candidate to be extracted.3
It is important to mention that, when teeth are aligned to correct the crowding, it is necessary to check that there is enough space in the arch by performing the necessary measurements in order to determine which incisor to remove thus achieving an optimal occlusion that will provide function, stability and aesthetics.4 The removal of a lower incisor has many advantages with respect to premolar extractions: first, it reduces treatment time (especially if the crowding occurs in the anterior region); second a more stable treatment is expected in the anterior region because intercanine width is not altered significantly. Finally, since it requires minimal retraction unlike cases of premolar extractions, the anteroposterior position of the mandibular incisors does not change significantly so a harmonic profile may be maintained. Extraction of a lower incisor has some disadvantages, for example: if there is a Bolton discrepancy lower space closure will result in an overjet increase.5
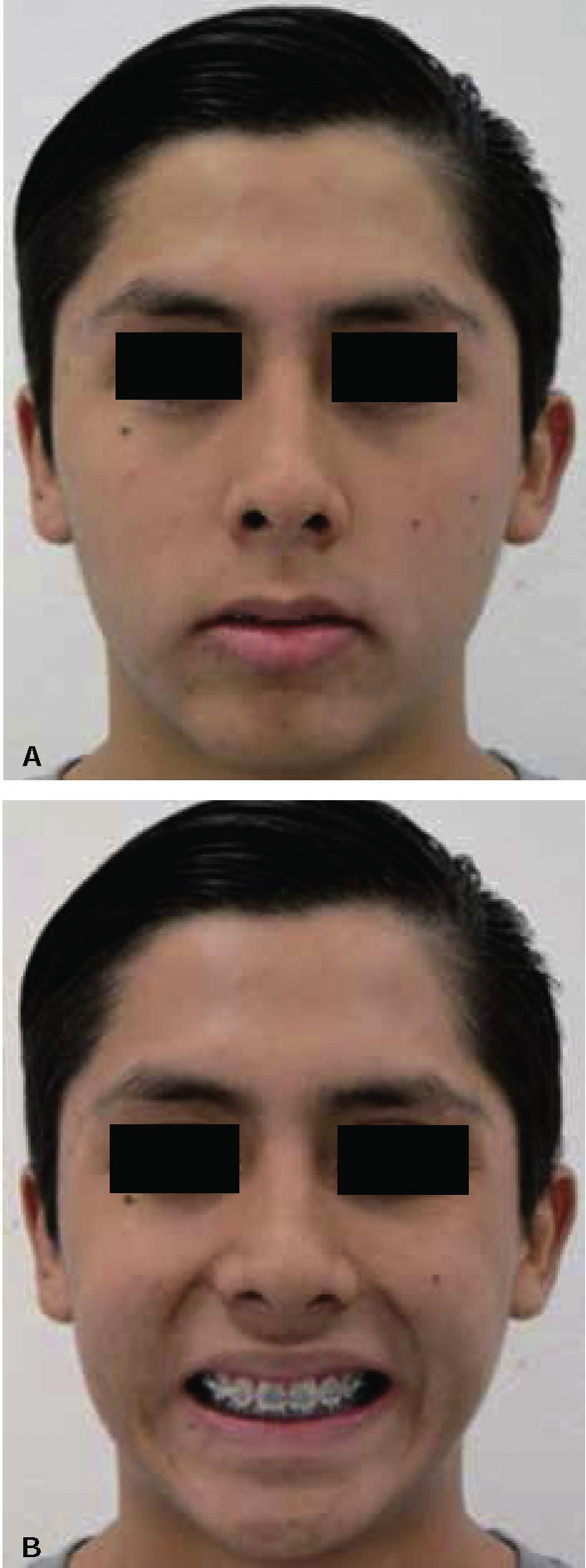
CASE REPORTMale patient, 17 years 02 months of age, who referred as reason for consultation «I want to fix my teeth because they are crooked». Extraoral frontal and smile photographs were obtained as well as a profile photographs. An oval facial contour and good facial thirds relationship was observed (Figure 1). Upon smile analysis, he showed the totality of the clinical crowns, reduced buccal corridors and mild crowding in the upper arch (Figure 2). He had a convex profile, increased nasolabial angle, normal interlabial distance as well as incisal edge-stomion relationship, upper lip retrusion and a slight soft chin retrusion (Figure 3).
INITIAL RADIOGRAPHIC STUDIES


In the lateral headfilm (Figure 4), a skeletal class II, vertical growth, upper incisors within normal values and lower incisor proclination may be noted.

In the initial panoramic radiograph short condyles, short mandibular ramus without asymmetries or apparent pathologies, complete dentition and impacted third molars may be observed (Figure 5).

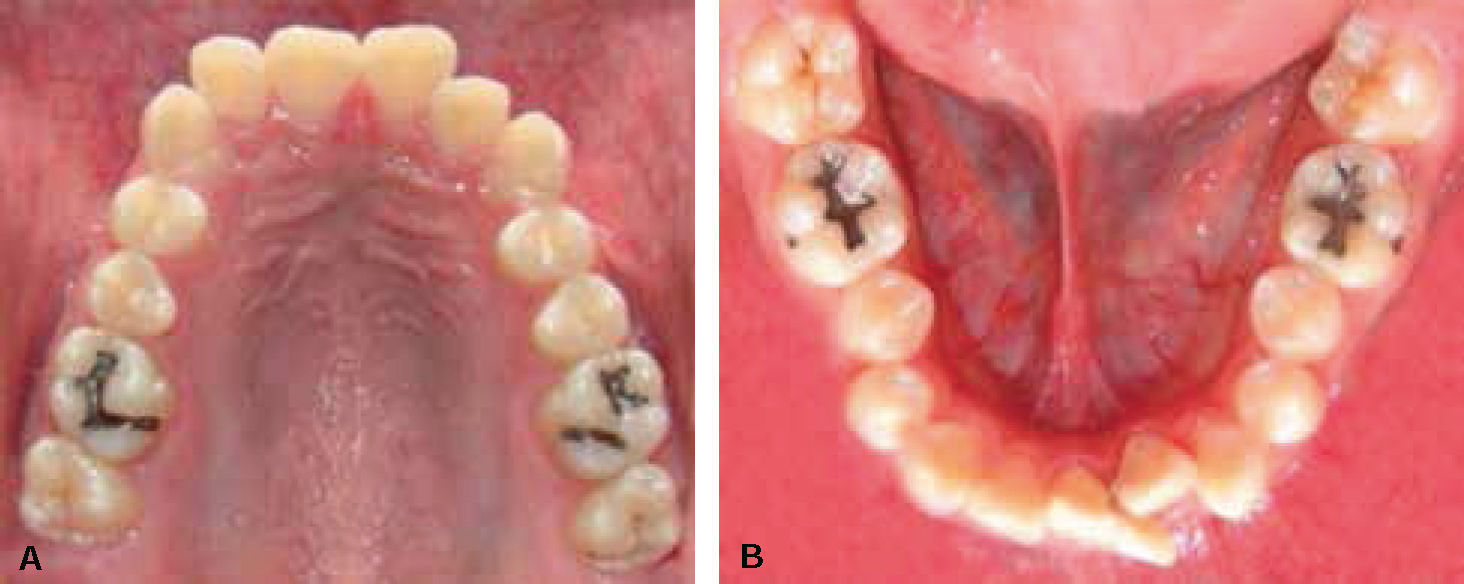
In the initial intraoral photographs, a bilateral molar class I, canine class II, mild upper and lower crowding, labially positioned lower left central incisor were noted. The patient also presented an increased overjet and a normal overbite with oval arch form both upper and lower (Figures 6A and B).

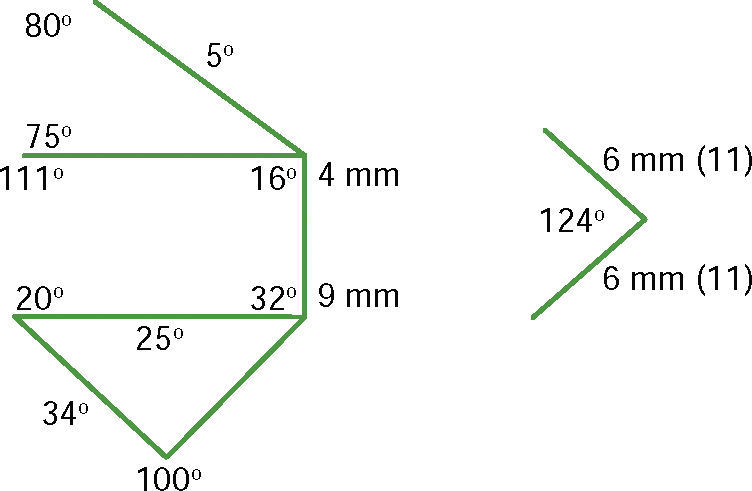
Steiner's cephalometric analysis was taken as reference (Figure 7).
TREATMENT PLAN
One of the options considered for the treatment of this patient was removing four first premolars. However, premolar extractions would imply an increased treatment time due to the necessary anchorage loss of the posterior segments. Therefore it was decided to perform the extraction of the right and left upper premolars and a lower left central incisor (31) due to the presence of a periodontal condition. 0.022” slot MBT appliances were placed. The alignment and leveling phase was carried out with 0.016”, CuNiTi archwires, 0.019” x 0.025” CuNiTi and 0.019” x 0.025” SS archwires.
TREATMENT PROGRESSIn the facial photographs it may be observed that the patient continues to have a mild facial asymmetry, the interlabial opening improved and the buccal corridors were reduced (Figures 8A and B).
INTRAORAL PROGRESS PHOTOGRAPHS
In the intraoral photographs the complete appliance placement including second molars may be observed. After the alignment and leveling stage the initial CuNiTi archwires were changed for 0.019” x 0.025” stainless steel archwires. A better alignment is evident: the upper dental midline is centered (Figure 9) and a better archform (Figure 10).


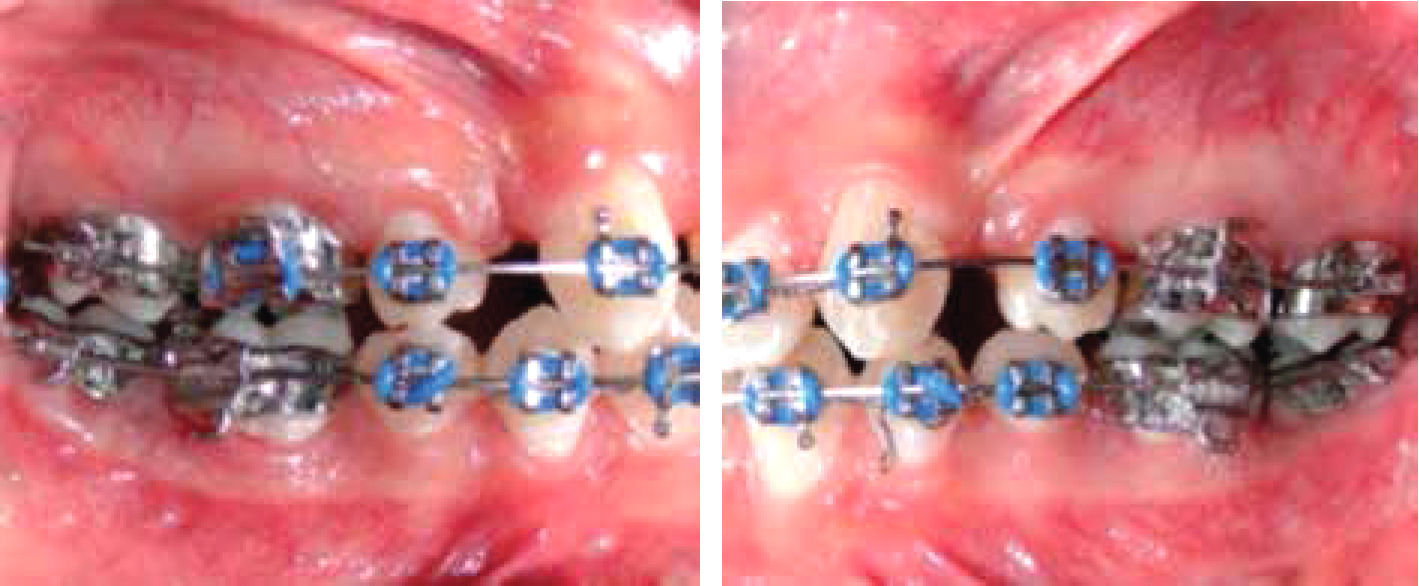
In the right and left lateral photographs a bilateral functional molar class II and canine class I may be observed although the extraction spaces have not yet been closed (Figure 11).

In the progress radiographic studies it may be observed that the patient continues to be class II with hyperdervergent growth (Figure 12).

In the panoramic radiograph after 6 months, some radicular convergences and divergences were evident and it was decided that some brackets needed repositioning. At this time the patient was referred for 3rd molar surgery (Figure 13).
TREATMENT RESULTS
Centric relation was coincident with centric occlusion in functional molar class II. In the final photographs the closed spaces may be observed; a functional molar class II was achieved due to the extractions of upper premolars, canine class I was achieved as well as a normal overbite and overbite. The profile remained harmonic. Treatment time was 18 months (Figures 14A andB).


The patient underwent upper premolar extractions in order to improve the archform, which was accomplished. Sliding mechanics was facilitated due to the technique.6
DISCUSSIONThe extraction of an incisor is an effective treatment in patients with mild crowding and combined with premolar extractions, it may improve the increased overjet. Anchorage loss was easier since no extractions were performed in the lower arch, hence, space closure mechanics were focused on the upper arch through sliding mechanics which may be achieved in a short period of time. Treatment time was 1 year 6 months and for retention, aesthetic front Hawley plaques were used daily to improve occlusal settlement. After this time period, retainer use was recommended by night only for another year.
CONCLUSIONSIncisor extraction is an effective method for correction of malocclusions compared to conventional mechanics in cases where premolars extractions would inevitably have been performed as well as retraction of the anterior segment for crowding correction and overbite improvement. It is a therapeutic option that corrects problems quickly and effectively in patients with mild crowding and without compromising the profile.
Incisor position should be assessed carefully since in these cases, it is a better option to remove a tooth that has periodontal problems or bone loss due to its position than extract a healthy tooth. If the tooth is compromised this option may be the best choice. One of the biggest advantages in carrying out this alternative is that it decreases treatment time.
A disadvantage of this kind of treatment is that the lower dental midline will not be centered with the facial midline at the end of treatment, however the overjet remains normal.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia